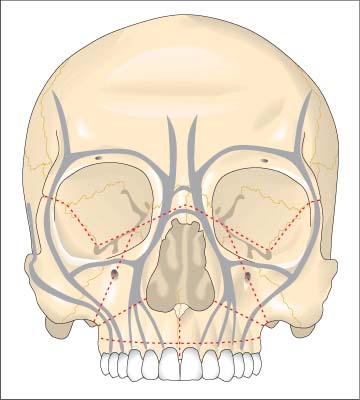
9 Diagnosing Injuries of the Midface The midface region includes the visceral cranium without the mandible, extending from the maxillary teeth to the superior margin of the orbits and root of the nose, where it shares a sizable border with the anterior and middle cranial base. The midface comprises: The midface is made of a system of cavities. Strong skeletal buttresses (nasal, maxillojugular, pterygopalatinal) absorb the forces of mastication and transmit them to the calotte. Spaces in between are bordered by delicate lamellar bone (Fig. 9.1). Anatomic and functional weaknesses (e. g., the infraorbital nerve canal or frontozygomatic suture) act as predetermined breaking points, allowing classification of midfacial fractures. With the exception of the masseter muscle and the medial and lateral pterygoid muscles, the bony structures of the midface lack strong muscles. Gross displacement occurs chiefly as a result of the traumatic blow and less as a result of muscular pulling forces. An exception is the anterior open bite deformity, which is caused by pull of the medial pterygoid muscle in midfacial fractures, drawing the maxilla to dorsal and caudal. The cavity system of the midface consists of the orbital cavities, maxillary sinuses, nasal cavity, ethmoid cells, and sphenoid sinus. While the integrity of the eye sockets ensures unimpaired and proper functioning of the ocular muscles, vital for depth perception, the skeletal structure of the nose and paranasal sinuses ensures physiologic nasal breathing. Lining the nose and paranasal sinuses is a layer of mucosa, which contains ciliated epithelium and allows continuous clearance of discharge out of the paranasal sinuses into the nasal cavity. Ventilatory disturbances cause destruction of the ciliated epithelium; adhesions, unphysiologic skeletal buttresses, and obstructed ostia hinder clearance of discharge. Thus, midfacial fractures which heal in malposition not only affect cosmetic appearance and impair masticatory function, but they also impair ventilatory function of the nose and paranasal sinuses and can thus lead to chronic sinusitis. In addition, malposition in the orbital region can eliminate depth perception. Fig. 9.1 Framework of the midfacial skeleton (from Schwenzer and Ehrenfeld, Vol. 2, 2002). The buttresses are shown in gray and typical fracture lines in red. Classifications of midface fractures vary. The classification presented here is based on a combination of localization and fracture type (Table 9.1). Localization is the main factor in categorization of midface fractures. On the basis of the traditional classification systems of Gu rin, Le Fort, Wassmund, Thoma, Spiessl, and Scholl, one can separate fractures into: These two forms can occur to varying degrees in combination. The Le Fort classification is the most widely used, despite the fact that it fails to describe a number of fractures sufficiently (e. g., fractures of the nasoethmoidal complex). Especially in focused high-energy trauma, fractures can occur at atypical localizations or as comminuted fractures of the midface.
 Flowchart and Checklist Craniofacial Injuries, Chapter 3, p. 20.
Flowchart and Checklist Craniofacial Injuries, Chapter 3, p. 20.
 Treatment of Injuries of the Midface, Chapter 19, p. 157.
Treatment of Injuries of the Midface, Chapter 19, p. 157.
Surgical Anatomy
 maxilla;
maxilla;
 nose;
nose;
 ethmoid bones;
ethmoid bones;
 sphenoid bones;
sphenoid bones;
 zygomatic bones;
zygomatic bones;
 lacrimal bones;
lacrimal bones;
 vomer.
vomer.
Classification of Midface Fractures
 fractures of the lateral midface (zygomatic fractures) and;
fractures of the lateral midface (zygomatic fractures) and;
 fractures of the central midface.
fractures of the central midface.
Localization | Fracture form |
Central midface | Infrazygomatic fractures (alveolar process fractures, dentoalveolar complex) |
Le Fort I or Guérin fracture with-and-without sagittal fracture | |
Central or pyramidal fractures (Le Fort II fracture with-and-without sagittal fracture) | |
Nasal skeleton fracture (nasomaxillary and nasoethmoid complex) | |
Irregular fractures | |
Partial fractures and defect fractures | |
Lateral midface Lateral fractures: | – zygomaticoorbital complex |
– isolated zygomatic bone fractures | |
– zygomaticomaxillary fractures | |
– isolated zygomatic arch fractures | |
– complex zygomatic bone/zygomatic arch fractures | |
– orbital margin fractures | |
– orbital wall fractures (“blow-out” fracture) | |
– zygomaticomandibular fractures | |
Combined central and lateral midface | Centrolateral fractures: detachment of the entire midface from the skull base, Le Fort III fracture |
Anterior and lateral skull base | Detachment of midface and anterior skull base (anterior skull base fracture), fracture of the temporal bone and petrous pyramid (fracture of the lateral skull base) |
Central Fractures of the Midface
Le Fort I and II are central midface fractures. The central segment of the midface is detached from the surrounding facial skeleton and displaced to dorsal or also wedged in.
Displacement is chiefly determined by the direction of trauma, but also by muscular traction of the pterygoid muscles. Both pairs of pterygoid muscles work to pull the mobile midface to dorsal and caudal (open bite). If fracture occurs in combination with sagittal fracture of the maxilla, a gap (diastema) forms between the affected incisors; severe displacement can cause a traumatic cleft palate (Fig. 9.2).
Fractures of the Alveolar Process
Fractures of the alveolar process involve isolated avulsion of the alveolar process. Osseous continuity can remain intact in the mandible, while involvement of the front incisor region of the maxilla affects the nasal floor, and lateral incisor region involvement affects the maxillary sinus. Alveolar process fractures often occur with concomitant dental injury.
Pathomechanism
Fractures of the alveolar process are caused by blunt trauma directed toward the front or side of the alveolar process. Displacement normally occurs in the direction of force, usually to dorsal or lateral. The more focused the impacting energy, the greater the likelihood of dental injury.
 Treatment of Alveolar Process Fractures, Chapter 22, p. 203.
Treatment of Alveolar Process Fractures, Chapter 22, p. 203.
Le Fort I Fractures
The fracture line travels from the pyriform aperture above the nasal spine through the anterior wall of the maxillary sinus, the zygomaticomaxillary buttress, the maxillary tuberosity, through the caudal tip of the pterygoid plates, the nasal wall of the maxillary sinus, finally reaching its starting point at the pyriform aperture.
There is often involvement of vomer and dislocation of the cartilaginous nasal septum. Septal hematomas can also occur. In some cases, the pterygoid process does not break, resulting instead in avulsion of the maxilla where the two structures meet.
Pathomechanism
Le Fort I fractures are caused by trauma from a blunt object over a large surface area, striking the dentoalveolar portion of the jaw from the front or side (Fig. 9.3).
Displacement generally occurs in the direction of trauma, usually to dorsal or lateral. Occasionally, the maxilla may rotate around a vertical axis.
Displacement due to the pulling forces of facial muscles is less common and only observed in atypical fractures in which the pterygoid process is separated from the cranial base and the maxilla is displaced to dorsocaudal by the pulling force of the medial pterygoid muscle.
Clinical Symptoms
Swelling of the upper lip and cheek is often seen and can extend to the region around the eyelid. Hematomas are common.
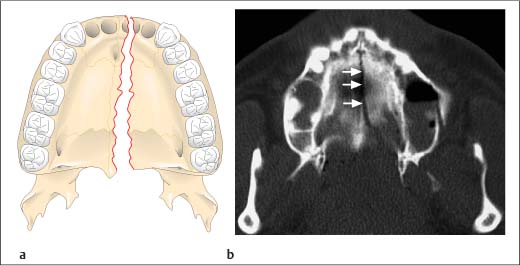
Fig. 9.2 Sagittal fracture of the maxilla.
a Schematic illustration (from Schwenzer and Ehrenfeld, Vol. 2, 2002).
b Axial view on computed tomography. Arrows indicate fracture line.
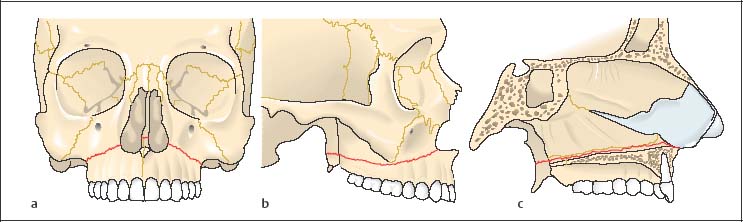
Fig. 9.3 Fracture lines in a Le Fort I fracture (from Schwenzer and Ehrenfeld, Vol. 2, 2002).
“Raccoon eye” or “monocle” hematomas are less common and generally affect mainly the lower lids. The swollen area is especially tender to palpation at the canine fossa. Sensory disturbances in the distribution area of the infraorbital nerve are only observed with abnormally high fracture lines. The oral vestibule may appear swollen and there are frequently submucosal hematomas in the cheeks and lips.
Displacement of the maxilla commonly results in malocclusion. Palpation reveals step-offs on the zygomaticomaxillary buttress and pyriform aperture as well as abnormal mobility of the maxilla.
There are tears in the mucosa of the oral vestibule and in the mucosal lining of the nose with hemorrhage from the mouth and nose. Posterior displacement of the maxilla results in a clinical picture resembling pseudoprognathism and there is hypophonesis (bandbox resonance) if the maxillary teeth are tapped with an instrument.
In sagittal fractures, the palatine mucosa also tears, resulting in diastema in the anterior maxilla, usually between teeth 11 and 21.
Certain signs of fracture include:
– abnormal mobility;
– displacement and resulting malocclusion;
– crepitus detection.
Diagnostic Imaging
In patients with multiple trauma, computed tomography of the midface (coronal or axial) is the method of choice. This allows imaging in a single series of all important structures, including adjacent regions and the skull base, without superimposition or changing the patient’s position (Fig. 9.4).
Computed tomography currently allows the most precise diagnosis of Le Fort I fractures and thus has—by and large—replaced conventional radiography techniques. Nonetheless, conventional radiography techniques are still justified in circumscribed alveolar process fractures or Le Fort I fractures.
 Paranasal sinus view (occipitomental projection): Shadowing of the maxillary sinus, often with fluid levels from hemorrhage into the sinus, is often visible as are fracture lines disrupting the pyriform aperture, anterior maxillary sinus wall, and zygomaticomaxillary buttress.
Paranasal sinus view (occipitomental projection): Shadowing of the maxillary sinus, often with fluid levels from hemorrhage into the sinus, is often visible as are fracture lines disrupting the pyriform aperture, anterior maxillary sinus wall, and zygomaticomaxillary buttress.
 Orthopantomogram: The maxillary sinuses show shadowing. There are fracture lines disrupting the pyriform aperture, the anterior maxillary sinus wall, and the maxillary tuberosity. Fractures of the dental roots can often be identified.
Orthopantomogram: The maxillary sinuses show shadowing. There are fracture lines disrupting the pyriform aperture, the anterior maxillary sinus wall, and the maxillary tuberosity. Fractures of the dental roots can often be identified.

Fig. 9.4 Fracture line in a Le Fort I fracture in the zygomaticomaxillary buttress region and lateral nasal wall (arrows, coronal computed tomography).
 Cephalogram (lateral cranium): This view allows visualization of posterior displacement of the maxilla or mid-face toward the skull base.
Cephalogram (lateral cranium): This view allows visualization of posterior displacement of the maxilla or mid-face toward the skull base. Dental films: These are used for exact evaluation of dental injuries.
Dental films: These are used for exact evaluation of dental injuries.
 Occlusal view: Occlusion projection of the maxilla is useful for detecting or excluding sagittal fracture.
Occlusal view: Occlusion projection of the maxilla is useful for detecting or excluding sagittal fracture.
Treatment
Treatment reduces fracture fragments and restores dental occlusion. Intermaxillary fixation and osteosynthetic measures using miniplates and microplates can be used.
 Treatment of Infrazygomatic Fractures (Le Fort I), Chapter 19, p. 170.
Treatment of Infrazygomatic Fractures (Le Fort I), Chapter 19, p. 170.
Le Fort II Fractures, Wassmund I Fractures
These fracture types describe detachment of a pyramid-like fragment from the midface; the maxilla, nasal skeleton, ethmoids, lacrimal bone, and sphenoid bone are involved. Associated injury of the skull base is common (Fig. 9.5).
The fracture line runs above or through the nasal bones, the medial orbital wall, along the inferior orbital fissure, traversing the infraorbital canal, infraorbital foramen, anterior maxillary sinus wall, and usually interrupting the middle third of the pterygoid process. Variations on fracture course are common.
Comminuted fractures of the bony nasal skeleton, septum dislocation, as well as fractures of the bony nasal septum, the vomer, and the perpendicular plate of ethmoid also occur.
The Wassmund I fracture does not include the nasal skeleton in the fracture fragment. The fracture runs from the orbital floor over the frontal process of the maxilla to the cranial margin of the pyriform aperture.
Pathomechanism
Fracture is predominantly caused by blunt trauma. The pterygoid process is avulsed from the cranial base, and the midface is displaced by the pull of the medial pterygoid muscles to dorsal and caudal (Fig. 9.6b).
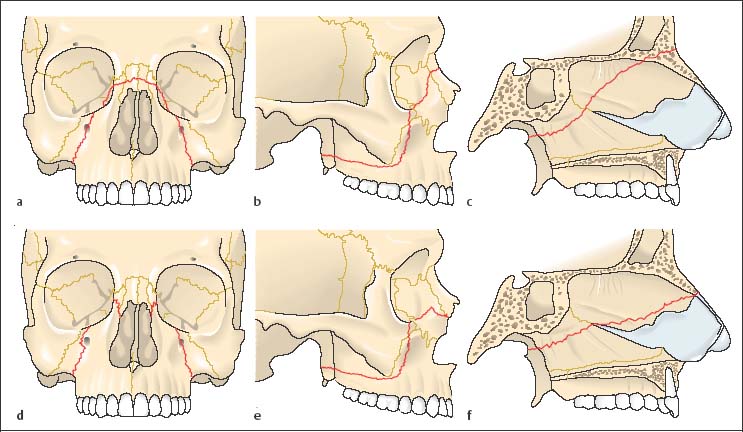
Fig. 9.5 Fractures in the Le Fort II level (from Schwenzer and Ehrenfeld, Vol. 2, 2002).
a–c Fracture lines in a Le Fort II fracture (Wassmund II fracture). The fracture is disrupting the nasal root.
d–f Wassmund I fracture. The fracture line mostly corresponds to the Le Fort II fracture line. The nasal skeleton is not involved.
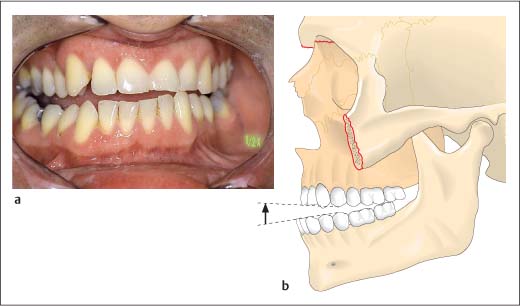
Fig. 9.6 Displacement of the midfacial fragment in a Le Fort II fracture.
a Malocclusion in the form of a maxillary retrognathism with open bite in a midfacial fracture.
b Dorsocaudal dislocation of the maxilla from pulling forces of the medial pterygoid muscle (from Schwenzer and Ehrenfeld, Vol. 2, 2002).
Clinical Symptoms
There is often unilateral or bilateral (raccoon eyes) periorbital hematoma, as well as swelling of the lids, cheeks, nose, oral vestibule, and often also orbital contents.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


