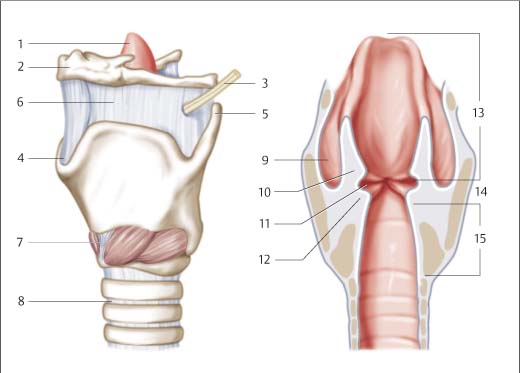
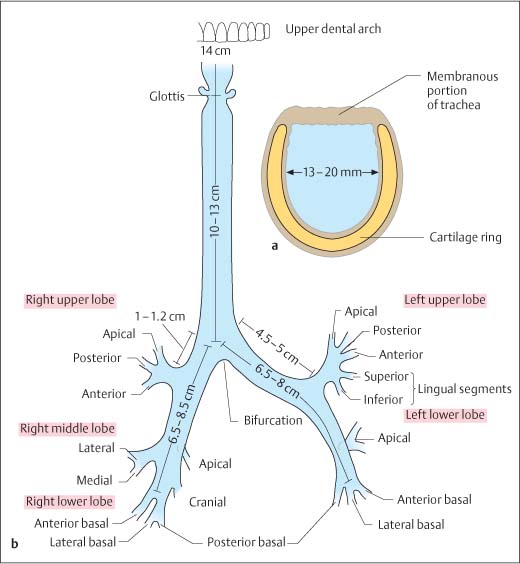
14 Diagnosing Injuries of the Larynx and Trachea Anteflexion of the head positions the mandible so that it affords effective protection against trauma to the larynx and cervical trachea. Injury to this region occurs if this protective reflex function is inhibited and the head is prevented from bending forward on impact. The rigid framework of the larynx is formed by four cartilages: The thyroid cartilage is made up of two laminae, which meet at approximately a right angle in men and at ca. 120 in women. The epiglottis petiole attaches to the inner side of the thyroid cartilage. The dorsal cricoid lamina extends into the interior of the thyroid cartilage frame, articulating with it and with the arytenoids. The vocal ligament and vocalis muscle are secured at the vocal process of the arytenoids. The laryngeal muscles are divided into those that open the glottis and those that close it. The only muscle that acts to open the glottis is the posterior cricoarytenoid (posticus) muscle. Spanning the ventral aspect of the cartilage framework, the cricothyroid muscle is the only laryngeal muscle innervated by the superior laryngeal nerve. All other muscles are supplied by the inferior (recurrent) laryngeal nerve, which originates from the vagus nerve and, after it loops in the thorax, travels cranially between the trachea and esophagus (Fig. 14.1). The trachea extends from the cricoid cartilage to its bifurcation, a distance of 10–13 cm, or in topographic terms of the vertebral column, from the sixth cervical vertebra to the fourth thoracic vertebra. The tracheal framework is made up of 15–18 horseshoe-shaped cartilage rings which are closed off dorsally by the membranous portion of the trachea (Fig. 14.2). Fig. 14.1 Anatomy of the outer and inner larynx (modified from Richter 1992). 1 epiglottis, 2 hyoid bone, 3 superior laryngeal nerve, 4 superior thyroid notch, 5 superior horn of thyroid cartilage, 6 thyrohyoid membrane, 7 cricothyroid muscle, 8 annular ligament, 9 pyriform sinus, 10 plica vestibularis (ventricularis, vestibular ligament), 11 laryngeal ventricle (sinus of Morgagni), 12 vocal fold (vocal ligament), 13 supraglottic space (this level is described as the transglottic space, which comprises the vestibular ligament, Morgagni’s ventricle, and vocal fold). Fig. 14.2 Anatomy of the trachea, bronchial tree, and segments (modified from Richter 1992). a Bronchial tree and segments—lengths. b Cross-section of the trachea. Injuries of the larynx (Figs. 14.3, 14.4) and trachea can be grouped according to pathomechanism as follows: – blunt extraluminal causes of trauma: impact, blow, strangulation, entrapment, sudden longitudinal pull from dorsal reflection of the head; – blunt intraluminal causes of trauma: long-term intubation, endoscopy, violent coughing, blunt foreign bodies; – sharp extraluminal causes of trauma: penetrating injury, cut, missile wound, rotating objects; – sharp intraluminal causes of trauma: sharp, aspirated foreign bodies; – sharp perforating trauma: missile wound, puncture, cut; – endolaryngeal mucosal lesions: caustic injury, scalding, thermal burn. Classification by degree of severity has proven itself clinically, as it also provides information useful for deriving necessary therapeutic measures (Table 14.1).
 Flowchart and Checklist Injuries of the Neck, Chapter 3, p. 25.
Flowchart and Checklist Injuries of the Neck, Chapter 3, p. 25.
 Treatment of Injuries of the Larynx, Pharynx, Trachea, Esophagus, and Soft Tissues of the Neck, Chapter 23, p. 209.
Treatment of Injuries of the Larynx, Pharynx, Trachea, Esophagus, and Soft Tissues of the Neck, Chapter 23, p. 209.
Surgical Anatomy
 thyroid cartilage;
thyroid cartilage;
 epiglottic cartilage;
epiglottic cartilage;
 arytenoid cartilage;
arytenoid cartilage;
 the cricoid cartilage.
the cricoid cartilage.
Pathomechanism and Classification
 Direct trauma:
Direct trauma:
 Indirect trauma.
Indirect trauma.
Grade | Description |
1 | Visible hematoma, hemorrhage, no fracture |
2 | Hematoma, swelling, nondisplaced stable fracture |
3 | Free cartilage, vocal cord dysfunction, unstable moveable fracture |
4 | Open laryngeal injury, laryngotracheal separation |
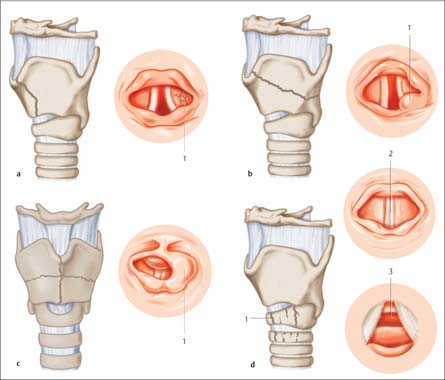
Fig. 14.3 Schematic illustration of injuries of the larynx (modified from Richter 1992).
a Linear vertical laryngeal fracture. A common form of fracture in noncalcified cartilage skeleton; associated with injuries of internal structures, which are destroyed as a result of elastic deformity of the inward and outward movement of the cartilage laminae. 1 Destruction of the soft tissues on one side.
b Linear oblique fracture of the larynx. The fracture line is above the level of the glottis (supraglottic fracture). The cranial thyroid cartilage fragment can be considerably displaced toward the hyoid, so that there is marked diastasis, which can be observed in the intrinsic structures as separation and mucosal tears in the Morgagni’s ventricle. The region around the arytenoids is edematous and hemorrhagic. Dislocation of the arytenoid cartilage is possible. 1 Edematous arytenoid.
c Multiple fracture or comminuted fracture of the larynx. This fracture form is most suited to calcified cartilage. The harder cartilage better protects the soft tissues of the transglottic space. However, the epiglottis is often separated at the petiole and covers the entrance to the larynx. Visualization of the interior of the larynx is then only possible with transnasal pharyngolaryngoscopy. 1 Supraglottic constriction.
d Cricoid fracture. proximity of the recurrent nerves causes palsy of the vocal cords with unilateral or bilateral medialization of the vocal folds. The mucosa of the subglottic space is injured and heals with formation of granulation tissue, which may develop into subglottic stenosis. 1 Cricoid fracture and fracture of the first tracheal ring; 2 view of the vocal fold level with complete vocal fold closure (medialization): severe respiratory distress, voice good; 3 subglottic granulation.
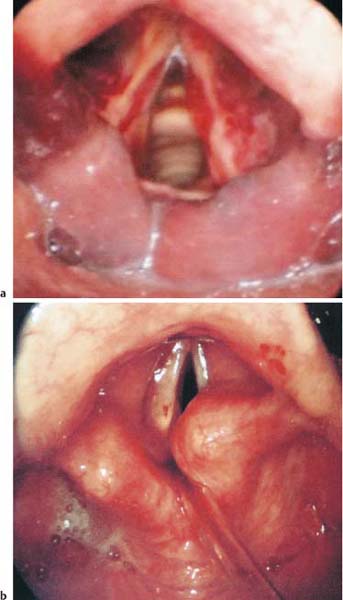
Fig. 14.4 Laryngeal injuries.
a Hematoma in the vocal folds and edema over both arytenoid cartilages following laryngeal trauma.
b Disarticulated right arytenoid cartilage after laryngeal trauma.
Fractures
The dynamics of laryngeal fractures vary. Fracture dynamics are determined by the direction and force of the blow, and by the maximum bending or fracture behavior of the cartilage. Compression testing has shown that the laryngeal lumen closes with a compression force of 15–20 kg from anterior.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


