8
Diagnostic Audiology
Craig W. Newman and Sharon A. Sandridge
Coupled with the patient’s case history and physical examination, audiologic testing assists the physician in developing a medical, surgical, or rehabilitative treatment plan for patients with auditory disorders. Further, audiologic procedures may be used to quantify outcome when administered in a pre- and posttreatment protocol.
The audiologic test battery is composed of two major categories of procedures. The first group of tests involves behavioral or psychophysical techniques requiring the patient to take an active role in the test session by responding to some form of an auditory stimulus. These tests include pure-tone and speech audiometry. The second group of tests capitalizes on physiologic responses to auditory signals and does not require active participation by the patient. The latter category of relatively objective test procedures includes immittance studies, otoacoustic emissions, and auditory evoked potentials.
It may be noted by the more seasoned professional, that a discussion of the traditional behavioral diagnostic tests (e.g., tone decay, Short Increment Sensitivity Index [SISI]; Alternate Binaural Loudness Balancing [ABLB]; Bekesy Audiometry) has been omitted in this chapter. Although these tests may have some interest from an historical perspective, they hold little clinical value in today’s audiologic test battery. It is our intent to provide the otolaryngology practitioner or resident with the most essential concepts and terms underlying contemporary diagnostic audiology.
 Pure-Tone Audiometry
Pure-Tone Audiometry
Pure-tone audiometry is the most fundamental component of the audiologic evaluation. Results from pure-tone testing are used to (1) determine the severity of hearing loss; (2) diagnose the type (i.e., conductive, sensorineural, or mixed) of hearing loss by comparing air- and bone-conduction thresholds; (3) describe the configuration of hearing loss (i.e., pattern of pure-tone thresholds from low frequencies to high frequencies); (4) determine the intensity levels at which other audiologic procedures will be performed; and (5) determine the need for rehabilitative treatment.
Pure-tone audiometry is based on obtaining a series of thresholds. According to the American National Standards Institute (ANSI S3.20), threshold is defined as the “minimum effective sound pressure level of the signal that is capable of evoking an auditory sensation in a specified fraction of trials.”1 Clinically, the term threshold is defined as the lowest intensity at which the patient is able to respond to the stimulus 50% of the time (e.g., two out of four trials using a bracketing approach). For air-conduction testing, thresholds for single frequencies are assessed between octave intervals ranging from 250 Hz to 8000 Hz. When differences in thresholds of 20 dB or greater are obtained between adjacent thresholds, responses to inter-octave frequencies (750, 1500, 3000, or 6000 Hz) are determined. For bone-conduction testing, thresholds are measured at octave intervals between 250 and 4000 Hz.
Air-conduction measurements, using standard supraaural headphones or insert earphones, assess the entire peripheral auditory system including both the conductive (outer ear and middle ear) and sensorineural portions (cochlea and eighth nerve). In contrast, bone-conduction measurements are made using a bone oscillator typically placed on the mastoid prominence, although forehead placement is an alternative. Puretone signals transmitted via the bone oscillator cause the skull to vibrate, thereby stimulating the cochlea. For clinical purposes, bone-conduction audiometry is used to bypass conductive mechanisms and provide a measure of sensorineural reserve. It should be noted that tactile responses occur when signal levels are too intense, especially at low frequencies. In the latter case, patients respond to the vibration of the oscillator rather than to an auditory percept, leading to possible erroneous test results.
Clinical Procedures
Pure-tone thresholds are obtained using an audiometer that is calibrated to current ANSI specifications (ANSI S3.6) to ensure both the validity and reliability of test results.2 Regardless of the make and model, all diagnostic audiometers have the capability of presenting calibrated pure-tone stimuli for air-and bone-conduction testing and speech stimuli using monitored live voice or recorded presentations. The results from puretone testing are recorded on a form called the audiogram, with frequency displayed on the abscissa and intensity in dB HL (hearing level) on the ordinate. Fig. 8–1 shows a typical version of an audiogram and associated set of symbols used to document responses.
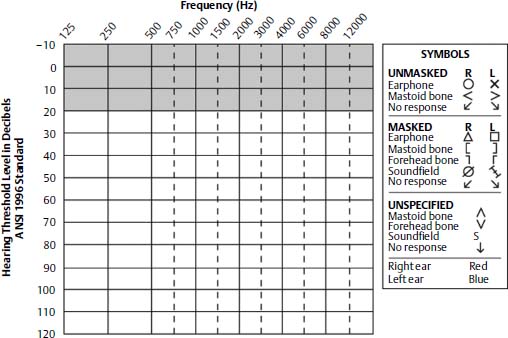
Figure 8–1 Example of an audiogram and a key of audiometric symbols.
Obtaining valid and reliable pure-tone thresholds requires a skilled examiner. Without proper control of the following variables, results may be influenced by such factors as collapsed ear canals, false-positive/negative responses, equipment calibration, ambient noise in the test environment, earphone/bone-oscillator placement, visual cues given by examiner, ear selection, frequency sequencing, instructional set, response mode (use of handheld switch versus hand/finger raise), threshold procedure, and patient rapport.3,4
Audiogram Interpretation
Magnitude of Hearing Impairment
Several schemes have been developed to classify the degree of hearing impairment based on the pure-tone average (PTA) of 500, 1000, and 2000 Hz.5 The two-frequency PTA (Fletcher average, which is the best two thresholds at 500, 1000, and 2000 Hz) is often a better predictor of hearing for speech than the three-frequency PTA. Table 8–1 shows a classification scheme that is appropriate for adults; however, it is noteworthy that losses as minimal as 15 to 25 dB HL can have negative effects on the academic performance of children.6 Calculating the PTA provides an overall estimate, albeit a loose one, of the impact a given hearing loss has on communication function.
Type of Hearing Loss
Three types of hearing loss, namely, conductive, sensorineural, and mixed, can be determined by comparing air-conduction thresholds to bone-conduction thresholds for each ear independently.
• Conductive hearing loss involves disorders of the outer ear, middle ear, or both. A conductive hearing loss is characterized by bone-conduction threshold responses obtained at 20 dB or better (reflecting normal cochlear or neural function) with air-conduction thresholds falling outside the normal limits. For illustrative purposes, the audiometric pattern for a bilateral conductive hearing loss is displayed in Fig. 8–2A. As shown, thresholds for air conduction are elevated (poorer hearing) for both ears. In contrast, masked bone-conduction thresholds fall within normal limits across the frequency range showing normal sensorineural function.
• Sensorineural hearing loss involves the cochlea, eighth cranial nerve, or both. A sensorineural hearing loss is characterized by a relatively equal (i.e., within 10 dB) elevation (i.e., poorer thresholds) of both air- and bone-conduction thresholds that fall outside the normal limits. For example, audiometric findings for a bilateral sensorineural hearing loss are displayed in Fig. 8–2B. As can be seen, both air- and bone-conduction thresholds are elevated and interweaving.
• Mixed hearing loss is a combination of a conductive and sensorineural hearing loss. Mixed hearing losses are characterized by an elevation of both the air- and bone-conduction thresholds beyond the normal limits. Yet, as illustrated in Fig. 8–2C, air-conduction thresholds are even poorer (responses present at higher intensity levels) than bone-conduction responses. The difference between the air- and bone-conduction thresholds, known as the air-bone gap, reflects the degree of the conductive component contributing to the overall hearing loss.
| PTA (in dB HL) | Category | Communication Difficulty |
|---|---|---|
| 0–25 | Normal | No significant difficulty |
| 26–40 | Mild | Difficulty understanding soft-spoken speech |
| 41–55 | Moderate | An understanding of speech at 3 to 5 feet |
| 56–70 | Moderately severe | Speech must be loud for auditory reception; significant difficulty in group settings |
| 71–90 | Severe | Loud speech may be understood at 1 foot from the ear; may distinguish vowel but not consonant sounds |
| 90+ | Profound | Does not rely on audition as primary mode of communication |
Source: Adapted from Roeser RJ, Buckley KA, Stickney GS. Pure tone tests. In: Roeser RJ, Valente, M, Hosford-Dunn, H, eds. Audiology Diagnosis. New York: Thieme, 2000;239. Reprinted by permission. HL, hearing level referring to the ANSI-1996 scale.
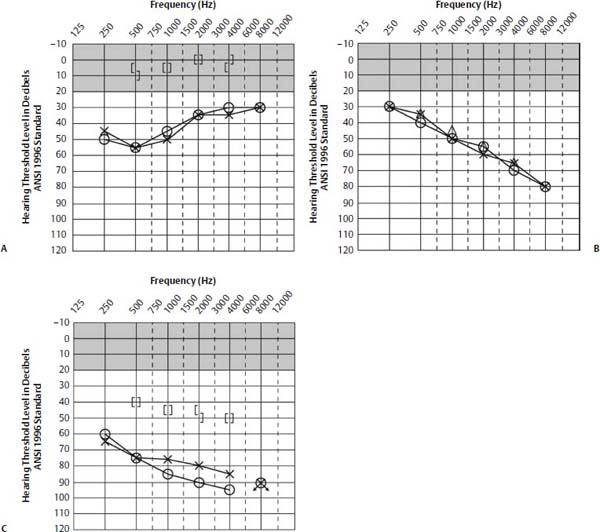
Figure 8–2 Audiometric results. (A) Conductive hearing loss. (B) Sensorineural hearing loss. (C) Mixed hearing loss.
Audiometric Configuration
A variety of audiometric configurations is used to describe patterns of pure-tone findings (Fig. 8–3). Often certain configurations are considered pathognomonic of specific otologic conditions. For example, a 4000-Hz notch is consistent with noise exposure. A rising conductive loss reflects a stiffness tilt associated with middle ear effusion. In contrast, a sloping conductive loss reflects a mass tilt associated with such disorders as ossicular discontinuity, middle ear tumor, and thickened tympanic membrane. For patients with otosclerosis, the bone-conduction threshold often is reduced at 2000 Hz. The latter finding is referred to as the Carhart notch.
 Speech Audiometry
Speech Audiometry
Results from speech audiometry are useful for (1) crosschecking the validity of pure-tone thresholds; (2) quantifying suprathreshold speech recognition, which assists the clinician in determining site of lesion; and (3) estimating communication function so that appropriate rehabilitative interventions can be recommended and outcome monitored. Although several speech tests are available, the following sections focus on the two major components of speech audiometry used routinely in diagnostic audiology, namely, the speech reception threshold (SRT) and suprathreshold word recognition testing.
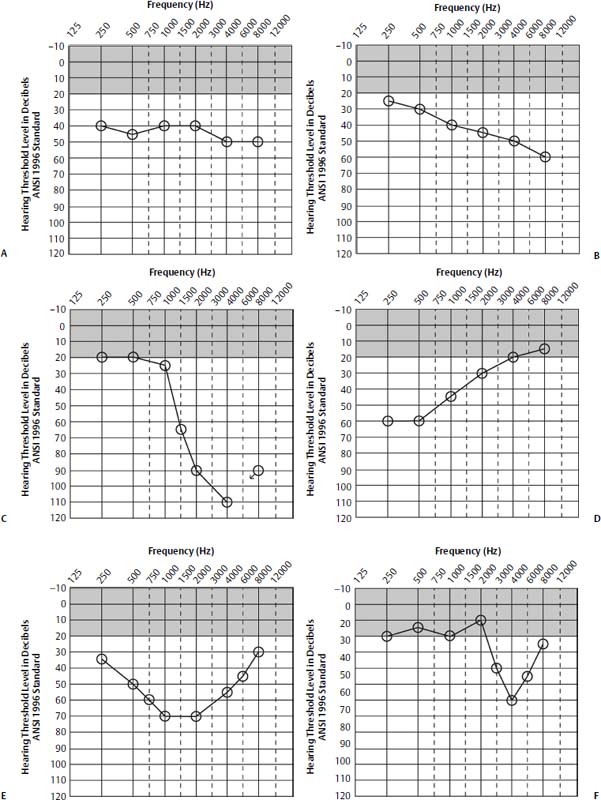
Figure 8–3 Examples of audiometric configurations used to describe the pure-tone audiogram. (A) Flat. (B) Gradually sloping. (C) Precipitously sloping. (D) Rising. (E) Trough. (F) Notch.
Speech Recognition Threshold
Similar to pure-tone thresholds, the SRT is the lowest hearing level at which the patient correctly recognizes speech stimuli 50% of the time for each ear independently. The most commonly used and recommended speech stimuli for obtaining SRTs are spondaic words.5 A spondee is a bisyllabic word with equal stress on both syllables (e.g., baseball, hotdog, airplane). Because the PTA reflects hearing thresholds in the speech-frequency region and the SRT is measured using speech stimuli, close agreement between the latter two measures is expected. Accordingly, functional hearing loss (i.e., pseudohypoacusis) should be considered whenever there is an SRT-PTA discrepancy of more than 12 dB, especially when the SRT is better than would be predicted from the PTA.7 In addition to functional hearing loss, a variety of other reasons must be considered when an SRT-PTA discrepancy exists, including (1) audiometer malfunction; (2) eighth cranial nerve disorders; (3) significant hearing loss with an island of normal hearing; and (4) cognitive or language disorders.
Word Recognition Testing
Materials and Procedures
Word recognition testing (WRT) is evaluated using monosyllabic phonetically balanced (PB) words. PB word lists contain all of the phonetic elements of connected discourse representative of everyday English speech. The most popular 50-item PB-word lists used today are the Central Institute for the Deaf (CID) Auditory Test W-22 and the Northwestern University Test No. 6.8 These word lists are presented in an “open response” format wherein the set of possible responses to a test item is open and limited only by the patient’s vocabulary. Because patients with severe hearing impairments often perform poorly on open response tests, alternative “closed response” multiple choice tests such as the California Consonant Test (CCT) have been developed.9 In addition to monosyllabic word lists, several sentence-length materials such as the Everyday Speech Sentences10 and Speech Perception in Noise (SPIN) test11 have been developed to approximate a patient’s speech understanding using contextual materials or hearing in the presence of a competing background noise.
Typically, WRT is performed at a 30- to 40-dB sensation level (i.e., above the SRT) or at the patient’s most comfortable listening level (MCL) for each ear independently. Higher presentation levels, however, may be necessary to determine the patient’s maximum word recognition score (i.e., PB Max). The evaluation of word recognition at multiple intensity levels is referred to as the performance-intensity (PI) function. For standardization purposes, it is preferable that PB word lists are presented using commercially available recordings rather than “live voice” presentations.
Scoring and Interpretation
Word recognition scores are expressed as the percentage of words correctly repeated from the 50 (full) or 25 (one-half) word lists. The obtained percent correct scores then are used in a classification scheme to estimate speech understanding ability. For example, word recognition scores of 90 to 100% are classified as excellent, 80 to 88% good, 70 to 78% fair, and below 70% is poor. It should be noted, however, that considerable variability on test-retest occurs especially as the number of test items is reduced from 50 words to 25 words, known as the “list size/measurement error trade-off.”12
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


