Disorders of the Auricle
Benjamin D. Liess and William C. Kinney
The external ear is a unique part of the human sensory system. Its structure, prominent position, and complex function predispose the auricle to disorders not seen in other parts of the human body. Congenital defects of the auricle result from disruption of complex developmental events and may lead to many combinations of both external and middle ear disorders. The prominent position of the ear makes it more susceptible to both mechanical and thermal trauma and also affects how the auricle heals from the trauma. A unique set of local infectious and systemic diseases manifests in the ear and may represent a primary process or an associated finding. Multiple dermatologic conditions involve the auricle and should be treated as part of the general dermatologic illness. In addition to systemic infectious etiologies, both immunologic and metabolic disease states may develop auricular manifestations. The auricle is also subject to various neoplastic processes. This chapter assists the otolaryngologist in recognizing and understanding the various disease entities that can involve the auricle.
 Congenital Disorders of the Auricle
Congenital Disorders of the Auricle
Congenital disorders of the auricle involve a wide range of deformities, each requiring a different surgical approach for correction. Rogers1 classified these defects in descending order of severity in terms of deformity: microtia,2 lop ear,3 constricted ear, and prominent or protruding ear.4 Weerda2 combined the classification systems of Rogers and Tanzer and expanded on this classification by correlating the defect with degree of developmental dysplasia (Table 15–1). Other findings not seen in these classification systems include preauricular pits and sinuses as well as preauricular appendages.
Heredity is a factor in specific defects. Preauricular pits and sinuses appear to be dominant characteristics in some families.3 Deafness and auricular deformities have been reported as characteristics of both dominant and recessive genetic disorders. For example, ear deformities occur in families of patients with mandibulofacial deformities such as Treacher-Collins syndrome.4 Additionally, the incidence of microtia may vary among ethnic groups. In one series by Harris et al,5 the incidence was estimated to be 1 to 3 per 10,000 live births. In contrast, the incidence of microtia is estimated to be 1 in every 4000 live births among the Japanese and 1 in every 900 to 1200 among Navajo Native Americans.6
| Constricted ear (cup or lop), cryptotia |
| Prominent ear (first-degree dysplasia) |
| Hypoplasia of superior third of auricle (first-degree dysplasia) |
| Hypoplasia of middle third of auricle (second-degree dysplasia) |
| Anotia (third-degree dysplasia) |
| Complete hypoplasia (third-degree dysplasia) with atresia of external auditory canal |
| Complete hypoplasia (third-degree dysplasia) without atresia of external auditory canal |
| Hypoplasia of entire superior third |
Source: Adapted from Weerda H. Classification of congenital deformities of the auricle. Facial Plast Surg 1988;5:385–388. Reprinted by permission.
The embryologic relationship of the auricle to the middle ear produces a range of concurrent defects in the middle ear and surrounding structures that must be evaluated when an auricular deformity is present. Middle ear deformities can vary from a narrow external auditory canal with minimal ossicular defects to fused ossicles with an absence of mastoid pneumatization. Specific abnormalities of the ossicles include a shortened long process of the malleus that may be attached to the anterior canal wall or complete absence; the malleus and incus may be underdeveloped or a single mass of bone; and stapes abnormalities including defects in the superstructure or even complete absence of the footplate. Facial nerve disorders can include loss of the bony fallopian canal covering, bulging of the nerve over the oval window, or running of the nerve inferior to the oval window. Changes in the tympanic bone, temporomandibular joint, mastoid, and location of dura also have been associated with deformities of the auricle.7 Additionally, children with external ear abnormalities have a mildly increased risk of concurrent renal abnormalities8 and may need to undergo a clinical genetics evaluation to screen for additional anomalies.
Microtia represents a range of findings from complete agenesis to a somewhat small ear with an atretic canal. The most common finding is a vertically oriented sausage-like or “peanut” ear (Fig. 15–1). Twice as many males are affected, with the right side being involved more often. Bilateral microtia is relatively rare but is seen frequently in patients with Treacher-Collins syndrome or bilateral craniofacial microsomia.
Constricted ear is a term coined by Tanzer9 to represent deformities in which the encircling helix is tight. This term includes the “cup ear,” which refers to an increase in the conchal bowl size (Fig. 15–2), and “lop ear,” with inferior bending of the superior helix (Fig. 15–3). Repair may involve reshaping existing tissue or require supplemental skin and supporting structures. Stahl’s ear (Fig. 15–4) represents a variant of constricted ear. It is characterized by a third crus with a flattened scaphoid fossa and deficient antihelix.
Auricular atresia results from abnormal development of the first branchial cleft (ear canal) and arch (auricle) (also see Chapter 1). Lack of recanalization of the canal occurs during the same embryologic period as ossicular formation. As expected, ossicular abnormalities are commonly associated. Children with this anomaly may develop otitis media and cholesteatoma10 with ear pain and fever. If clinical suspicion exists, computed tomography (CT) studies may delineate a pathologic process.

Figure 15–1 Peanut ear
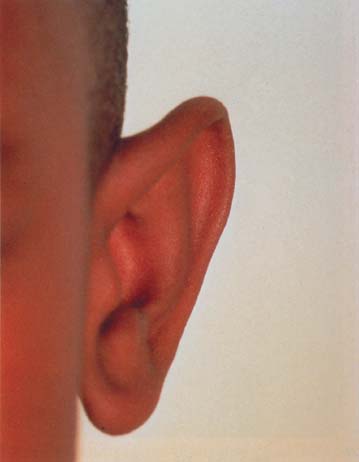
Figure 15–2 Cup ear.
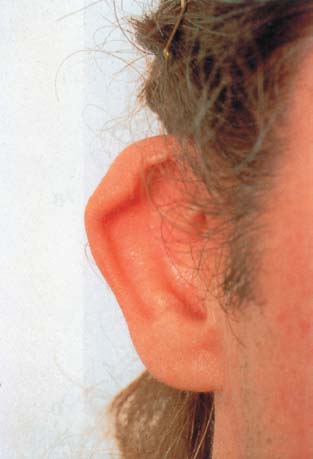
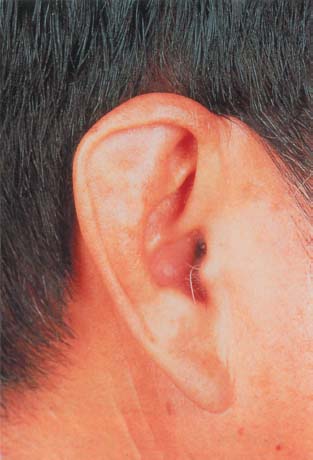
Figure 15–4 Stahl’s ear.
Cryptotia is the failure of the superior auriculocephalic sulcus to form, with the underlying cartilage buried beneath the scalp. The deformity occurs commonly in Japan, with an incidence as high as 1 in 400 births.11
Protrusion of the auricle with subsequent folding of the helix and antihelix occurs between the third and sixth month of gestation. Any interference with this process may result in a prominent ear (Fig. 15–5). Of known defects, the most common finding is failure of the antihelix to fold. Widening of the concha may also be seen. These findings are usually bilateral with a heredity influence, as they are seen in first-degree relatives.
Auricular appendages are common and result from the presence of accessory auricular hillocks. They usually appear anterior to the auricle and most often are unilateral. Skin alone or skin with underlying cartilage may be present. Children with preauricular appendages may have an associated unilateral hearing loss; therefore, complete audiologic testing may be necessary.12 These appendages may appear as part of Goldenhar syndrome. Auricular sinuses are pit-like depressions occurring in a triangular area just anterior to the auricle (Fig. 15–6). The embryologic basis for these sinuses is unclear, but is thought to be caused by failed closure of the dorsal part of the first branchial groove. Some sinuses appear to be a portion of ectoderm sequestered during formation of the auricle.13
Congenital Syndromes
Treacher-Collins syndrome (mandibulofacial dysostosis) is an autosomal dominant hereditary malformation caused by abnormal development of the first branchial arch. Deformities of the auricle are common and usually are bilateral but may be unilateral. Associated findings include auricular deformities, atresia or stenosis of the external auditory canal, middle ear anomalies resulting in a conductive hearing loss, lower eyelid notching, diminished nasofrontal angle, cheek flattening, mandibular hypoplasia, palatal defects, and dental anomalies.14,15
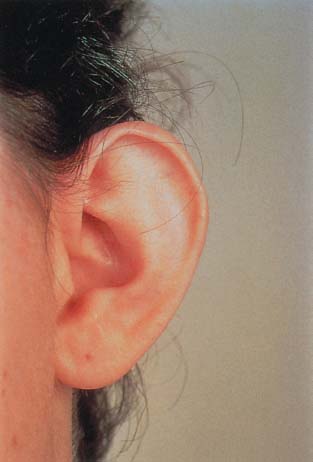
Figure 15–5 Prominent ear.

Figure 15–6 Preauricular sinus.
Branchio-oto-renal syndrome (Melnick Fraser syndrome) is an autosomal dominant disorder with both branchial arch and renal anomalies. Auricular findings include preauricular sinuses or auricular appendages. Additionally, an associated sensorineural, conductive, or mixed hearing loss may exist. Although it is unclear why the association among multiple organ systems exists, it remains important for any child with branchial arch anomalies to be evaluated for concurrent otologic and renal deformities.16
Goldenhar syndrome (oculoauriculovertebral dysplasia) has been described as autosomal dominant, but other factors in addition to heredity may have a role. Ear findings include microtia, preauricular sinuses or appendages, and external auditory canal atresia.17
Townes-Brocks syndrome (anus-hand-ear syndrome or renal ear and radical [REAR] syndrome) is an autosomal dominant disorder with multiple abnormalities including malformations of the external and middle ear with sensorineural hearing loss, hand deformities, renal anomalies (mainly hypoplastic kidney), and anorectal malformations. Auricular findings include microtia, “satyr” or “lop” ear, and preauricular tags or pits.18
Nager syndrome (preaxial acrofacial dysostosis) is an autosomal dominant condition resulting from abnormal development of the first and second branchial arches. Characteristics of this condition include the absence of radius, radioulnar synostosis, and hypoplasia or absence of the thumbs. Acrofacial dysostosis is characterized mainly by lower lid ptosis, cleft palate, severe micrognathia, and malar hypoplasia. Auricular findings include atresia, aplasia, and dysplasia of the auricle, along with multiple deformities of the external, middle, and internal ear with related hearing loss.19
Miller syndrome (postaxial acrofacial dysostosis) is an inherited disorder characterized by distinctive craniofacial malformations that occur in association with abnormalities of the outer aspects of the forearms and lower legs. Craniofacial malformations may include malar hypoplasia, micrognathia, cleft lip and palate, “cup-shaped” ears, and ectropion.20
Surgical Correction
The need for surgical correction of a congenitally malformed auricle is based on multiple variables including, but not limited to, the severity of deformity, associated middle ear anomalies, unilateral versus bilateral involvement, and the degree of inner ear function. The immediate role of the otologist is to assess hearing and select an appropriate hearing aid. In the newborn, auditory brainstem response testing is performed. In the older child, a combination of auditory brainstem response testing and behavioral audiometry is employed. Jahrsdoerfer and Hall21 recommend a CT scan after age 3 years to evaluate the middle ear structures. Glasscock and colleagues22 obtain plain films in the infant to assess bony atresia of the external auditory canal, portions of the labyrinth and cochlea, and internal auditory canal. They reserve CT scan for the older child. In the case of auricular atresia, intraoperative facial nerve monitoring to identify the commonly aberrant nerve is recommended to help prevent iatrogenic facial paralysis.23,24
Disagreement exists whether the malformed auricle or atretic external auditory canal should be repaired first. The reconstructive surgeon believes that repairing the auricle after the atresia decreases cartilage viability because of changes in blood supply and scarring resulting from previous surgery. The otologist would first correct the atresia, believing that proper positioning of the new auricle is dependent on appropriate placement of the new external auditory canal. Investigation has shown that a reconstructed auricle can be repositioned successfully with careful soft tissue elevation,4 but this additional procedure is avoidable if the atresia is addressed first. Timing for surgical correction of the deformity also is controversial. In patients with unilateral microtia and a normal opposite ear, Glasscock and colleagues22 prefer to wait until the patient is age 18 and able to make a decision based on the risks and benefits involved. Jahrsdoerfer and Hall21 perform most of the repairs on patients between the ages of 4 and 6 years. Brent4 suggests that optimal timing for unilateral repair is when the patient is 6 to 7 years old, after the rib cartilage has matured and the child can perform postoperative care. Exceptions for postponement of auricular repair in unilateral cases include cases of a chronically draining fistula involving the ear or extensive cholesteatoma. For bilateral microtia, Jahrsdoerfer and Hall suggest repair of at least one side before the child starts school.
 Auricular Trauma
Auricular Trauma
Auricular trauma can result from blunt, penetrating, or thermal injury. The auricle is susceptible to such trauma because of its prominent and unprotected position. Unlike the eyes, the auricle has no reflex to protect against impending injury. In addition to immediate damage from the traumatic event, complications of auricular trauma such as chondritis with loss of cartilage support can be cosmetically deforming.
Often, auricular trauma will require surgical reconstruction. In most cases, prophylactic antibiotics and tetanus prophylaxis are warranted. Photographs or drawings may be helpful for planning a repair and documenting the extent of injury. In a multitrauma patient, stabilization and treatment of other injuries take precedence over auricular trauma.
Blunt Trauma
Shearing forces occurring with blunt trauma may produce an auricular hematoma (Fig. 15–7). Commonly seen in wrestlers and boxers, this hematoma forms when blood vessels of the perichondrium are traumatically separated from their underlying cartilage. Additional accumulation of blood further separates the perichondrium from the cartilage. Because cartilage receives oxygen and nutrients solely from the perichondrium, this separation may result in cartilage necrosis. Early treatment is necessary to prevent growth of ectopic fibrinocartilage from the perichondrium, resulting in a thickened external ear or “cauliflower ear” (Fig. 15–8). The pathogenesis of auricular hematoma has been studied and confirmed in an animal model.25
Auricular hematoma originally was treated with repeated 196 aspirations and bandaging, but unfortunately such treatment often resulted in a thickened auricle. Current methods for treatment include aspiration followed by pressure dressing involving a plaster mold26 or reinforced collodion dressing,27 anterior auricular incision with cartilage fenestration and hematoma evacuation,28 postauricular incision with resection of cartilage and hematoma evacuation followed by cotton bolster dressings29 or through-suturing,30 and continuous portable suction drainage.31,32 Schuller and associates33 describe a technique of incising the hematoma, removing the clot, debriding any compromised cartilage, and then suturing dental rolls in place to bolster and reshape the auricle. This technique is technically simple and highly reliable. Antibiotic ointment and oral antistaphylococcal antibiotics commonly are prescribed. Bolsters are removed in 7 to 14 days. The advantage of this technique is that the patient may return to work or to sports activities with protective headgear the next day.

Figure 15–7 Auricular hematoma.
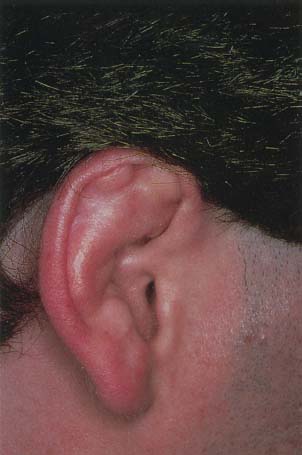
Figure 15–8 Cauliflower ear.
In the event of late treatment where fibrinocartilage has formed, the old clot and growth of new cartilage can be excised along with auricular skin until a normal contour is achieved as compared with the other ear. The ear can be repaired successfully with minimal distortion of normal tissue.28 Fortunately, such extensive deformity has become a rarity. Generally these procedures are without risk; however, hematoma may reaccumulate or infection may be introduced prompting initiation of antibiotics.
Lacerations and Abrasions
Lacerations of the auricle may range from a simple laceration requiring primary closure to complete avulsion. The auricle, like the face, has excellent blood supply and heals remarkably well. Proper surgical technique with atraumatic handling of tissue, minimal debridement, realignment of known anatomic landmarks, and meticulous approximation of tissue edges will provide the best results. If cartilage exposure occurs, the risk of infection increases and antibiotic prophylaxis may be required.
Simple Lacerations
Approximation of the cartilage, perichondrium, and skin edges is required for a good result. Some prefer to avoid direct suturing of cartilage and believe that only approximation of the skin is required, citing concerns of weakening of the structural integrity.34 Appropriate sutures include a through-and-through nonabsorbable stitch to approximate all three layers or a figure-of-eight closure of perichondrium and cartilage using an absorbable suture and simple skin closure. Advantages of the latter approach include better stabilization of the cartilage with no overriding of repaired edges and better approximation of auricular skin. If perichondrium-to-perichondrium suturing is employed, some cartilage may have to be removed.
Complex Lacerations
The same principles of repair apply to complex lacerations. However, because the laceration is complex, correct alignment of the fragments may be difficult. Temporary sutures may be helpful in realigning auricular landmarks. Debridement may be necessary to create adequate margins for reapproximation but should be kept to a minimum.
Abrasions
Abrasions of the auricle can result from a motorcycle or bicycle accident or another event resulting in a dragging injury across the ground. These wounds are contaminated and may have embedded debris. Persistent, gentle scrubbing can be used to clean the ear and remove dirt and particulate matter. The auricle should be covered with an antibiotic-impregnated gauze and a pressure dressing applied for 24 hours. Local wound care is employed after the dressing is removed to allow for reepithelialization.
Partial Tissue Loss
Partial tissue loss includes avulsions of the skin alone or full-thickness loss of the auricle. If the avulsion results in skin loss only with preservation of the perichondrium, then a split- or full-thickness skin graft may be applied directly. Potential donor sites include the upper eyelid or the cranial surface of the auricle. When trauma to skin and perichondrium involves the concha or antihelix, cartilage may be removed and a skin graft placed directly on the posterior perichondrium. This cartilage removal will not result in loss of support. When skin and perichondrium loss involves other parts of the auricle, pedicled flaps of postauricular skin may be used. For larger defects, a temporoparietal fascia flap may be used with a split-thickness skin graft.35
Full-thickness loss of the helix of less than 2 cm can be converted to a wedge repair with primary closure. Cupping of the auricle may result, but this can be corrected at closure with the excision of side triangles at the apex of the wedge. Larger defects of the marginal rim can be repaired with a chondrocutaneous advancement flap as described by Antia and Buch36 or with a modified Antia-Buch repair.37 Skin and cartilage are incised laterally with undermining of skin medially to allow for advancement of the helical rim. Some defects may require bringing additional material into the defect to minimize the decrease in ear size. Options include advancement flaps from adjacent areas with cartilage grafting and staged procedures with implanting of the exposed cartilage in the postauricular skin. Further reconstruction with a cartilage graft occurs during a second procedure.
Auricular Avulsions
Near-total or total avulsion of the auricle may be seen with animal or human bites, knife injuries, or motor vehicle accidents. Careful debridement of devitalized tissue along with wound cleaning and irrigation should occur with each case. Successful reattachment usually is more cosmetic than reconstruction. If the avulsed segment remains partially attached, an attempt should be made to regain position. In these situations, the blood supply may be adequate for partial or complete repair.
Reattaching the avulsed segment as a composite graft often results in various degrees of venous congestion and requires blood thinning agents to decrease clotting and improve blood flow.38 Multiple stab wounds or medicinal leeches38 also may improve tissue survival. Mladick et al39 described a “pocket principle” for the treatment of auricular avulsions where the skin of the avulsed segment is dermabraded and reattached in its correct anatomic position. The auricle then is buried beneath a postauricular incision or “pocket.” After 10 to 14 days, the auricle is removed from the pocket and allowed to reepithelialize.
Microvascular replantation of near total or total auricular avulsion is an effective surgical option. Anastomosis to the superficial temporal vessels either directly or via vein graft was first described by Pennington et al.40 Although a technically challenging procedure, successful operation with excellent aesthetic outcome has been reported, even in unfavorable cases.41–45 These authors describe the necessity of meticulous dissection and careful handling of tissue during direct vessel anastomosis and venous graft repair to avoid complications. As with the composite graft technique, blood thinners and medicinal leeches may assist with ear perfusion and subsequent neovascularization and healing.
In the event of complete avulsion, the avulsed segment should be transported in a cold, sterile container, and reattached as soon as possible. If the ear cannot be saved, then an auricular prosthesis held in place by osseointegrated implants or total auricular reconstruction may be needed.
Animal bites require special consideration not seen with other forms of trauma. Documentation of what type of animal, when the injury occurred, status of tetanus immunization, and rabies status of the animal should be completed as part of the initial evaluation. Photo documentation of animal bites may be needed in the event that legal action is taken by the injured party.
All animal bites to the auricle require debridement, irrigation, and prophylactic antibiotics along with a 24-hour checkup. Common organisms seen with both human and nonhuman bites are listed in Table 15–2. A majority of wounds contain both aerobic and anaerobic organisms. Careful cleaning and wound irrigation is required. Surgical repair follows the principles outlined above. Stucker and colleagues46 recommend delayed repair of severe or older human bites to allow for initial antibiotic treatment to decrease the degree of bacterial presence from the traumatic inoculation. For the uncomplicated injury less than 5 hours old, they recommend primary repair. If delayed repair is chosen, local wound care should be employed until the wound is clean and shows signs of granulation tissue formation.
Thermal Injuries
Frostbite
Frostbite is a localized injury resulting from exposure of tissue to subfreezing temperatures (Fig. 15–9). Frostbite injury may be divided into four degrees. First degree presents with edema and erythema and in approximately 1 week the superficial skin layers slough. Second degree begins with the development of blisters and may progress to bulla formation. Upon desiccation of the blisters an eschar will form; when the eschar sloughs, healthy tissue will appear. Third degree consists of dermal and possible subcutaneous tissue damage resulting in an eschar that may take months to heal. Fourth degree presents with damage to the deeper tissues and underlying bone, which often leads to tissue necrosis, gangrene, and autoamputation. The extent of injury depends on the duration of exposure, temperature, and whether contact with metal, moisture, or protective ointment occurs.47

Figure 15–9 Frostbite pinna.
Tissue loss is caused by direct cellular and vascular injury. At a cellular level, chondrocytes show a greater degree of devastation compared with epidermal cells. Vascular injury results from separation of the vascular endothelium from the underlying lamina, thought to be caused by ice crystal formation.48 Resultant tissue necrosis then is caused by erythrocyte extravasation, interstitial edema, and decreased blood flow. Endothelial cells at the injury site release chemical mediators, including arachidonic acid metabolites, which directly stimulate contraction of vascular and nonvascular smooth muscle, modulate platelet aggregation, and influence histamine release.49
Treatment of auricular frostbite first requires rapid rewarming of the affected tissue. Wet cloths at 38° to 42°C are applied to the ear and changed as needed until the ear is thawed.50 The auricle should be kept clean and both physical pressure upon the ear and vasoconstrictors should be avoided. Prophylactic antibiotics are recommended and early debridement generally is discouraged because several months may be required to assess the extent of self-healing. Heggers and colleagues51 recommend debridement of blisters because they contain arachidonic acid metabolites that may further damage the auricle.
Burns
The auricle is at risk of extensive injury from a burn because of its prominent position and tissue composition. Lack of subcutaneous tissue leaves the perichondrium and cartilage with little protection. Exposed cartilage is at increased risk of chondritis (Fig. 15–10). Dowling et al52 estimated that infection occurred in up to 25% of auricular burns.
Burn injury is classified as first, second, and third degree. First-degree (superficial) burns involve only the epidermis and present with erythema, warmth, and no blisters, and are painful to touch. Minimal treatment is needed. Second-degree (partial-thickness) burns involve the epidermis and part of the dermis and appear red, blistered, and may be swollen and painful to touch. They can be further classified as superficial or deep, depending on the amount of dermis involved. Third-degree (full thickness) burns involve the epidermis and dermis and appear erythematous, mottled, white, brown, or charred, and lack all but deep sensation. Local tissue loss may result from both direct heat injury and tissue ischemia. Ischemia is due to both increased vascular permeability to fluid from platelet microthrombi damage to small vessels, and release of chemical mediators similar to those seen in frostbite injury.
Treatment of auricular burns is similar to treatment of burns in other locations. This treatment may be remembered with the six C’s of care: (1) remove clothing, (2) cool the burn, (3) clean the burn site, (4) chemoprophylaxis with tetanus immunization, (5) cover the burn site with appropriate dressings, and (6) comfort the patient with analgesics. Topical mafenide acetate (Sulfamylon) cream is recommended due to excellent eschar and cartilage penetration along with clinical efficacy in reducing the incidence of chondritis. Exposed cartilage must be covered with vascularized tissue. A complication of cartilaginous involvement in burn injury is suppurative chondritis, commonly caused by Pseudomonas aeruginosa. In chondritis, appropriate antibiotics may be given intravenously or by direct injection into the ear multiple times each day, in addition to topical application of Sulfamylon cream. Principles of reconstruction described for avulsion may be used to correct any resulting defect.

 Infections of the Auricle
Infections of the Auricle
Infections of the external ear include primary infections of the auricle and infections of the external auditory canal. This discussion focuses on infections of the auricle but includes those processes that may overlap with the external auditory canal. Infections of the external ear may be primary or secondary to underlying disease or injury.
Bacterial Infections
Impetigo
Impetigo is a highly contagious superficial spreading infection involving the superficial layers of the epidermis. Impetigo of the auricle commonly occurs when an infection of the lateral external auditory canal and concha extends to the auricle. The clinical presentation may be bullous or nonbullous. Bullous impetigo presents with rapidly appearing superficial clusters of fragile blisters or large bullae. Rupture of the blisters produces a raw area surrounded by a ragged fringe of epidermis called a “collarette of scale.”53 Lymph nodes are not frequently involved. Bullous impetigo is commonly caused by Staphylococcus aureus, which has been cultured from blisters. Nonbullous impetigo (impetigo contagiosa) presents a single erythematous macule that becomes vesicular and easily ruptures, leaving a “honey-colored” crust over the erosion. This commonly expands into surrounding areas and may have associated local lymphadenopathy.54 Some disagreement exists concerning the causative agent, but most concur that staphylococcal organisms are responsible for cases in temperate climates and streptococcal organisms for those in tropical environments.53 The ear may be autoinoculated when children scratch the external meatus after touching another affected area of the body.
Before initiating antibiotic treatment, wound cultures should be obtained. Local wound care is appropriate in addition to topical antistaphylococcal agents, including mupirocin, which have been proven equally effective as oral agents.55,56
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


