24 Diagnosis, Evaluation, and Management of Causes of Peripheral Incapacitating Vertigo other than Meniere Disease
There are many physiologic and pathologic causes of vertigo. For a better understanding of the pathophysiology of vestibular-induced vertigo, it is best to think of vertigo as resulting from a steady-state malfunction. The normal physiologic vestibular receptors in the bony labyrinth monitor the motion and position of the head in space by detecting angular and translational forces of the head. Inside the bony labyrinth is the perilymphatic fluid, within which there is the membranous labyrinth and its contained endolymphatic fluid. The two otolith organs, one in the utricle and one in the saccule, in each inner ear monitor linear acceleration/translational forces, including gravity. The three semicircular canals in each inner ear are detectors of angular acceleration.
The semicircular canals are positioned at near right angles to each other so that they sense movements in any and all planes in space, with the left and right sides complementing one another. Thus, there is redundancy built into this system, which is an important concept in the outcome and treatment of the disease state. Each canal is filled with endolymph and has a swelling at the base that is called the ampulla. The ampulla contains the cupula, a gelatinous mass with the same density as endolymph, which is attached to polarized hair cells.
With the head at rest, the hair cells from both labyrinths emit a steady baseline rate of discharges that induces a steady rate of vestibular nerve impulses. As long as the neural input at the level of the vestibular nuclei is equal from both labyrinths, the self-perception will be one of no (head) movement. It is the function of the vestibular end organs to modulate these steady-state signals and interact with the ocular motor system, the locomotive system, and the cognitive region of the brain to stabilize vision with head movements, maintain a stable upright posture against gravity and movement, and produce a conscious three dimensional awareness of where the head and body are in space. As always, there are feedback loops from each of these systems, and the signals are modulated further by the cerebellum.
Displacement of the neutrally positioned cupula by head turning (an angular acceleration or deceleration) causes either a stimulatory or an inhibitory response of any or all semicircular canals bilaterally, depending on the rapidity, direction and plane of the motion. It should be noted that the cupula forms an impermeable barrier across the lumen of the ampulla. This becomes important when we discuss the treatment of benign paroxysmal positional vertigo (BPPV). The term utriculofugal refers to cupular movement away from the utricle, whereas utriculopetal refers to cupular movement toward the utricle. In the superior and posterior semicircular canals, utriculofugal deflection of the cupula is stimulatory and utriculopetal deflection is inhibitory. The opposite is true for the lateral semicircular canal.
Nystagmus, one of the key manifestations and signs of vertigo, is defined as the repeated and rhythmic oscillation of the eyes. Stimulation (or inhibition) of the semicircular canals most commonly causes jerk nystagmus, which is characterized by a slow phase (slow movement in one direction) followed by a fast phase (rapid movement in the other direction). Although it is the modulated vestibular signal that induces the slow phase, the nystagmus is named according to the direction of the fast phase. The fast phase is in fact a saccade generated by the reticular activating system; this is why nystagmus is more evident during states of heightened consciousness. Nystagmus can be horizontal, vertical, oblique, torsional (rotatory), or any combination thereof and may be induced by vestibular signal asymmetries or disturbances that arise more centrally. Thus, though it may be challenging at times to differentiate peripheral from central vertigo, there are certain features and symptoms as listed in Table 24.1 that help make this distinction.
Overview of Disorders
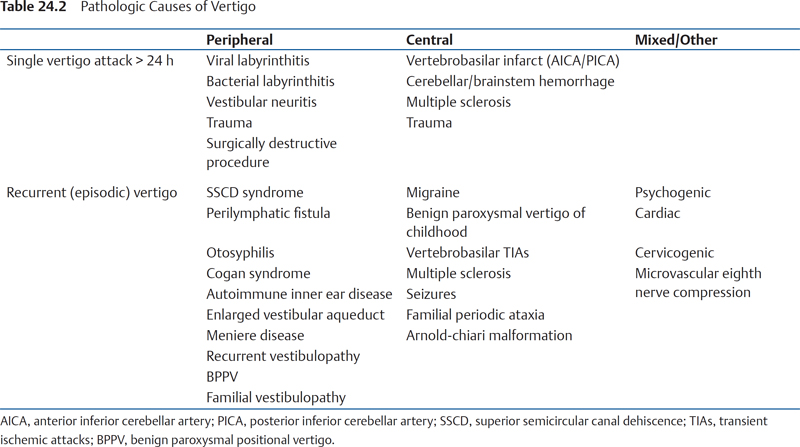
There are a host of peripheral, central, and other disorders that can cause vertigo (Table 24.2), with BPPV and Meniere disease being the two most common peripheral causes. Meniere disease will not be discussed in this chapter as it is discussed in Chapter 23 in this book. Although there is some controversy about whether clinicians should make the differentiation between peripheral and central, it is a useful exercise to help establish the differential diagnosis. This will help direct the workup, guide the treatment, and, if indicated, direct the patient to the proper specialist.
Peripheral disorders induce vertigo through their evoked, nonphysiologic asymmetric central input. Therefore, not surprisingly, the peripheral disorders listed in Table 24.2 are all typically unilateral. Ultimately, many of these disorders resolve with time, returning the system to a steady state; alternatively, if the vestibular end organ remains dysfunctional, the system (brain) adjusts to a new norm (vis-à-vis the new steady state). This process is mediated by the cerebellum and brainstem and occurs automatically in most individuals as long as the contralateral vestibular organ remains normal (the redundancy described earlier). This “compensation” process is enhanced greatly by head, visual, and body motion/stimulation and can be inhibited by vestibular suppressant medication and immobility. Thus, even though patients favor sedentary activity because it tends to minimize the vestibular “asymmetry” and eases their symptoms, anyone with an acute vestibular disorder should be encouraged to ambulate as much and as soon as possible and avoid taking vestibular suppressants such as the benzodiazepines. For many individuals, a formal course of vestibular rehabilitation physiotherapy greatly facilitates the process.
Table 24.1 Features of Peripheral versus Central Vertigo
| Peripheral | Central |
Vertigo onset | Usually sudden | Sudden or gradual |
Vertigo severity | Often intense and disabling | Less distinct and disabling |
Vertigo pattern | Single self-limited or episodic | Episodic or constant |
Vertigo aggravated by head movement | Yes | Not usually |
Associated nausea, vomiting, diaphoresis | Frequent and prominent | Infrequent and less severe |
Nystagmus type | Horizontal or torsional (or mixed); almost never vertical | Horizontal, torsional, or vertical |
Nystagmus direction | Typically unidirectional with fast phase usually away from the affected ear (irrespective of direction of gaze) | May be bidirectional; may change direction with changes in direction of gaze |
Nystagmus intensity affected by fixation | Intensity decreased or totally suppressed by visual fixation (except torsional variant) | Intensity unaffected or, rarely, enhanced by visual fixation |
Nystagmus intensity usually not affected by direction of gaze | Nystagmus intensity may be increased when patient looks in direction of fast phase | Nystagmus intensity affected by direction of gaze |
Hearing loss and facial weakness | May be present | Very uncommon |
Central nervous system symptoms/signs | Absent | Often present |
Gait | Mild to moderate ataxia with tendency to fall toward side of lesion | Moderate to severe ataxia with tendency to fall to either side |
As a result of impaired central compensation, virtually all these acute or episodic inner-ear disorders can become chronic. It is therefore important for the clinician to differentiate between cases of “true” episodic vertigo brought on by head movement such as occurs in BPPV, and the dysequilibrium arising from the asymmetry of an uncompensated loss that is merely aggravated by head motion.
Of all the “central” disorders in Table 24.2, migraine is by far the most common and most likely to be mistaken for and/or diagnosed along with peripheral vertigo. Vertigo is a common occurrence with migraine, though in itself it is usually less intense than peripheral vertigo. It can occur before, during, after or independent of the headache. There is also an increased incidence of BPPV and possibly Meniere disease with migraine.
In addition to an uncompensated unilateral vestibular loss, chronic (vestibular) dysequilibrium may result from bilateral vestibular hypofunction (Table 24.3). Bilateral disorders resulting in permanent vestibular hypofunction provide no backup, without any future possibilities for vestibular compensation. When both sides are affected simultaneously, as is often the case in systemic vestibulotoxicity from medications (most commonly aminoglycosides), there is no resultant vestibular asymmetry and thus no initial period of vertigo.
The hallmark features of bilateral vestibular hypofunction, all of which are derived from the absent vestibular input, are gait ataxia, oscillopsia (visual blurring with head movement), and the absence of symptoms with the head at rest. The hallmark vestibulo-ocular test findings include diminished or absent caloric responses and abnormal lateral head thrust tests bilaterally. Unfortunately, there are few treatments to offer these patients. Their long-term safety should be considered when they are advised about the operation of heavy machinery and automobiles. Assistive living devices such as canes, walkers and grab bars in the home are vital. Several centers are undertaking efforts to develop vestibular “prostheses.”
Single Episode Vertigo
Acute Vertigo with Hearing Loss
Viral Labyrinthitis
Nonbacterial labyrinthitis is thought to be caused by viral infections. Viruses implicated include herpes zoster, measles and mumps.1 However, definitive evidence for a viral etiology remains elusive at present, and as such a variety of pathophysiologic theories exist. These include a novel theory of labyrinthitis which proposes free-floating particles in the endolymph as the causative agent.2
Evaluation
Viral labyrinthitis is a clinical syndrome defined by the presence of acute-onset vertigo, disequilibrium, hearing loss, and vegetative symptoms.3 A viral prodrome may be described by the patient.
Physical Examination
Spontaneous horizontal nystagmus or a mixed horizontal/torsional nystagmus beating toward the healthy ear can be observed.1 Romberg testing demonstrates positional imbalance. The evaluation should include a complete head and neck examination, as well as a focused neurological examination. The Dix-Hallpike maneuvre should also be performed, which will be negative.
Videonystagmography
Caloric testing reveals a unilateral decreased response in the affected ear.
Audiometry
Audiometry is recommended to document the extent of hearing loss.
Diagnosis
Diagnosis of viral labyrinthitis is based on clinical history and physical examination, and is supported by videonystagmography (VNG) and audiometric testing. Exclusion of neurological causes for the clinical presentation must be completed, which may include appropriate imaging.
Management
The acute phase lasts days to a few weeks. Symptomatic recovery involves vestibular compensation. Supportive care, including hydration and antiemetics, may be used in the short term. Vestibular exercises should also be considered to hasten vestibular compensation.
Bacterial Labyrinthitis
Bacterial infection of the inner ear can occur from the subarachnoid space to the scala tympani via the cochlear aqueduct in meningitis, through the temporal bone modiolus in osteomyelitis, by hematogenous spread through the stria vascularis,4 or from the middle ear in otitis media.5 In one series, 13.7% of pediatric patients with meningitis also developed sensorineural hearing loss (bilateral in 74.6% and unilateral in 25.4% of the children who developed sensorineural hearing loss).6 These authors found five variables to be associated with the development of hearing loss in meningitis patients: CT evidence of increased intracranial pressure, male sex, glucose levels in the cerebrospinal fluid (CSF), Streptococcus pneumoniae as the causative organism, and presence of nuchal rigidity. Haemophilus influenzae, Streptococcus pneumoniae, and Neisseria meningitidis were found to be the top three causative organisms in patients with hearing loss.
Table 24.3 Vestibular Causes of Chronic Disequilibrium
Uncompensated unilateral loss Vestibulotoxicity (aminoglycosides) Congenital/hereditary Bilateral Meniere disease Autoimmune disorders Meningitic labyrinthitis Trauma Presbyastasis (aging) Chronic radiation effects Bilateral acoustic neuromas (neurofibromatosis type 2) Idiopathic |
Evaluation
The patient is questioned for symptoms of bacterial meningitis, such as headache, fever, stiff neck, and photophobia. A thorough neuro-otologic history includes questions regarding hearing loss, vertigo, imbalance, tinnitus, otalgia, otorrhea, and premorbid hearing status. Sudden onset of hearing loss and vertigo is expected in bacterial labyrinthitis. Nausea and vomiting may also be present.
Physical Examination
Meningeal signs, including nuchal rigidity, are evaluated. Meningitis of middle ear origin will present with findings of middle ear infection, including tympanic membrane inflammation and purulent middle ear fluid. Examination includes a complete head and neck examination, tuning fork testing, and a complete cranial nerve and neurological examination.
Laboratory Investigations
A complete blood count is drawn, which demonstrates an elevated white blood cell (WBC) count in patients with bacterial meningitis. Furthermore, in meningitis, a CSF sample is taken for WBC count (elevated, greater than 60% polymorphonuclear leukocytes), culture of causative organism, and Gram stain.4
Videonystagmography
Meningitis is a known cause of vestibulopathy.7 Vestibular testing should be considered in conjunction with the patient’s age and overall clinical condition. In some patients who eventually demonstrate improved audiometric results, their vestibular responses continue to be absent.8
Audiometry
Audiometric testing should be performed as soon as possible. For children under 6 months, distortion product oto-acoustic emissions (DPOAE) should be used. Those children that fail the DPOAE should undergo auditory brainstem response evaluation.6 Audiometric testing should occur at appropriate intervals following resolution of meningitis.
Diagnosis
Meningitic origin bacterial labyrinthitis will usually affect both ears, whereas an infection originating from the ear will result in unilateral bacterial labyrinthitis. Diagnosis of meningitis is based on clinical findings, elevated WBC, and elevated CSF WBC, and culture of a causative organism. Bacterial labyrinthitis diagnosis is clinical, based on the previously described findings.
Management
Auditory and presumably vestibular damage occurs early, and as such early diagnosis and antibiotic treatment are paramount.6 Patients with diagnosed meningitis and/or bacterial labyrinthitis are treated with intravenous (IV) antibiotics. CSF cultures help target antibiotic therapy in meningitis. Surgical management (drainage of middle ear fluid/mastoid infection) is based on the particular otological findings on examination. A myringotomy and culture can also guide antibiotic treatment. Adjunctive dexamethasone has been shown to reduce hearing loss in H. influenzae type b and pneumococcal meningitis.9
Mobilization and vestibular therapy are helpful in promoting vestibular compensation once the acute phase of disease is complete.
Early cochlear implantation has been recommended in patients with bilateral profound deafness caused by meningitis.10 The goal is to implant before the occurrence of labyrinthitis ossificans.
Acute Vertigo without Hearing Loss
Vestibular Neuritis (Vestibular Neuronitis)
Vestibular neuritis is an acute, isolated, and spontaneous unilateral vestibular de-afferentation syndrome.11 The incidence is 3.5 per 100,000.12
The current presumed etiology is a viral or postviral inflammation of the vestibular nerve,13 with histopathological studies revealing similar findings to those found in herpes zoster oticus.14 The finding of herpes simplex virus type 1 latency-associated transcripts in the vestibular ganglion by reverse transcriptase polymerase chain reaction supports a viral reactivation hypothesis of vestibular neuritis.15 The superior vestibular nerve is more commonly affected than the inferior. Superior nerve involvement may lead to degeneration of the uticular macula and its otolithic membrane with release of otoconia into the surrounding endolymph. Migration of these free floating otoconia into a semicircular canal (most commonly the posterior canal which is inervated by the inferior vestibular nerve) can then give rise to secondary BPPV.
Evaluation
Symptoms include an acute or subacute onset of continuous rotatory vertigo, gait and postural imbalance, nausea, and vomiting.16 The vertigo lasts for days with gradual improvement. Hearing is reported as subjectively normal. A complete focused history includes a search for other causes of vertigo and other neurological symptoms.
Physical Examination
Spontaneous nystagmus is observed that is typically horizontal with a torsional component, and does not change direction with direction of gaze. The head-thrust test17 is often positive in the direction of the affected side. Patients can stand, and on gait testing will veer toward the affected side.13 The evaluation should include a complete head and neck examination, as well as a focused neurological examination. The Dix-Hallpike maneuvre should also be performed, which will be negative.
Electro/Videonystagmography
Caloric testing typically, though not always, reveals unilateral vestibular hypofunction on the affected side.13
Audiometry/Imaging
Audiometry and imaging (computed tomography [CT]/magnetic resonance imaging [MRI]) of the head reveal normal thresholds and anatomy, respectively.13
Diagnosis
The diagnosis is made on a history of spontaneous prolonged (lasting days) vertigo, a physical examination consistent with a unilateral peripheral vestibulopathy (unilateral positive head-thrust), and the absence of signs and symptoms suggestive of another neurological process.13
Management
During the acute phase, patients are treated with short-term vestibular suppression to control their vestibular symptoms. Examples include dimenhydrinate and lorazepam13 though caution should be taken with the latter as benzodiazapenes, though effective in suppressing the vestibular asymmetry centrally at the brainstem level, may prolong the recovery.
Given the presumed viral/inflammatory etiology of vestibular neuritis, it is reasonable to direct therapy at decreasing the inflammation. This therapy typically involves oral corticosteroids. In a small, double-blind, prospective, placebo-controlled, crossover study, methylprednisolone was found to be more effective than placebo in controlling vertiginous symptoms.18 However, a recent meta-analysis concluded that corticosteroids were only beneficial in caloric response recovery and did not improve clinical symptoms.16 The role of corticosteroids in vestibular neuritis remains controversial.
Antiviral treatment with either acyclovir or valacyclovir should also be considered, although evidence supporting its use is limited. A recent placebo controlled randomized clinical trial in patients with vestibular neuritis demonstrated that methylprednisolone significantly improves the recovery of peripheral vestibular function, but that valacyclovir does not show a benefit in this patient population.19
Vestibular exercises have long been considered helpful to promote compensation after a vestibular lesion. The earlier the exercises are started, the quicker and better are the rehabilitation results.20 In a controlled human study, vestibular exercises were shown to improve central vestibulospinal compensation after vestibular neuritis compared with patients not treated with vestibular exercises.21
Recurrent Vertigo
Recurrent Attacks of Vertigo with Hearing Loss
Superior Semicircular Canal Dehiscence Syndrome
The superior semicircular canal dehiscence (SSCD) syndrome was first described by Minor et al.22 Studies on cadaveric temporal bones have found a dehiscence of the overlying bone of the superior semicircular canal in 0.5% of specimens.23 In an additional 1.4% of specimens, the bone coverage was less than 0.1 mm, such that it might appear dehiscent even on ultra-high resolution CT of the temporal bone.
The underlying pathophysiology is an opening in the bone that overlies the superior semicircular canal. This creates a third mobile window (the first and second being the oval and round windows) into the inner ear. As a result, the membranous labyrinth responds to sound and pressure changes. The resultant eye movements typically align themselves with the plane of the affected superior semicircular canal. Dehiscence of the bone overlying the superior semicircular canal is presumed to arise from a developmental cause.23,24 Precipitating events of the SSCD syndrome include direct trauma, and activities that produced changes in middle ear or intracranial pressure.25
Evaluation
This syndrome includes symptoms of vertigo or oscillopsia that is induced by loud sounds or pressure transmitted to the inner ear from the external auditory canal. This can result from application of pressure to the external auditory canal by pressing the tragus or inserting ear plugs, or during air travel. Vertigo or oscillopsia can be evoked by nose blowing or a Valsalva maneuver which increases middle ear pressure, or by coughing and straining (lifting, bowel movement) which increases the intracranial pressure. The Tullio phenomenon (sound-induced vertigo and/or nystagmus) often is characteristic of this syndrome. Patients may describe motion of objects in response to loud noise, with the direction of the perceived motion in a vertical-torsional plane.25 Associated auditory symptoms include hearing loss, autophony, and hyperacusis of bone-conducted sounds such as the sound of their own footsteps and even their eyes moving in the orbits.26 Other described symptoms include chronic disequilibrium, and motion intolerance.22 A complete focused history includes a search for other causes of vertigo.
Physical Examination
Sound- or pressure-evoked eye movements is best identified with Frenzel glasses.25 Positive pressure applied to the external canal by pressing on the tragus or by pneumatic otoscopy results in nystagmus with upward and torsional (motion of the superior pole of the eye away from the affected ear) components. On the contrary, negative pressure in the external canal or a Valsalva maneuver against a closed glottis results in nystagmus with downward and torsional (motion of the superior pole of the eye toward the affected ear) components. Weber tuning fork testing will lateralize to the affected ear, and a low frequency tuning fork (128 and 256 Hz) placed on the lateral malleolus of the ankle may be heard by the patient.27
The evaluation should include a complete head and neck examination, as well as a focused neurological examination (cranial nerves, gait, tandem gait, cerebellar testing, Romberg). The Dix-Hallpike maneuvre should also be performed.
Audiometry
Audiometry typically reveals a low-frequency conductive hearing loss on the affected side, with normal word recognition and intact acoustic reflexes.25,28 The intact acoustic reflexes may be the significant clue that differentiates SSCD from otosclerotic conductive hearing loss.29
Electro/Videonystagmography
Routine electronystagmography fails to identify objective abnormal findings, but the patient may report vertigo with the application of pressure to the external auditory canal.30
Vestibular-Evoked Myogenic Potentials
Vestibular-evoked myogenic potentials (VEMPs) are enhanced in SSCD, displaying a reduced response threshold on the affected side.26
Computed Tomography
High-resolution CT scanning is necessary to visualize the dehiscence. The use of thin 0.5-to 0.625-mm cuts and oblique reformats in the plane of the superior semicircular canal increases the positive predictive value to 93%.31 An example of CT findings in a patient with SSCD syndrome is shown in Fig. 24.1.
Diagnosis
SSCD syndrome is diagnosed by focused history, upward and torsional nystagmus elicited by sound/pressure, and radiological confirmation of bony dehiscence over the superior semicircular canal.25 Audiometry, acoustic reflexes and VEMP testing aid in the diagnosis.
Management
Conservative
In most patients, control of symptoms is achieved by avoidance of symptom-evoking sound and pressure stimuli.32 Only in the presence of debilitating vestibular or auditory symptoms should surgical management be pursued.
Surgical
Surgical management of SSCD syndrome is through resurfacing32 or plugging of the superior semicircular canal. Plugging is performed through a middle fossa22 or transmastoid29 approach.
The preferred approach at our center is the transmastoid approach, which has the advantages of obviating a craniotomy, avoidance of temporal lobe retraction, familiarity of the approach for experienced otologists, and the ability to occlude the canal without manipulating the defect.29 Briefly, a 5 to 6cm postauricular incision is made, a standard mastoidectomy is performed, and the horizontal canal is visualized. Bone between the horizontal canal and tegmen is carefully drilled layer by layer with a small diamond burr to blue-line the superior canal on both sides of the dehiscence. The dura over the canal is gently mobilized, but not elevated, to verify the dehiscence. Care must be taken, as dural elevation may cause injury to the inner ear. A 1 × 3 mm2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


