Fig. 11.1
A patient with differentiated thyroid carcinoma of the left thyroid lobe with bilateral cervical lymph nodal metastases demonstrated by fine-needle cytology. Ultrasonography demonstrates multiple nodules with irregular margins in the left thyroid lobe (a, b), cystic left cervical lymph nodes (c), and solid right cervical lymph nodes (d)
Fig. 11.2
A patient with differentiated thyroid carcinoma of the right thyroid lobe with cervical lymph nodal metastasis demonstrated by fine-needle cytology. Ultrasonography demonstrates a large nodule in the right thyroid lobe with irregular margins and inhomogeneous echotexture (a, b) and an enlarged right cervical lymph node (c) with increased vascularity at Doppler ultrasonography (d)
Primary differentiated thyroid carcinoma or metastases from this tumor may also be incidentally detected by several diagnostic imaging methods (Figs. 11.3, 11.4, 11.5, and 11.6).
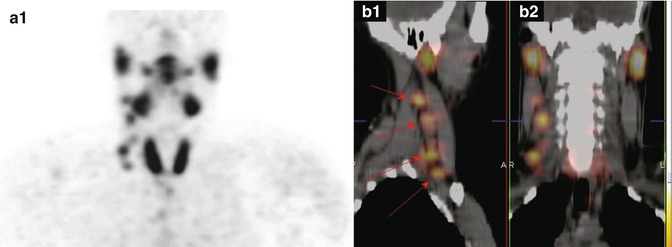
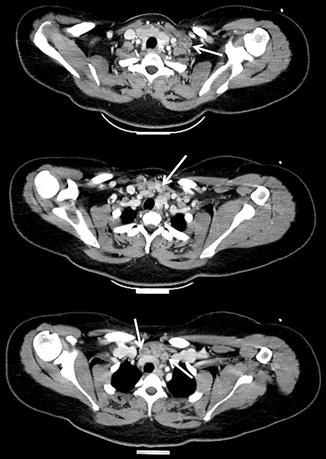
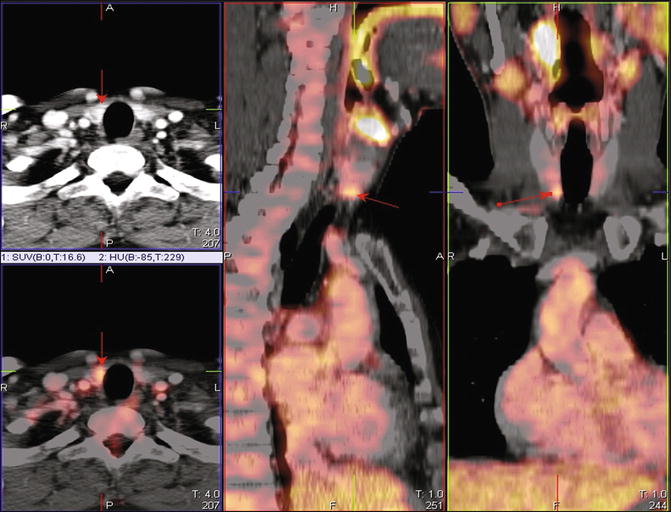
Fig. 11.3
Right cervical lymph nodal metastases of differentiated thyroid cancer detected by 99mTc-MIBI scintigraphy both at planar (a) and fused tomographic single-photon emission computed tomography/computed tomography (SPECT/CT) images (b1, b2, arrows)
Fig. 11.4
Cervical and upper mediastinal metastatic lymph nodes from differentiated thyroid carcinoma detected by contrast-enhanced computed tomography (arrows)
Fig. 11.5
Differentiated thyroid carcinoma of the right thyroid lobe incidentally detected by fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT). Axial CT (upper left image) and axial (lower left image), sagittal (central image), and coronal (right image) fused PET/CT images show focal radiopharmaceutical uptake corresponding to a small thyroid nodule of the right thyroid lobe (arrows)
Fig. 11.6
Ultrasonographic findings of the same patient of Fig. 11.5. Ultrasonography (US) shows a mixed right thyroid nodule (a, arrow) with increased vascularity at Doppler US (b) and hypoechoic right cervical lymph nodes (c). Fine-needle aspiration cytology demonstrated a differentiated thyroid carcinoma with right cervical lymph nodal metastases
Sonographic features suggestive of abnormal metastatic lymph nodes include loss of the fatty hilus, a rounded rather than oval shape, hypoechogenicity, cystic change, calcifications, and peripheral vascularity. No single sonographic feature is adequately sensitive for detection of lymph nodes with metastatic thyroid cancer [1]. US-guided fine-needle aspiration (FNA) of sonographically suspicious lymph nodes should be performed to confirm malignancy if this would change the management [1].
After thyroidectomy, most patients receive ablative iodine-131 (131I) therapy, depending on the individual patient’s situation and physician preference [2, 3]. A third element of DTC treatment, levothyroxine therapy (L-T4), aims to achieve either a low-normal thyrotropin (TSH) concentration or TSH suppression, depending on the disease stage [4].
With treatment, most patients with DTC have an excellent prognosis with normal life expectancy. However, some show persistent disease after initial therapy or develop recurrent disease during follow-up [2]. Postsurgical follow-up of DTC aims to identify early the small proportion of patients with residual disease or who will develop recurrence (Figs. 11.7, 11.8, 11.9, 11.10, and 11.11).
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
