Development of Binocular Vision
Robert H. Duckman
Jojo W. Du
Binocular vision refers to the condition where the two eyes view a common portion of visual space. In vertebrates, the size of this overlap ranges from 0° to about 190° in humans (1). In visual space, objects occupy a three-dimensional space; the x- and y-dimensions give the object visual direction, and the z-dimension gives the object depth information. The x- and y-axes information can be obtained from the geometric retinal image. The z-axes information, however, is not available to a single retina, but requires the input from two retinae. For humans, the eyes are frontally placed and laterally separated. This separation is crucial in providing the two eyes with slightly different views of an object. These small differences in retinal images, known as disparity, provide the critical z-axes information giving rise to depth perception.
Traditionally, Worth (2) classified binocular function into three hierarchically related levels:
Bifoveal fixation
Fusion
Stereopsis
In normal adults, the presence of bifoveal fixation is a necessary prerequisite for fusion, and fusion is essential for stereopsis. It is currently known, however, that bifoveal fixation is not a sufficient condition for functional fusion or for stereoscopic abilities. This chapter considers each of these three levels of binocular function to describe the mechanisms underlying the development of bifoveal fixation and fusion, leading to the pinnacle of binocular function, stereopsis, the ability to discriminate disparate information giving a three-dimensional depth percept.
Stereopsis is an acquired ability; thus, newborn babies do not perceive binocular depth until a sudden onset at age 3 to 5 months. This sudden onset is followed by a period of rapid maturation that finalizes between 4 and 6 months of age, in which the adultlike stereo- acuity is achieved. The oculomotor system is not mature at birth, but develops rapidly in parallel with the anatomic development of the eye, vision, and the visual pathway. Binocularity and stereopsis can only manifest if the eyes are accurately aligned. At this early age, infants are very sensitive to conditions that interfere with visual development. Common vision problems (e.g., uncorrected refractive errors, strabismus, and visual deprivation) present during this period of plasticity can cause a permanent reduction of stereoacuity by hampering the development of stereopsis. Early detection of these anomalies within the critical period carries high potential for recovery and normal vision development, because the potential to develop normal visual function seem to be inversely related to age.
Early research on infant binocular vision failed to separate monocular and binocular cues to depth. Owing to poor experimental design,
results described in those initial studies could be affected by monocular cues of depth or technical artifacts. Based on those results, consistent conclusions regarding the binocular component of depth perception could not be delineated. Subsequent studies were designed with the focus of increasing understanding of binocular cues. Further research was made more accurate by studying binocular cues in isolation from monocular ones, thus leading to more conclusive information.
results described in those initial studies could be affected by monocular cues of depth or technical artifacts. Based on those results, consistent conclusions regarding the binocular component of depth perception could not be delineated. Subsequent studies were designed with the focus of increasing understanding of binocular cues. Further research was made more accurate by studying binocular cues in isolation from monocular ones, thus leading to more conclusive information.
Ocular Alignment and Convergence
As the eyes track an object, they move in synchrony via yoked eye movements. This results in synchronous retinal images. When both foveae are directed toward the same target, a condition known as bifoveal fixation results. Similar retinal images and, hence, bifoveal fixation are thought to be required for binocular fusion and stereopsis. In preverbal infants, the development of bifoveal fixation has been studied indirectly by measuring ocular alignment and vergence control. Although ocular alignment and vergence control improves with age (3), several lines of evidence suggest that this is not the limiting factor on early binocular function. Early studies of ocular alignment suggested that infants often exhibit divergence (4,5), indicating a lack of bifoveal fixation and, thus, accounting for the lack of binocular function and stereopsis. This is in contrast to more recent findings that most newborn infants are orthotropic (6), thus indicating that cortical development, rather than ocular alignment, is the limiting factor on early binocular function.
Early eye alignment experiments conducted by Wickelgren (5) and Maurer and de Graaf (4) presented visual targets and recorded the relative position of the two pupil centers using corneal photography (5). Their research concluded that infant visual axes are generally diverged. This technique had a pitfall, however; it measured eye alignment with respect to the center of the pupil (optic axis), but did not take into account that the optical axis did not coincide with the visual axis (line from the target to the fovea). This optic axis-visual axis discrepancy is called the angle alpha. The results from their experiments, therefore, could be affected by errors in their methodology. Later in 1975, Slater and Findlay (7) concluded that binocular fixation was present at birth with a limited response to static targets (10 and 20 inches). Although the corneal photography method was used, previous limiting factor of the angle alpha was overcome by using an average correction method (2).
Interestingly, Aslin (8) provided evidence that inaccuracies in binocular fixation during early infancy are not the result of a divergence bias. The resting position of binocular alignment in infants and adults was estimated by obtaining photographic measures of interpupillary distance in total darkness. The mean dark vergence position in the adult group corres- ponded to a distance of approximately 100 cm. The mean dark vergence positions were 25 and 50 cm for infants aged 1 to 4 months and 6 to 18 months, respectively. Hence, these results provide evidence that young infants’ inade- quate convergence to near target distances is not the result of a divergence bias. Moreover, these results suggest that the young infants’ oculomotor system can most easily maintain binocular fixation at relatively near viewing distances. The correspondence between the optic-visual axis discrepancy and interocular separation during development and the validity of the estimates of dark vergence in infants is uncertain, however.
Although clinical observational reports indicate newborn infants often exhibit substantial eye turns, mostly exotropia (9), Hainline and Riddell (3) proposed that some eye turns were caused by the confusion of versions and vergences (as evaluated from a single photograph taken of an off-axis infant) as well as the large angle kappa of newborn infants. Angle kappa is the angle between the visual line, which connects the point of fixation with the nodal points and the fovea, and the pupillary axis, which is a line through the center of the pupil perpendicular to the cornea.
Thorn et al. (6) used the Hirschberg test to examine the ocular alignment in 34 healthy infants; they reported that most infants are orthotropic in the first month. This is in contrast with previous large sample (N = 1031–3316) studies that used the examiner’s face as a
fixation target as infants attend to a face better than to a light (10,11,12). Besides the large angle kappa of newborn infants, Thorn et al. (6) have found the task of judging the position of their own reflection from an infant’s cornea to be far more difficult than the Hirschberg test. Another confounding factor, when using the examiner’s face as a fixation target, is that the facial features on which the infant fixates change with age (3). In any case, all studies concur that a substantial proportion of newborns are orthotropic and that this proportion increases with age (13). Owing to the limited cooperation of infants, methods available to test ocular alignment prove to be insufficient. Hence, examiners have resorted to an indirect measure of ocular alignment.
fixation target as infants attend to a face better than to a light (10,11,12). Besides the large angle kappa of newborn infants, Thorn et al. (6) have found the task of judging the position of their own reflection from an infant’s cornea to be far more difficult than the Hirschberg test. Another confounding factor, when using the examiner’s face as a fixation target, is that the facial features on which the infant fixates change with age (3). In any case, all studies concur that a substantial proportion of newborns are orthotropic and that this proportion increases with age (13). Owing to the limited cooperation of infants, methods available to test ocular alignment prove to be insufficient. Hence, examiners have resorted to an indirect measure of ocular alignment.
To successfully fixate bifoveally, not only do the eyes need to be relatively well aligned in the stationary state, but they also need to be capable of changing its alignment in the appropriate direction should the object of interest move. To determine whether bifoveal fixation is a limiting factor for stereopsis, a number of researchers measured the ability of young infants to change their vergence in response to static and dynamic targets.
Using corneal photography, Aslin (14) recorded changes in binocular eye alignment in infants 1, 2, and 3 months of age in response to a luminous target that moved along the infant’s midline. In his experiments, angle alpha was not affected by changes in the target distance because the light creating the corneal reflection was created by the moving target itself, and was not a fixed light source as in previous experiments (5). The results indicated that infants have the ability to converge and diverge in the appropriate direction as early as 1 month of age, but they cannot consistently converge to near targets until 2 months of age. Moreover, as age increases, the ability to respond appropriately to faster target motion also increases (14).
Because disparity is a likely cue for the visual system to indicate the necessity for a change in convergence, Aslin (14) also observed the saccadic refixation response to wedge prisms, clinically known as the four-prism diopter base out test commonly used to test for foveal suppression. The introduction of a prism during bifoveal fixation induces a shift in the image of the target as viewed by the affected eye, thus creating diplopia. A typical response to the four prism-diopter base out test consists of biphasic eye movements: a saccade followed by a convergent movement. If the affected eye is suppressed, the disparity created by the prism is not detected, and no eye movement occurs. If suppression is not present, the affected eye detects the disparity created by the prism and diplopia results. Eye movements will then be initiated to realign the foveae to reattain fusion. A five- or ten-prism diopter wedge prism, which displaces the image 2.5° and 5° nasally, respectively, was placed alternately in front of each eye of infants 3, 4.5, and 6 months of age. Refixational eye movements in response to disparity induced by wedge prisms were not present consistently until 6 months of age. This agreed with earlier results by Parks (15), whose clinical reports indicate that saccadic response to a prism test was not present in infants until 4 to 6 months of age.
Birch et al. (16) examined the hypothesis of whether the development of vergence accounts for the onset of stereopsis by comparing the ages of onset for stereopsis with and without vergence requirements. The presentation of stimuli near the horopter, which is a geometric surface in visual space that passes through the point of bifoveal fixation and contains all corresponding retinal points where single vision results (Fig. 7.1), did not significantly alter the age of onset of stereopsis. Hence, the development of accurate vergence is not the limiting factor in the development of stereopsis, but rather, the onset of stereopsis is dependent on the development of neural mechanisms (16).
Moreover, Hainline and Riddell (3) measured monocular and binocular eye positions of 631 infants (aged 17–120 days) from photographic images of eyes when static targets were presented (25–200 cm). Many of even the youngest infants showed good ocular alignment, both monocularly and binocularly, although the youngest infants displayed the greatest variability in vergence. This suggests that oculomotor constraints are not a significant barrier to the development of higher forms of binocularity.
When infants are tested using tasks that require dynamic changes in vergence, a different picture emerges. Ling (17) moved a target
consisting of a black disc (2 inches in diameter) along the infant’s midline from a distance of 3 to 36 in (at 2 inches/second); she concluded that systematic vergence eye movements throughout the range of target distances employed do not appear until 7 weeks postnatally. Aslin (14) also reported that infants do not consistently converge to dynamic targets until 2 months of age, and do not converge without delay until 3 months. This is in agreement with the Coakes et al. (18) study where their results showed that convergence is well established by 3 months.
consisting of a black disc (2 inches in diameter) along the infant’s midline from a distance of 3 to 36 in (at 2 inches/second); she concluded that systematic vergence eye movements throughout the range of target distances employed do not appear until 7 weeks postnatally. Aslin (14) also reported that infants do not consistently converge to dynamic targets until 2 months of age, and do not converge without delay until 3 months. This is in agreement with the Coakes et al. (18) study where their results showed that convergence is well established by 3 months.
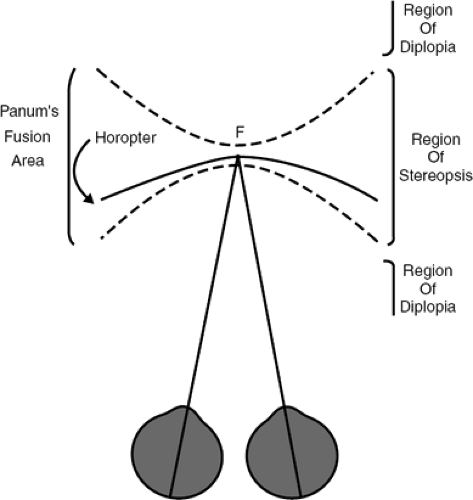 Figure 7.1 A schematic of an observer bifoveally fixating a point in space and the resulting specification of the horopter, Panum’s fusion area, the region of stereopsis and the region of diplopia. |
This discrepancy could result from the use of static versus dynamic targets. Studies that employ static targets (3) report good eye movement control, even in early infancy. When dynamic targets are used (14,17), however, few report good eye movement control, especially in the youngest infants. This suggests that different mechanisms could mediate static versus dynamic vergence and that these may have different developmental time courses during infancy. It is important to note that, although appropriate vergences are made in response to a near target, it is by no means suggestive of bifoveal fixation, but merely that the infant is fixating with consistent retinal points, which may or may not correspond to the fovea. Nevertheless, it appears that neural mechanisms, not bifoveal fixation (although necessary, but not limiting), are the limiting factor in the development of stereopsis.
Fusion
Fusion is the combining of two retinal images into a single percept. When the two foveae are aimed toward the same object in visual space, each eye receives similar stimulation and, thus, gives rise to a fused percept of an object. Beside the foveae, many retinal loci can yield fusion. These loci comprise the horopter. Single vision, however, can also occur at areas around the horopter, known as Panum’s fusion area (Fig. 7.1). This area for single vision is wider at the periphery. Any object located in front or behind Panum’s fusion area does not stimulate corresponding retinal points, resulting in diplopia.
The development of binocular single vision is accompanied by the development of oculomotor systems that function to keep images from the two eyes aligned. Binocular single vision is composed of sensory fusion and stereopsis. Fusion is often referred to as unification—a process by which the images formed on the retinas of the two eyes are combined into a single percept. As a prerequisite to achieve fusion, the eyes must be able to align themselves in such a manner that the retinal images of the fixated object can be easily placed and maintained on the fovea of the two eyes. Any object located outside of Panum’s fusion area while the subject is fixating on a target, does not stimulate corresponding retinal points, resulting in diplopia in the absence of suppression. As demonstrated by psychophysical and electrophysiologic measurements, human infants display a rapid onset of fusion at 3 to 5 months of age, which correlates with the development of stereopsis (19). To determine whether fusion is a prerequisite for stereopsis, fusion has been measured in normal healthy infants as well as in those with stra- bismus.
In normal healthy infants, fusion is not present at birth, but develops at approximately 3 months of age, corresponding to the development of stereopsis. To study the development of binocular function in infancy, Braddick and Atkinson (20) examined visual evoked potential
(VEP) induced by random dot patterns that alternated between correlated (fusible) and anticorrelated (rivalrous) states and found the median age at which binocular VEP first could be detected to be 11.4 weeks. Gwiazda et al. (21) determined the age of onset of fusion preference to be 12.4 weeks, and that female infants (9.9 weeks) developed fusion-rivalry discrimination earlier than male infants (13.8 weeks). In concordance with Gwiazda et al. (21), Thorn et al. (6) used forced-choice preferential looking (FPL) and found similar ages of onset of fusion (12.8 weeks) and that the shift of preference from rivalrous to fusible stimuli occurred during a brief period, often less than 2 weeks. Using both FPL and VEP protocols, which showed high concordance, Birch and Petrig (22) reported that few infants aged 2 to 3 months demonstrated fusion; most infants aged 5 months and older demonstrated fusion and reached adult levels by 6 to 7 months of age in 149 healthy, full-term infants. Together, studies on the ages of onset of fusion show close agreement. These findings suggest that sensory fusion is not present at birth but develops rapidly over the first 6 months of life.
(VEP) induced by random dot patterns that alternated between correlated (fusible) and anticorrelated (rivalrous) states and found the median age at which binocular VEP first could be detected to be 11.4 weeks. Gwiazda et al. (21) determined the age of onset of fusion preference to be 12.4 weeks, and that female infants (9.9 weeks) developed fusion-rivalry discrimination earlier than male infants (13.8 weeks). In concordance with Gwiazda et al. (21), Thorn et al. (6) used forced-choice preferential looking (FPL) and found similar ages of onset of fusion (12.8 weeks) and that the shift of preference from rivalrous to fusible stimuli occurred during a brief period, often less than 2 weeks. Using both FPL and VEP protocols, which showed high concordance, Birch and Petrig (22) reported that few infants aged 2 to 3 months demonstrated fusion; most infants aged 5 months and older demonstrated fusion and reached adult levels by 6 to 7 months of age in 149 healthy, full-term infants. Together, studies on the ages of onset of fusion show close agreement. These findings suggest that sensory fusion is not present at birth but develops rapidly over the first 6 months of life.
To determine the effect of anomalous visual experience on fusion capabilities, a number of studies examined fusion in children with early-onset infantile esotropia to gain insights into the sequence of events that lead to strabismus. Eizenman et al. (23) measured VEP responses to dynamic random dot correlograms (RDC) in children with early-onset esotropia before and after surgical alignment. Before surgical alignment, 38% of children showed detectable VEP responses (significantly different to age-matched normals), compared to 85% after surgery (not significantly different to age-matched normals), suggesting that children with early-onset esotropia have the capacity for fusion and that a congenital sensory fusion defect is not the cause of esotropia (23). Although the critical period for fusion development is longer than that of stereopsis (24




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
