19 Disorders of the Eustachian Tube
More than just an anatomic conduit, the eustachian tube is a dynamic link between the middle ear and the nasopharynx. It is important in the role of aeration and drainage of the middle ear and essential for the optimal conduction of sound. This chapter offers a comprehensive overview of the anatomy, physiology, pathology, and treatment options currently available for disorders of the eustachian tube.
History
The eustachian tube was first noted by Alcmaeon of Croton around 500 bc.1 It was described in detail in 1562 by the Italian anatomist Bartolomeo Eustachi2 and later brought to light by the Pope’s physician Giovanni Maria Lancisi in the early 1700s.3 Around the same time as Lancisi, Antonio Maria Valsalva gave the tube its eponymous name and furthered our understanding of its cartilaginous and osseous portions.1 Valsalva’s work paved the way for future researchers, notably the 19th century English otologist, Joseph Toynbee, who furthered the studies of the peritubal muscles and popularized the Toynbee test to assess tubal dilatory function.4 Toward the end of the 19th century, Adam Politzer related eustachian tube dysfunction to the pathogenesis of otitis media with effusion.
Anatomy
Overview
Measuring approximately 31 to 38 mm in length in the normal adult and approximately 21 mm in an infant,5,6 the eustachian tube is a small organ originating in the middle ear and extending to the nasopharynx. The progression of mucociliary clearance within the eustachian tube flows from the proximal middle ear cavity to the distal nasopharyngeal space.7
The eustachian tube is composed of bony and cartilaginous portions. The bony portion is lined with a layer of cuboidal respiratory epithelium,8 which begins from the middle ear orifice, and courses inferiorly through the temporal bone with a funnel-shaped lumen. It becomes progressively narrow until reaching the isthmus, the narrowest point along the tube that marks the junction between the bony portion and the cartilaginous distal two-thirds of the eustachian tube. This cartilaginous portion is composed of a single segment of cartilage, is anchored superiorly to the basisphenoid bone, and empties into the nasopharynx. The bony portion remains fixed and stays patent under normal circumstances in contrast to the cartilaginous portion of the tube, which is dynamic (particularly the distal portion) and closed at rest. The cartilaginous portion is lined by the pseudostratified columnar respiratory epithelium that is taller, more densely ciliated, and abundant in mucin-secreting goblet cells.6,9
The eustachian tube orifice can be readily identified just posterior to the inferior turbinate by locating the torus tubarius, also known as the posterior cushion, which contains the mobile medial cartilaginous lamina (Fig. 19.1A). The lateral cartilaginous lamina, shorter and anchored to the basisphenoid bone, is immobile. The entire cartilaginous skeleton looks like an inverted “j” hook (Fig. 19.1B). It is important not to confuse the tubal orifice with the fossa of Rosenmüller, a recess in the posterior-lateral nasopharynx just posterior to the torus tubarius and at the depth of which courses the internal carotid artery.7 Within the mid-portion of the cartilaginous eustachian tube, the mucosal surfaces of the anterolateral and posteromedial walls meet in apposition, closing the lumen in the resting position. This approximately 8-mm long section is termed the functional “valve” and is composed of the mucosa, submucosa, Ostmann fat pad, lateral cartilaginous lamina, and the relaxed bulk of the tensor veli palatini muscle.
Peritubal Muscles
The four peritubal muscles are the tensor veli palatini, the levator veli palatini, the tensor tympani, and the salpingopharyngeus. The principal dilator muscle is the tensor veli palatini, and it is innervated by the mandibular division of the trigeminal nerve.10 The tensor veli palatini originates from the basisphenoid bone and is composed of two bundles of muscle fibers. They course anteriorly and inferiorly and converge in a tendon that runs under, or at times inserts into, the hamulus of the medial pterygoid processes before inserting into the soft palate. The dilator tubae portion of the tensor veli palatine originates directly along the anterolateral membranous wall of the eustachian tube and is important for active tubal dilation as well as tubal closure.9
The levator veli palatini is important for elevating and supporting the soft palate and the torus tubarius throughout eustachian tube dilation. It originates in the base of the temporal bone, runs along the floor of the eustachian tube, inserts into the soft palate, and is supplied by the vagus nerve.3 The tensor tympani arises from the cartilaginous portion of the eustachian tube and attaches to the malleus in the middle ear cavity. The salpingopharyngeus appears to depress the floor of the lumen to facilitate dilation. It originates in the medial and inferior borders of the cartilaginous eustachian tube and inserts into the palatal musculature.
There are several anatomical differences in the pediatric eustachian tube compared with adults that may play a role in the pathogenesis of otitis media. In children, the eustachian tube is of considerably shorter length with a narrower lumen and is more compliant, is more horizontally oriented, and contains more luminal mucosal folds (Table 19.1).9 The anatomy of the eustachian tube in children may predispose them to reflux of nasogastric contents, allergic or other inflammatory mediators, and various pathogens.
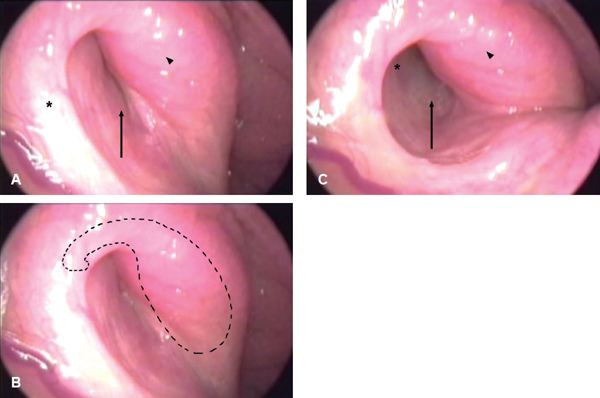
Figure 19.1 (A) Normal right eustachian tube in the closed position showing the torus tubarius (arrowhead), orifice (arrow), and anterolateral wall (asterisk). (B) Right fibrocartilaginous eustachian tube skeleton (dashed outline). (C) Normal right eustachian tube in the fully dilated position showing the torus tubarius (arrowhead), orifice (arrow), and lateral cartilaginous lamina (asterisk).
Physiology
Eustachian Tube Dilation and Closure
Tubal dilation generally occurs in two distinct phases. Dilation begins with palatal elevation partly owing to the contraction of the levator veli palatini muscle, which also results in medial rotation of the torus tubarius and the posteromedial wall of the cartilaginous eustachian tube. The levator veli palatini remains contracted throughout the tubal dilation cycle and serves as a scaffold against which the tensor veli palatini subsequently acts. The second phase of tubal dilation involves contraction of the tensor veli palatini, which actively dilates the eustachian tube’s functional valve with a lateral traction force on the anterolateral membranous wall. Full contraction of the tensor veli palatini results in maximal opening of the valve and creates a rounded lumen (Fig. 19.1C). It is important to note that tubal dilation propagates from the nasopharyngeal opening toward the isthmus of the eustachian tube in a distal-to-proximal direction, with closure proceeding in the opposite direction. The opposing mucosal surfaces of the cartilaginous eustachian tube contact one another to create an air- and water-tight seal. Adequate ventilation of the middle ear space requires that dilation of the functional valve is not wide to permit air flow and frequent to maintain air pressure at near ambient levels. Tubal dilation occurs approximately 1.4 times/min throughout the day, lasts approximately 400 ms, and substantially decreases during sleep.11,12
Middle Ear Gas Exchange
Exchange of middle ear gases with venous gases results in an overall lower net pressure in the middle ear. The most important and abundant of these is nitrogen and the resultant nitrogen gradient. Consequently, the nitrogen gradient is believed to play an important role in the long-term effects of negative pressure in eustachian tube dysfunction. The eustachian tube dilates by voluntary actions such as yawning and swallowing and by autonomic reflex stimulation secondary to alterations in gas composition and pressure that are detected by baroreceptors and chemoreceptors (Fig. 19.2).13,14
Anatomical Features of the Eustachian Tube and Middle Ear | Infant Anatomical Features Compared with Adult |
Length of tube | Shorter length |
Angle of tube relative to the horizontal plane | 10 degrees in infants versus 45 degrees in adults |
Angle/length of the tensor veli palatini to tubal cartilage | Variable angle and shorter muscle attachment in infants versus stable angle in adults |
Luminal area and volume | Smaller area and volume |
Cartilage volume | Less cartilage volume |
Cartilage cell density | Greater cell density |
Elastin at the hinge portion of the cartilage | Less elastin |
Ostmann fat pad | Relatively wider fat pad |
Mucosal folds | Greater folds |
Luminal glands | Variable types of glands |
Connective tissue located lateral to the tube | Different |
Middle ear volume | Smaller volume |
Source: Charles D. Bluestone, MD. Eustachian Tube: Structure, Function, Role in Otitis Media. Shelton, Connecticut: People’s Medical Publishing House; 2005; Table 3.2.
Clearance of the Middle Ear
The distal cartilaginous portion actively transports secretions, fluids, and debris toward the distal nasopharyngeal opening of the tube.2,15 However, in the presence of extremely viscous secretions, mucociliary clearance may be hindered. Surfactants help reduce surface tension within the lumen of the eustachian tube, effectively aiding mucociliary clearance, tubal dilation, and exchange of gases across the mucosal barrier.16,17
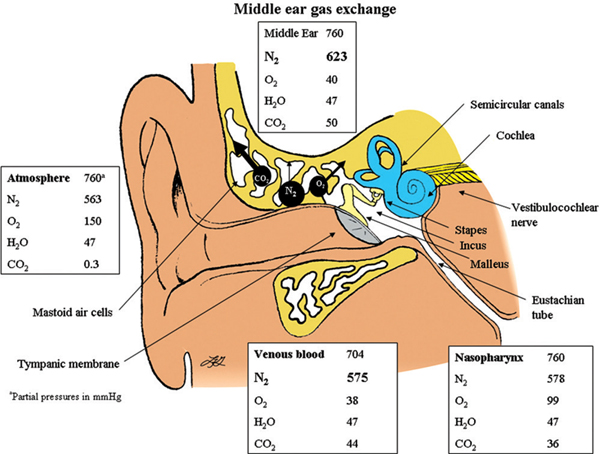
Figure 19.2 Middle ear gas exchange.
Printed with permission from: Sade J, Ar A. Middle ear and auditory tube: middle ear clearance, gas exchange, and pressure regulation. Otolaryngology-Head and Neck Surgery 1997;116(4):499–524
The muscular pumping action during tubal closing serves as an additional and synergistic means of tubal clearance. At the end of tubal dilation, as the eustachian tube progressively closes in a proximal-to-distal direction, an expelling force is generated by the relaxing cartilage and peritubal muscles.15
Protection of the Middle Ear
The functional valve of the eustachian tube protects the middle ear against the reflux of sounds and material from the nasopharynx and below.2 During the brief periods of intermittent tubal patency, the existing air pressure within the middle ear and the mastoid cavity provides a gas cushion that further inhibits the reflux of material from reaching the middle ear.12
Evaluation of the Eustachian Tube
History and Physical Examination
A comprehensive history and physical examination are the first steps toward evaluating patients. Patients should be questioned about inflammatory disorders such as allergies, laryngopharyngeal reflux, Samter triad, and sinusitis. In the pediatric population, it is important to additionally inquire about recurrent otitis media, persistent or recurrent respiratory infections, smoke or wood stove exposure, daycare attendance, and immune deficiency.18 Eustachian tube disorders can also be familial. Ciliary motility disorders, such as Kartagener syndrome and cystic fibrosis, are also important to note. Tobacco use or smoke exposure can negatively affect mucociliary clearance. It is important to note relevant surgical history such as tympanostomy tube placements or adenoidectomy. Medications, especially nasal preparations of topical corticosteroids and oxymetazoline, medications for allergies, oral contraceptives, and any hormonal replacement therapies should also be noted.
Physical examination includes a comprehensive head and neck evaluation with otoscopy or micro-otoscopy assessment. The external auditory canal, tympanic membrane, and middle ear pressure status are important to assess. Eustachian tube dilatory dysfunction is often associated with negative pressure in the middle ear, so it is crucial to look for tympanic membrane retraction, retraction pockets, effusion, perforations, tympanosclerosis, or cholesteatoma. Tympanic membrane lateral and medial excursions with breathing will likely indicate a patulous eustachian tube. Retractions surrounded by mobile tympanic membrane may indicate a past history of tubal dilatory dysfunction. A tympanogram and audiogram should be obtained to determine the resting middle ear pressure and hearing.
Endoscopic Examination of the Eustachian Tube
High-quality endoscopy by using a Hopkins rod or a flexible endoscope has become an invaluable tool for evaluating the eustachian tube. The initial examination should assess the nasal mucosa, nasopharynx, pharynx, larynx, hypopharynx, and subglottic space for signs of inflammation or underlying allergy, granulomatous, laryngopharyngeal reflux, or other diseases.19
When examining the eustachian tube with a flexible endoscope, the optimal view into the depths of the tubal lumen may often be obtained by advancing the endoscope through the contralateral naris, passing it behind the vomer, and positioning it close to the nasopharyngeal orifice. To best inspect the mucosal folds within the tubal valve during swallowing and yawning, the endoscope should be directed down the longitudinal axis of the lumen, approximately 45 degrees superior to the floor of the nasal cavity. When examining with a rigid endoscope, 4-mm scopes with a 30 or 45 degrees viewing angle are ideal. The scope should be directed laterally and, on successful recognition of the orifice, rotated superiorly.20 The resting torus tubarius and tubal orifice is expected to have a convex s-shaped appearance. Signs of edema or hypertrophy with diminished tubal dilation are often seen with dilatory dysfunction.21
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


