Purpose
To assess whether optical coherence tomography angiography (OCTA) can be used as an alternative to conventional fundus fluorescein angiography (FFA) for the detection of myopic choroidal neovascularization (CNV).
Design
Validity and reliability analysis.
Methods
Twenty-eight eyes of 26 consecutive Japanese patients with exudative lesions associated with pathologic myopia were included in this institutional study. Myopic CNV was detected in 23 eyes of 22 patients; 5 eyes exhibited simple hemorrhage. The main outcome measure was CNV detection by OCTA and FFA. The CNV area was individually measured by FFA and OCTA. Intraclass correlation coefficients (ICCs) for the CNV area, independently measured by 2 investigators using OCTA and FFA, were determined.
Results
OCTA images with sufficient quality for CNV assessment were obtained for 17 eyes with CNV and 4 without. FFA alone detected CNV in all 17 eyes, while OCTA alone detected CNV in 16 (94.1%). The 1 eye for which CNV was not detected by OCTA exhibited a 0.01 mm 2 area on FFA. Both FFA and OCTA did not detect CNV in eyes with simple hemorrhage. The mean CNV areas on FFA and OCTA were 0.59 ± 0.56 mm 2 and 0.51 ± 0.55 mm 2 , respectively; the 2 values were significantly correlated ( P < .001, r = .86). The ICC (2, 1) values for FFA and OCTA were 0.944 and 0.997, respectively.
Conclusions
Our results indicate that OCTA can detect most myopic CNVs if high-quality images are acquired and can preclude the requirement for FFA in these settings.
When ophthalmologists identify patients with exudative lesions associated with pathologic myopia, they must determine the presence of choroidal neovascularization (CNV) to decide the treatment strategy. Fundus fluorescein angiography (FFA) has been used to detect CNVs and evaluate their activity. However, FFA is an invasive examination and results in varying degrees of patient discomfort, including anaphylactic reactions that can occur during and/or after FFA. A prospective study reported that 4.8% of patients who underwent angiographic procedures with intravenous fluorescein experienced adverse events, including nausea (2.9%), vomiting (1.2%), flushing/itching/hives (0.5%), and other reactions.
Recently, spectral-domain optical coherence tomography (SDOCT) was used for the examination of myopic CNVs. In 2006, Garcia-Layana and associates reported that the sensitivity of OCT B-scans for the detection of CNV activity once a diagnosis of CNV associated with pathologic myopia was established was approximately 97%. However, in 2013, despite considerable advancements in SDOCT technology, Leveziel and associates reported that the exudative features of myopic CNV are more obvious on FFA than on SDOCT, suggesting that FFA should be performed when new-onset myopic CNV is suspected. Thus, FFA continues to be the gold standard for initial CNV detection.
Compared with thermal laser photocoagulation and photodynamic therapy, intravitreal injections of vascular endothelial growth factor (VEGF) inhibitors allow for vision restoration in many patients with subfoveal myopic CNV. Because subretinal hemorrhage can be caused by both CNV and new lacquer crack formation in eyes with pathologic myopia, the presence of CNV should be confirmed prior to treatment initiation. Frequently, simple hemorrhage caused by new lacquer cracks spontaneously disappears without intervention. In addition to the existence of CNV, the lesion size should be precisely evaluated because it is negatively correlated with mean changes in vision after intravitreal anti-VEGF injections.
Recently, several research groups reported that optical coherence tomography angiography (OCTA) can detect CNV in patients with age-related macular degeneration (AMD). Because OCTA is noninvasive and allows for the direct visualization of blood vessels in vivo, it is a desirable tool. However, there is no prior study on OCTA for myopic CNV. Therefore, we conducted the present study to assess whether OCTA can be used as an alternative to conventional FFA for the detection of myopic CNV by comparing images obtained by the 2 modalities.
Methods
This study was approved by the ethics committee of Kyoto University Graduate School of Medicine (Kyoto, Japan). All study protocols adhered to the tenets of the Declaration of Helsinki. The nature of the study and the possible risks and benefits of participation were explained to all study candidates. All subjects choosing to participate provided written informed consent.
Subjects
Consecutive treatment-naïve patients with pathologic myopia (defined as a spherical equivalent of <−6.00 diopters and/or an axial length [AL] of >26 mm with chorioretinal abnormalities such as lacquer cracks, chorioretinal atrophy, and posterior staphyloma ) and exudative lesions who visited the Department of Ophthalmology and Visual Sciences at Kyoto University Graduate School of Medicine (Kyoto, Japan) between February 2015 and November 2015 were recruited for this study. All patients underwent comprehensive ophthalmologic examinations, including measurement of the best-corrected visual acuity (BCVA) using a decimal visual acuity chart (Landolt chart) and AL using an IOLMaster (Carl Zeiss Meditec, Inc, Dublin, California, USA). All BCVA data were converted to the logarithm of the minimal angle of resolution (logMAR) for statistical analyses. Indirect ophthalmoscopy, slit-lamp biomicroscopy, color fundus photography (TRC-NW8F; Topcon Corp, Tokyo, Japan), SDOCT (Spectralis HRA+OCT; Heidelberg Engineering, Heidelberg, Germany), FFA, indocyanine green angiography (ICGA) (HRA-2; Heidelberg Engineering), and OCTA (RTVue XR Avanti with AngioVue; Optovue, Inc, Fremont, California, USA) were also performed. OCTA images are obtained twice in approximately 3 seconds. Although OCTA images can be obtained without pupil dilation depending on the patient condition, we induced mydriasis before the procedure to obtain high-quality images. The inclusion criterion was as follows: presence of exudative lesions, including subretinal hemorrhage, serous retinal detachment, and retinal edema, associated with pathologic myopia diagnosed by retinal specialists using slit-lamp biomicroscopy, color fundus photography, and SDOCT. A total of 28 eyes with exudative lesions in 26 consecutive Japanese patients (22 women, 4 men) were eventually included. Among these, 23 eyes of 22 patients were diagnosed with myopic CNV (CNV group) and 5 eyes of the remaining 4 patients were diagnosed without CNV (simple hemorrhage group) by retinal specialists using biomicroscopy, color fundus photography, SDOCT, FFA, and ICGA.
Analysis of Choroidal Neovascularization With Fluorescein Angiography and Optical Coherence Tomography Angiography
All FFA images of the 28 eyes were independently evaluated by 2 investigators (M.M. and M.H.). CNV was defined by the presence of a hyperfluorescence on early-phase images that increased in size and intensity on late-phase images. The CNV area was measured on early-phase FFA images after correction for AL-related magnification by HRA-2 built-in software ( Figure 1 ).
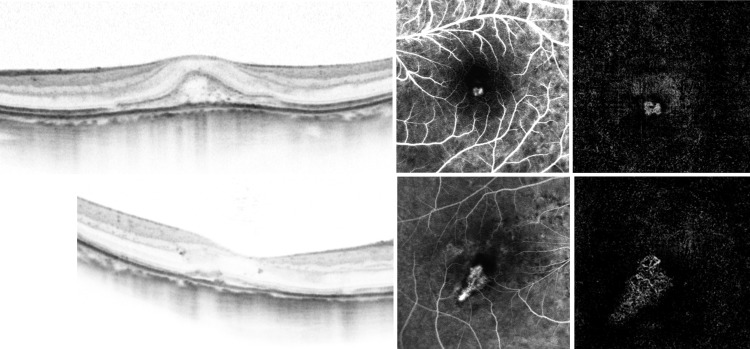
All OCTA images were obtained using RTVue XR Avanti with the AngioVue macular cube (3 × 3 mm) protocol. Each imaging cube comprised 304 clusters of repeated B-scans that contained 304 A-scans each. Retinal layer segmentation was automatically performed by the built-in software. Outer retinal level OCTA images were independently analyzed by 2 investigators to confirm the presence or absence of CNV. The CNV area was manually measured using ImageJ software (public domain software; National Institutes of Health, Bethesda, Maryland, USA; Figure 1 ). However, the RTVue XR Avanti system does not have a built-in correction system for AL-related magnification. Because the SDOCT scan area increases for eyes with a long AL, we had to consider adjusting the length of an image quadrant (304 pixels) on 1 side, particularly for eyes with high myopia in the present study. A square raster scan area measuring 10 × 10 degrees, which is equivalent to a square measuring 3 × 3 mm in the Gullstrand model eye, was used. The length on 1 side was corrected using AL, the flatter meridian, the steeper meridian, and the spherical equivalent refraction in the modified Littmann formula (Bennett formula).
Statistical Analyses
Data are presented as means ± standard deviations where applicable. All statistical analyses were performed using SPSS (version 21; IBM, Armonk, New York, USA). We used Student t tests or χ 2 tests to compare datasets as appropriate and analyzed correlations using Pearson rank correlation coefficients. Intraclass correlation coefficients (ICCs) for the area of CNV determined by the 2 investigators were calculated to determine the reliability of both OCTA and FFA measurements in 10 patients. A P value of <.05 was considered statistically significant.
Results
The characteristics of the study population are shown in Table 1 . The mean age was 64.9 ± 12.9 years and the mean AL was 28.62 ± 1.79 mm. There were no significant differences in sex, age, logMAR BCVA, AL, and lens status ( P = .31, P = .054, P = .074, P = .92, and P = .066, respectively) between the CNV and simple hemorrhage groups. Among the 28 eyes examined, OCTA images with sufficient image quality for CNV assessment were successfully obtained for 21 eyes of 20 patients, including 17 eyes in the CNV group and 4 eyes in the simple hemorrhage group. The quality of images was not sufficient for CNV assessment in 7 eyes of 6 patients, including 6 eyes in the CNV group and 1 eye in the simple hemorrhage group. There were no significant differences in sex, age, AL, lens status, and CNV status between the 2 groups ( P = 1.00, P = .18, P = .065, P = .65, and P = .78, respectively; Table 2 ). The visual acuity was significantly better in eyes with successful OCTA images than in those with poor-quality images ( P = .03). For subsequent analyses, we included the 21 eyes with high-quality OCTA images ( Table 3 ).
| CNV Group a | Simple Hemorrhage Group b | P | |
|---|---|---|---|
| N eyes (patients) | 23 eyes (22 patients) | 5 eyes (4 patients) | |
| Female sex, eyes (patients) | 19 eyes (18 patients) | 5 eyes (4 patients) | .31 |
| Age (y) | 67.0 ± 13.0 | 70.4 ± 7.7 | .054 |
| Visual acuity, logMAR | 0.505 ± 0.505 | 0.076 ± 0.196 | .074 |
| Axial length (mm) | 28.64 ± 1.98 | 28.55 ± 0.35 | .92 |
| Pseudophakia, eyes (patients) | 10 eyes (9 patients) | 0 eyes (0 patients) | .066 |
| Successfully Obtained Images Group a | Unsuccessfully Obtained Images Group b | P c | |
|---|---|---|---|
| N eyes (patients) | 21 eyes (20 patients) | 7 eyes (6 patients) | |
| Female sex, eyes (patients) | 18 eyes (17 patients) | 6 eyes (5 patients) | 1.00 |
| Age (y) | 63.0 ± 13.6 | 70.4 ± 7.7 | .18 |
| Visual acuity, logMAR | 0.263 ± 0.301 | 0.924 ± 0.618 | .03* |
| Axial length (mm) | 28.07 ± 1.05 | 30.27 ± 2.57 | .065 |
| Pseudophakia, eyes (patients) | 7 eyes (7 patients) | 3 eyes (2 patients) | .65 |
| N eyes (patients) with CNV | 17 eyes (17 patients) | 6 eyes (5 patients) | .78 |
a Successfully obtained images group: Optical coherence tomography angiography images were of high quality for CNV assessment.
b Unsuccessfully obtained images group: Optical coherence tomography angiography images were of low quality for CNV assessment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


