12 Diagnosing Dental Injuries All teeth can be divided into three segments. The crown of the tooth protrudes into the oral cavity; the root secures the tooth to the alveolar bone; and the neck of the tooth forms the border region between root and crown. Hard dental tissue encloses the pulp chamber, which extends toward the roots into the root canal. Every tooth is made up of three varieties of hard dental tissue: Dental injuries are among the most common traumatic injuries involving the maxillofacial region. The exposed position of the maxillary central incisors, in particular, makes them vulnerable to injury in children between 8 and 12 years old. Children and adolescents with markedly protruding upper incisors are especially at risk. The remainder of dental injuries involves canines, premolars, and molars (Table 12.1). Dental injuries can be divided into fracture and luxation injuries, and both forms can occur concomitantly:
 Checklist Dental Injuries, Chapter 3, p. 24. Flowchart and Checklist Craniofacial Injuries, Chapter 3, p. 20.
Checklist Dental Injuries, Chapter 3, p. 24. Flowchart and Checklist Craniofacial Injuries, Chapter 3, p. 20.
 Treatment of Dental Injuries, Chapter 22, p. 199. Treatment of Injuries of the Mandible, Chapter 21, p. 186.
Treatment of Dental Injuries, Chapter 22, p. 199. Treatment of Injuries of the Mandible, Chapter 21, p. 186.
Surgical Anatomy
 Enamel is avascular and aneural and is comprised of 97 % inorganic material. Enamel is formed by internal enamel epithelium and is the hardest substance in the human body. Regeneration of enamel is impossible.
Enamel is avascular and aneural and is comprised of 97 % inorganic material. Enamel is formed by internal enamel epithelium and is the hardest substance in the human body. Regeneration of enamel is impossible.
 Dentin, unlike enamel, is produced over the lifespan. Dentin is formed by calcified ground substance secreted by odontoblasts, and is comprised of around 70 % inorganic material. Odontoblasts are mesodermal in origin, projecting long cytoplasmic extensions (Tomes’ processes) in the dentinal tubules, which run to the border between enamel and dentin.
Dentin, unlike enamel, is produced over the lifespan. Dentin is formed by calcified ground substance secreted by odontoblasts, and is comprised of around 70 % inorganic material. Odontoblasts are mesodermal in origin, projecting long cytoplasmic extensions (Tomes’ processes) in the dentinal tubules, which run to the border between enamel and dentin.
 Cement largely corresponds to woven bone, covering the dentin and entire root. The periodontal ligament collagen fibers (Sharpey’s fibers) are secured in the cement, suspending the tooth in the alveolar bone. Thus, mastication exerts pulling forces on the alveolar bone.
Cement largely corresponds to woven bone, covering the dentin and entire root. The periodontal ligament collagen fibers (Sharpey’s fibers) are secured in the cement, suspending the tooth in the alveolar bone. Thus, mastication exerts pulling forces on the alveolar bone.
Pathomechanism
 blunt, buffered trauma (blow to the lips) causes dental luxation;
blunt, buffered trauma (blow to the lips) causes dental luxation;
 direct trauma to the tooth causes dental fracture.
direct trauma to the tooth causes dental fracture.
Fractured teeth | Frequency (%) |
Central maxillary incisors | 70 |
Central mandibular incisors | 8 |
Lateral maxillary incisors | 6 |
Lateral mandibular incisors | 3 |
Dental Fractures
Classification
The classification of dental fractures is shown in Table 12.2 and Fig. 12.1.
Clinical Diagnosis
Attention should be paid to injuries of the lips when inspecting surrounding soft tissue injury as small fragments of fractured teeth can sometimes be found in the surrounding soft tissue. In injuries involving mandibular incisors (blow to the chin), injury of the temporomandibular joint should be excluded.
Extraalveolar dental fractures (crown fractures) | Enamel infraction |
| Enamel–dentin fracture without dental pulp exposure |
| Enamel–dentin fracture with dental pulp exposure |
Intraalveolar dental fractures | Coronal third root fracture |
| Middle third root fracture |
| Apical third root fracture |
| Longitudinal root fracture |
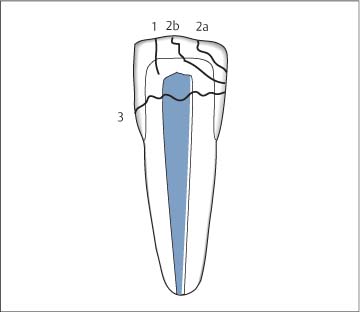
Fig. 12.1 Schematic illustration of types of dental fractures (from Schwenzer and Ehrenfeld, Vol. 2, 2002). 1 Crown infraction; 2 uncomplicated crown fracture, a enamel fracture, b enamel–dentin fracture without pulp exposure; 3 complicated crown fracture with pulp exposure.
Extraalveolar tooth fractures can be detected with inspection and palpation. Mobility of the injured tooth should be checked. In enamel-dentin fractures, attention should be paid to pulpal hemorrhage, which often appears as a mere pinpoint.
Testing of sensation (cold test) should be routinely performed. Findings may initially be negative, though pulp may be vital.
Diagnostic Imaging
Following injury of hard tissue, the patient should always undergo radiographic evaluation to rule out root or alveolar process fractures:
 panorama views (OPG);
panorama views (OPG);
 dental films;
dental films;
 occlusal views;
occlusal views;
 in exceptional circumstances (patient with multiple trauma) computed tomography.
in exceptional circumstances (patient with multiple trauma) computed tomography.
Treatment
For limited, isolated enamel infraction, sharp edges are smoothed and the enamel is treated with fluoride. If a larger area is involved, the clinical crown is restored using acid-etch bonding with composite filling.
In enamel-dentin fractures without pulp exposure (Fig. 12.2), the dentin wound is covered with a calcium hydroxide dressing for deeper wounds. Enamel injury is managed with acid-etch bonding with composite filling. Enamel-dentin fracture can be very painful, and because of risk of infection of the pulp via the open dentinal tubules, early management is desirable.
In enamel-dentin fractures with pulp exposure, it must be determined whether the pulp is viable (dot-like opening in children and adolescents) or whether pulpectomy is necessary. Pulpectomy must be followed by root canal obturation.
 Treatment of Dental Fractures, Chapter 22, p. 199.
Treatment of Dental Fractures, Chapter 22, p. 199.
Dental Luxation
Pathomechanism
Dental luxation involves traumatic loosening of the tooth with partial or complete tear of the Sharpey’s fibers. The alveolus is widened and there may be collapse or loss of the buccal alveolar wall. The tooth is thus partially or completely separated from the supporting periodontal structures, and vessels and nerves at the root tip are torn off; this is followed by pulp necrosis.
Classification
The following types of injury can be distinguished:
 dental concussion;
dental concussion;
 dental luxation without displacement (tooth loosening);
dental luxation without displacement (tooth loosening);
 dental luxation with displacement:
dental luxation with displacement:
– partial lateral luxation;
– complete lateral luxation;
– central luxation.
Clinical Diagnosis
Clinical evaluation assesses the degree of loosening, pain reaction to percussion, degree of displacement, disturbed sensation, and concomitant injuries (tooth, alveolar process, and jaw fracture as well as soft tissue injuries).
Diagnostic Imaging
Imaging procedures are similar to those used for tooth fractures. If there is an empty tooth socket with unexplained localization of the tooth, radiographic evaluation should exclude central luxation, lodging of the tooth or fragments in the surrounding soft tissues, and aspiration.
Treatment
Every dental luxation requires management.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


