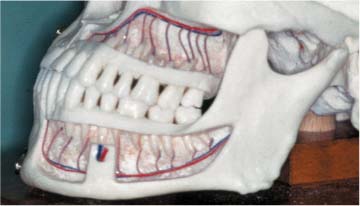
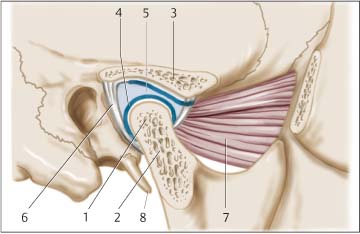
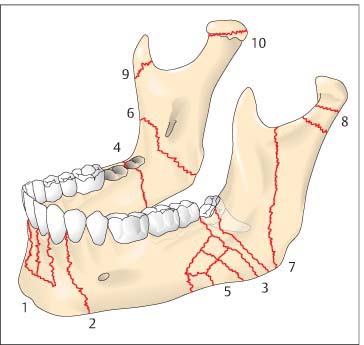
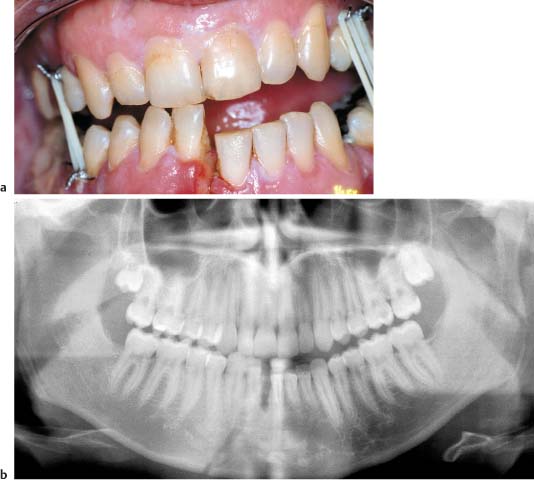
11 Diagnosing Injuries of the Mandible Checklist Treatment of Dental Injuries, Chapter 3, p. 24. Treatment of Dental Injuries, Chapter 22, p. 199. The lower jaw (mandible) is the only free-moving skull bone. The right and left portions of the mandibular arch are joined at the symphysis in the first year of life, forming a unique horseshoe-shaped skeletal component, whose attachment to the cranium is formed only by muscles and ligaments. A distinction is made between the mandibular body and the ramus of mandible. The ramus ends to cranial in the coronoid and condylar processes, which are separated by the mandibular notch (Fig. 11.1). The entire structure of the mandible is comprised of a solid skeletal construction (basilar arch), extending from the coronoid and condylar processes, over the rami and body, to the chin—allowing insertion of masticatory and tongue muscles—and a periodontal component (alveolar process). Innervation: The mandibular nerve enters the bone about 1 cm caudal of the mandibular notch at the mandibular foramen. It enters from lingual and continues through the mandible in a bony canal (mandibular canal) as the inferior alveolar nerve, together with arteries and veins, branching off into nerve fibers providing sensation to molars, premolars, and the gingiva. Fig. 11.1 Mandible with periodontium, nerve exit orifices, and course of the inferior alveolar nerve. The inferior alveolar nerve exits the mandibular body between the root tips of the first and second premolars as the mental nerve, providing sensation to the lower lip. Before leaving the mandibular body, it branches off into other nerve branches for the canines and frontal incisors. The distance between nerve canal and root tips or buccal cortical bone varies, but is on average around 5 mm. The lingual nerve runs near the inferior wisdom tooth, close to the mandible and sometimes separated from it only by the periosteum. The temporomandibular joint is the mobile connection between the mandibular condyle and the mandibular fossa of the squamous portion of the temporal bone. The mandibular condyle has a cylindrical form and extends relatively far to medial. The articular fossa is much wider than the condyle, allowing considerable vertical, transversal, and sagittal motion of the mandible (Fig. 11.2). Fig. 11.2 Section showing the temporomandibular joint and anatomic structures (modified from Richter 1992). 1 Mandibular condyle, 2 cancellous bone in the mandibular condyle, 3 articular fossa (temporal bone), 4 articular cartilage of the mandibular condyle/articular fossa, 5 articular disc, 6 joint capsule with lateral ligament, 7 lateral pterygoid muscle, 8 styloid process. The joint capsule is relatively loose. Its attachment to the temporal bone surrounds the articular tubercle and extends posteriorly to the petrotympanic fissure. The joint capsule is attached to the articular disk. The mandibular portion of the capsule extends far beyond the condyle down to the condylar neck. The articular ligaments are not very pronounced. Nonetheless, the following ligaments can be distinguished: Between the articular fossa and condyle lies the biconcave fibrocartilage articular disk. The articular disk is attached around its entire periphery to the joint capsule, dividing the temporomandibular joint into a superior and inferior space, and forming the functional articular fossa. The gliding motion of the joint occurs in the superior chamber, between the articular disk and skull base, while rotational movement of the mandibular condyle is possible in the inferior chamber. The physiologic motion of the temporomandibular joint is a rotational-gliding motion, which is directed by the coordination of the muscles of mastication (stomatognathic system). Because each of the two temporomandibular joints is rigidly connected to the other via the mandible, any movement occurring on one side necessarily affects the joint on the other side. The mandible’s exposed position makes it vulnerable and a frequent site of traumatic injury. Mandibular fractures are among the most common skeletal injuries occurring in human beings. Causes predominantly include assault, traffic accidents, and falls. As in all head injuries, mandibular injury is frequently associated with cranial, craniocerebral, and especially cervical spine injury. Mandibular fractures occur as simple, double, or multiple factures, often together with midfacial fractures. They are caused by direct and indirect trauma: Mandibular fractures tend to occur at typical areas of weakness (condylar process, mandibular angle with unerupted third molars, canine tooth region with long dental roots, and cysts). Displacement of fragments is caused, on the one hand, by traumatic force and on the other by the pull of muscles. Remember the closing muscles of the jaw are much stronger than the opening muscles. Thus, the orientation of the fracture line can be considered either favorable or unfavorable for displacement. Diagnosis of mandibular fractures is often possible on the basis of clinical symptoms. A search should be made for specific and unspecific signs of fracture: – deformity of the fractured bone with displacement; – abnormal mobility of the fragments; – crepitus. – hematomas and swelling; – tenderness and compression pain around the fracture; – abnormal function and sensory disturbances. The upper and lower jaws meet in a special position because of the dental arches. Normally the maxillary and mandibular teeth of a closed jaw fit together perfectly (occlusion), and there are no step-offs in the dental row. As fracture often causes step-offs in the dental row, malocclusion and step-offs in the dental row are important signs of mandibular fracture. However, they are also observed in isolated dental luxation and fractures of the alveolar process. In fractures involving the extremities, deformity of the fractured bone is frequently visible as abnormal bending or angulation. In mandibular fractures, angulation is often obscured by soft tissue swelling. Even with minimal displacement of the fragments, angulation and step-offs in the dental row and alveolar process can be seen or palpated intraorally. These are generally associated with malocclusion. Because of the firm attachment between the mucosa of the alveolar process and the bone (attached gingiva), displacement can cause gingival laceration over the fracture site. Abnormal mobility of bony fragments is a certain sign of fracture and is regularly detected in alveolar process fractures, mandibular fractures in the dental row, and fractures in the mandibular angle region. However, abnormal mobility of mandibular fragments is often difficult to distinguish from abnormal mobility of luxated teeth. Detection of mandibular fractures of the ramus, including intraarticular fracture, is not possible based on abnormal mobility. Segmental mandibular fractures (symphyseal fracture with basal triangle) with unfavorable fracture lines can result in complete loss of mandibular continuity and stability. Similar signs are observable in avulsion of the tongue musculature from the chin (missile wounds and explosion injuries) (Fig. 11.3, see also Fig. 1.2). Crepitus describes a grating sound heard when broken bone ends rub together. Mandibular fracture surfaces are often smooth so that there is minimal crepitation. Fig. 11.3 Segmental mandibular fracture with considerable displacement. Swelling of the tongue and floor of the mouth can pose a risk of airway obstruction. Considerable bleeding in the floor of the mouth, cheeks, soft tissue of the chin, and, less frequently, the tongue and pharyngeal soft tissue results from fracture and traumatic tearing of the soft tissue. There is also concomitant posttraumatic edema. The skin in the affected region is taught and elastic; step-offs are hardly palpable through the swelling. Even palpation of the margin of the mandible is often impossible. Hematoma and edema in the floor of the mouth can take on life-threatening proportions, making immediate intubation, and occasionally tracheotomy (cricothyrotomy) necessary. This is especially the case with complete loss of mandibular stability (segmental chin fracture with displacement of the tongue to dorsal, see Fig. 1.2). Tenderness to palpation is found with nearly every fracture. However, it is also a sign of inflammation and occasionally tumor. Lacking tenderness to palpation tends to support a cause other than fracture. Mild pressure applied to the longitudinal axis of the mandible with a tap on the chin elicits pain at the fracture site. Looking for signs of longitudinal compression pain is especially useful for diagnosing fractures of the mandibular ramus, and the condylar process in particular. Compression pain is also present, however, with contusion, distortion, and inflammation of the temporomandibular joint. Mandibular fractures restrict chewing, speaking, and swallowing functions. Trismus, lockjaw, or lateral deviations on opening the mouth are signs of fracture, but are also observed in other disorders (dislocation, abscess, and tumor). Fractures of the mandible between the mandibular foramen and the mental foramen regularly traverse the alveolar canal. Lesions of the inferior alveolar nerve are caused by direct tear, crushing force, or hematoma. Hypesthesia, anesthesia, or occasionally paresthesia, occur distal to the injury in the nerve distribution area, predominantly affecting the lower lip. Sensation in the teeth and gingiva is impaired or lost. Sensory disturbances in the nerve distribution area of the mental nerve can be observed, however, after shearing injuries involving soft tissue in the chin area and following extensive hematoma—without the presence of fracture. Sensory disturbances involving lingual nerve distribution seldom occur as a direct result of trauma. The lingual nerve can be injured by bone fragments in mandibular angle fractures or by extensive hematoma in the floor of the mouth. Under physiologic conditions the teeth of the upper and lower jaw fit together in a specific position (normal occlusion), whereby there can also be individual interdigitation (individual occlusion). Wear facets are often observable on the corresponding surfaces of opposing teeth. Any deviation without plausible explanation from this specific and routinely reproducible occlusion must be considered—with an appropriate patient history—a sign of fracture. This is especially true for unilateral malocclusion. Conventional radiographic diagnosis has primacy in routine diagnosis of isolated mandibular fractures. All fractures of the mandible must be viewed in two planes. Panoramic views (orthopantomogram) and posterior-anterior (p.-a.) half-axial mandibular views (based on the Clementschitsch technique) are considered standard. Survey radiographs of the cranium are less useful in evaluating mandibular fractures, especially intraarticular fracture, as there is often superimposition of structures. Conventional radiography should always use the posterior-anterior (p.-a.) view for evaluating the facial skeleton, as only those structures close to the film are sharply imaged (film is closest to the face). Special projections are occasionally helpful for visualizing the temporomandibular joint (e. g., the technique based on Sch ller, and the technique based on Hofrath). Dental films and occlusal views are especially suitable for intraoral diagnostics (tooth in fracture gap). Like midfacial fractures, many mandibular fractures can now be more precisely imaged using computed tomography than with conventional techniques. This is especially true for multiply traumatized patients with craniocerebral and spinal injuries; initial diagnosis can thus include evaluation of not only the cranial bones, but also the facial skeleton and spine with high-quality images. Axial views are generally used for evaluating injury. Coronal reconstructions are possible using small slice thicknesses on axial CT. However, visualization of structures is less exact than on direct coronal views. For specific clinical questions, such as diagnosis and treatment planning in temporomandibular fractures, coronal views are superior. Evaluation requires a special, hyperextended position and can only be performed after spinal injury has been ruled out. Magnetic resonance imaging can offer high quality imaging of changes in position or injury of the articular disk as well as changes in the joint capsule. Early detection of inflammatory complications such as osteitis at the fracture gap or osteomyelitis is possible. Orbital soft tissue structures can be shown on high-quality images without adverse radiation effects. Fractures can be divided based on anatomic, functional, and treatment aspects into (Fig. 11.4): – without dislocation of the condylar process; – with dislocation of the condylar process; – fracture-dislocations; This classification is intended for the dentate adult with normal occlusion. It can be roughly applied to fractures involving primary teeth, dentures, and the edentulous mandible. Fig. 11.4 Typical localization of mandibular fractures (from Schwenzer and Ehrenfeld, Vol. 2, 2002). 1 Alveolar process, 2 within the dental row (transverse fracture), 3 outside of the dental row in a fully dentate jaw, 4 outside of the dental row in a partially edentulous jaw, 5 comminuted fracture, 6 in ramus of mandible (oblique fracture), 7 in ramus of mandible (longitudinal fracture), 8 condylar process, 9 coronoid process, 10 condylar head. Direct trauma (fall onto the chin) causes the mandible to bend open and fracture (bending fracture). These fractures are often slightly displaced, especially in children (greenstick fracture). Pull from the masseter muscle causes slight tilting of the dental rows to lingual, which in turn leads to dehiscence of the fracture gap (Fig. 11.5). Fractures in this region are predominantly direct fractures. The long root of the canine tooth is a weak point in the mandible and muscle pull often leads to displacement: Depending on fracture course and trauma, fragments can be displaced orally (Fig. 11.6). Bilateral fractures in the canine region involve symphyseal fracture with the basal triangle: Fig. 11.5 Mandibular fracture with dentoalveolar involvement. a Considerable displacement in a mandibular parasymphysis fracture with step-offs between teeth 41 and 42. b Step-off between teeth 41 and 42 (orthopantomogram). Fractures involving the lateral incisor region can be caused by direct or indirect trauma. Fracture often involves displacement with step-offs; and depending on direction of force displacement is longitudinal with contraction or distraction (Fig. 11.7a–e). In transverse fractures and fractures with a fracture line ascending to mesial (ventral), the small fragment is displaced upward (closing muscles) and to medial (temporal muscle, masseter muscle, lateral pterygoid muscle), and the large fragment downward (opening muscles) and to lateral (contralateral pterygoid muscle) (Fig. 11.8). Displacement is often absent with a fracture gap ascending to distal, as the fragments are wedged together and adapted by the closing muscles. Longitudinal fractures of the mandibular body (sagittal fractures) are uncommon. They occur when the mandible is struck by extreme force from inferior and the teeth of the lower jaw collide with those of the upper jaw. The roots of the teeth act as chisels, opening the mandibular body longitudinally. This often involves concomitant extensive dental fracture of molars and premolars in the upper and lower jaw. Management can be conservative using splinting of the mandible and maxilla and intermaxillary immobilization (rigid elastic bands or loop wiring) for 4–6 weeks. An alternative is osteosynthesis using miniplates or, if necessary, compression plates. Fig. 11.6 Mandibular fracture in the lateral incisor region. a Considerably dislocated mandibular fracture in the right canine region with complete occlusion. Dislocation of the fragments is mimicking a gap between teeth 43 and 42.b Marked displacement in a parasymphyseal fracture on the right (panorama view). c Displaced mandibular parasymphysis fracture on the right (arrow; axial computed tomography). Displaced fractures should be reduced. Conservative management following reduction employs splinting of upper and lower jaw and intermaxillary immobilization (rigid elastic bands or loop wiring) for 4–6 weeks. Osteosynthesis is usually the preferred method.
 Flowchart and Checklist Craniofacial Injuries, Chapter 3, p. 20.
Flowchart and Checklist Craniofacial Injuries, Chapter 3, p. 20.
 Treatment of Injuries of the Mandible, p. 186.
Treatment of Injuries of the Mandible, p. 186.
Surgical Anatomy
 temporomandibular ligament;
temporomandibular ligament;
 sphenomandibular ligament;
sphenomandibular ligament;
 stylomandibular ligament;
stylomandibular ligament;
 pterygomandibular ligament.
pterygomandibular ligament.
Pathomechanism
 Direct trauma is generally the cause of injury to the chin region and the area around the canine teeth and fractures involving the alveolar process and teeth; it is less often the mechanism of injury in the mandibular angle region.
Direct trauma is generally the cause of injury to the chin region and the area around the canine teeth and fractures involving the alveolar process and teeth; it is less often the mechanism of injury in the mandibular angle region.
 Injuries and fractures of the condylar neck and temporomandibular joint are almost without exception caused by indirect trauma.
Injuries and fractures of the condylar neck and temporomandibular joint are almost without exception caused by indirect trauma.
Clinical Signs and Symptoms
 Certain fracture signs:
Certain fracture signs:
 Uncertain fracture signs are often found in mandibular fractures, but they can also have other sources:
Uncertain fracture signs are often found in mandibular fractures, but they can also have other sources:
Certain Signs of Fracture
Deformity and Dislocation
Abnormal Mobility
 Segmental mandibular fractures involve acute risk of suffocation as the tongue has lost its anchoring and sinks to dorsal.
Segmental mandibular fractures involve acute risk of suffocation as the tongue has lost its anchoring and sinks to dorsal.
Crepitus
 Clinical examination is exceedingly painful and therefore should be avoided.
Clinical examination is exceedingly painful and therefore should be avoided.

Uncertain Fracture Signs
Hematoma and Swelling
Tenderness
Longitudinal Compression Pain
Restricted Function
Sensory Disturbances
Mental Nerve (Inferior Alveolar Nerve)
Lingual Nerve
Malocclusion
Diagnostic Imaging
Classification of Mandibular Fractures
 mandibular fractures within the dental row;
mandibular fractures within the dental row;
 mandibular fractures outside of the dental row;
mandibular fractures outside of the dental row;
 fractures of the angle of mandible;
fractures of the angle of mandible;
 fractures of the ramus of mandible (without condylar process involvement);
fractures of the ramus of mandible (without condylar process involvement);
 fractures of the condylar process;
fractures of the condylar process;
 fractures of the articular fossa.
fractures of the articular fossa.
Fractures of the Mandibular Body with Dentoalveolar Involvement
Pathomechanisms
Symphysis or Parasymphyis Fracture
Canine Region
 The smaller fragment is often pulled craniad by the closing muscles (temporal muscle) and tilted by the masseter muscle to lingual and displaced to buccal.
The smaller fragment is often pulled craniad by the closing muscles (temporal muscle) and tilted by the masseter muscle to lingual and displaced to buccal.
 The large fragment is pulled caudal by the tongue musculature and opening muscles of the mouth.
The large fragment is pulled caudal by the tongue musculature and opening muscles of the mouth.
 If displacement of the detached segment is to lingual, the tongue will fall to dorsal and there is risk of suffocation.
If displacement of the detached segment is to lingual, the tongue will fall to dorsal and there is risk of suffocation.
 The detached segment can be displaced peripherally, which is far less common. If injury involves avulsion of the attachment of the tongue, there is also risk of suffocation from the tongue falling to dorsal.
The detached segment can be displaced peripherally, which is far less common. If injury involves avulsion of the attachment of the tongue, there is also risk of suffocation from the tongue falling to dorsal.
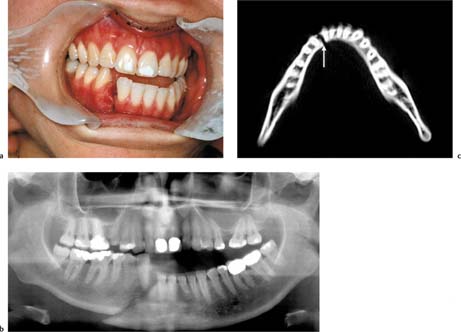
Lateral Incisor Region
Diagnostic Imaging
 panorama projection (orthopantomogram [OPG]);
panorama projection (orthopantomogram [OPG]);
 mandibular posterior-anterior, half-axial view (Clementschitsch)—film is closest to the face;
mandibular posterior-anterior, half-axial view (Clementschitsch)—film is closest to the face;
 half-lateral/lateral views of the mandible;
half-lateral/lateral views of the mandible;
 computed tomography;
computed tomography;
 dental films to determine the relationship between root and fracture gap and to detect or exclude dental root fracture.
dental films to determine the relationship between root and fracture gap and to detect or exclude dental root fracture.
Treatment
Nondisplaced Fractures
Displaced Fractures
Teeth in the Fracture Line
 The presence of a tooth in the fracture gap jeopardizes osseous healing considerably, particularly in the mandible. Saliva can enter the fracture gap through the periodontal pocket potentially causing osteitis in the fracture gap.
The presence of a tooth in the fracture gap jeopardizes osseous healing considerably, particularly in the mandible. Saliva can enter the fracture gap through the periodontal pocket potentially causing osteitis in the fracture gap.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


