Purpose
To evaluate demographics and outcomes of patients with recurrent corneal erosions related to trauma and epithelial and Bowman layer disorders.
Design
Retrospective case series.
Methods
setting : Wills Eye Institute, Philadelphia, Pennsylvania. study population : Two hundred seventy-two eyes (230 patients) presenting between 2008 and 2011 with recurrent corneal erosions related to trauma and epithelial and Bowman layer disorders. procedure : Conservative management, diamond burr polishing, excimer laser phototherapeutic keratectomy (PTK), and epithelial debridement alone. main outcome measure : Recurrence of erosions, more than 6 weeks after commencing treatment.
Results
Mean age was 46.5 ± 14.6 (2-85) years. Female subjects accounted for 53% of patients and 18.3% had bilateral involvement. Etiology included epithelial basement membrane dystrophy in 52.9% (144/272) and trauma in 25.7% (70/272). One hundred sixty-six eyes with more than a single visit were initially managed conservatively, 68 of 166 (40.9%) had diamond burr polishing, 7 of 166 (4.2%) had PTK, and 4 of 166 (2.4%) had epithelial debridement alone. Many eyes had >6 weeks follow-up: 120 of 166 (72.3%) after conservative management, 54 of 68 (79.4%) after diamond burr polishing, 7 of 7 (100%) after PTK, and 4 of 4 (100%) after epithelial debridement. Percentage of eyes with recurrence was 56.7% (68/120) after conservative management, 14.8% (8/54) after diamond burr polishing, and 28.6% (2/7) after PTK. Rate of recurrence (eye-years) was 0.74, 0.19, and 0.23 with conservative management, diamond burr polishing, and PTK, respectively. Mild haze was seen in 22.2% of eyes (12 eyes) after diamond burr polishing and 28.6% (2 eyes) after PTK.
Conclusion
Recurrent corneal erosions are most commonly associated with epithelial basement membrane dystrophy. Patients are generally initially managed conservatively, with recurrence in more than half of eyes. Diamond burr polishing is the most common surgical intervention and is effective in a majority of eyes.
Recurrent corneal erosion syndrome, first described by Hansen, is characterized by episodes of spontaneous corneal epithelial defect with associated pain, photophobia, tearing, and blurring of vision. It is an entity very commonly encountered in clinical practice. It is frequently annoying for patients as their quality of life is hampered, and is occasionally visually and functionally debilitating. Additionally, it is frustrating for the ophthalmologist because of its moderately high recurrence rate despite treatment. There are various hypotheses regarding the pathogenesis of recurrent corneal erosions, which involve the defective adhesion of the epithelium to the underlying basement membrane. Abnormality of basement membrane, absent or abnormal hemi-desmosomes, and increased activity of matrix metalloproteinases (MMPs), especially MMP-2 and MMP-9, have been attributed to the pathogenesis of recurrent erosions. There is a wide range of therapeutic options to prevent recurrences; however, there is no definitive treatment. Medical management with topical lubricants, topical hypertonic saline, topical steroids, oral doxycycline, bandage contact lens, and autologous serum and surgical management with anterior stromal puncture (ASP) with needle or with neodymium–yttrium-aluminum-garnet laser (Nd:YAG), alcohol delamination of epithelium, mechanical epithelial debridement with or without diamond burr polishing, and excimer laser phototherapeutic keratectomy (PTK) have been reported in literature. In our study we describe the demographics, management patterns, and outcomes with conservative as well as surgical treatment modalities of the patients with recurrent corneal erosions attributable to trauma and epithelial and Bowman layer disorders who presented to our service in the past 4 years.
Patients and Methods
We performed a retrospective case series, based on a computer search of all the patients with recurrent corneal erosions in the electronic health records of Corneal Associates at Wills Eye Institute. All patients with a diagnosis of recurrent corneal erosions seen from January 1, 2008 to December 31, 2011 were identified. This study was approved by the Institutional Review Board of Wills Eye Institute, Philadelphia, Pennsylvania, USA and was conducted in adherence to the tenets of the Declaration of Helsinki. Patients with the diagnoses of stromal corneal dystrophies, herpetic epithelial defect, bullous keratopathy, and band-shaped keratopathy were excluded. Demographic data and etiology of the erosions were evaluated for all the eyes presenting with recurrent erosions, and management outcomes were evaluated for the eyes with at least 6 weeks of follow-up. Data collected included age, sex, eye involved, presentation (acute or with minimal symptoms), etiology, duration of symptoms, other ocular comorbid conditions, previous intervention, treatment given, recurrence of erosions, time to first recurrence, duration of follow-up, and complications. Recurrence of erosions was defined as either an episode of erosion on examination or an episode of severe symptoms suggestive of erosion on patient history. Patients with a single visit or with fewer than 6 weeks of follow-up were excluded for calculation of recurrences, in order to eliminate symptoms caused by incomplete epithelial healing after commencing treatment. Conservative treatment included a broad group of patients that were managed medically, with a single or combination therapy using topical lubricant drops or ointment, topical hypertonic saline drops or ointment, topical steroids, oral doxycycline, or bandage contact lens. Surgical management included simple epithelial debridement, epithelial debridement with diamond burr polishing of Bowman membrane, ASP, and PTK. The rate of recurrence was also calculated in eye-years, as the number of recurrences divided by the years of follow-up. Patients who complained of symptoms every day or every other day, without a recurrence-free interval, were counted as single recurrence. Kaplan-Meier survival analysis was done to calculate the cumulative recurrence-free survival after treatment.
Surgical Procedure
Diamond burr polishing
After instilling topical anesthesia and placing an eyelid speculum, at the slit lamp, 7-10 mm of central corneal epithelium was debrided with a cellulose sponge, blunt spatula, or #15 blade. A hand-held battery-driven diamond burr (5.0 mm diameter, model #0012; Surgimed-MLB, Newtown, Pennsylvania, USA) was used to gently and uniformly polish the Bowman membrane in the entire area of epithelial defect in a vertical fashion for approximately 10 seconds. A bandage soft contact lens was placed, which was removed following resolution of the epithelial defect (typically postoperative day 4-5) and antibiotic drops were given 4 times a day for 1 week.
PTK
After instilling topical anesthesia and placing an eyelid speculum, the central corneal epithelium was removed with a cellulose sponge, blunt spatula, or #15 blade. PTK was performed with VISX Star S4 laser (Advanced Medical Optics, Santa Ana, California, USA). The entire epithelial defect area was treated uniformly with a 5- to 6-μm depth ablation at 6 Hz. Postoperative treatment was similar to that after diamond burr polishing.
Epithelial debridement
After instilling of topical anesthesia and placement of an eyelid speculum, all loose epithelium was removed as described for diamond burr polishing. Postoperative management was similar to that after diamond burr polishing.
Eyes that demonstrated visually significant haze were treated with a tapering dose of steroid drops (fluorometholone 0.1% or loteprednol 0.5%) starting at 4 times a day for 4-6 weeks.
Results
Demographic Pattern
There were a total of 272 eyes of 230 patients. Mean age was 46.5 ± 14.6 years (range: 2-85 years). Females accounted for 53% (122/230) of patients. Bilateral involvement was seen in 18.3% (42/230) of patients and the right eye was involved in 57.4% (108/188) of patients with unilateral involvement.
Patient Characteristics
The etiology of recurrent erosions was epithelial basement membrane dystrophy in 52.9% of eyes (144/272 eyes), trauma in 25.7% of eyes (70/272 eyes), epithelial basement membrane dystrophy with history of trauma in 7.7% of eyes (21/272 eyes), other etiologies in 9.9% of eyes (27/272 eyes), and unknown in 3.7% of eyes (10/272 eyes). Other etiologies included Reis-Bücklers dystrophy in 8 eyes, corneal scar in 6 eyes, erosion post refractive surgery in 5 eyes, erosions after Nd:YAG peripheral iridotomy in 3 eyes, Stevens-Johnson syndrome in 2 eyes, epidermolysis bullosa in 2 eyes, and Meesmann dystrophy in 1 eye.
There were 106 eyes of 87 patients that had only a single visit, and thus were excluded from further analysis. Of the remaining 166 eyes, acute presentation was seen in 18.7% of eyes (31/166), and 81.3% eyes (135/166) had minimal to no symptoms on presentation but had a history of previous episodes or symptoms of erosion. Median duration of symptoms in all eyes before presentation to our service was 8 months (mean: 16.3 months, range: 0.06-156 months). Median duration of symptoms in eyes with epithelial basement membrane dystrophy was 7 months (mean: 16.7, range: 0.06-136 months). In eyes with traumatic etiology, median time from trauma to presentation to our service was 12 months (mean: 38.7, range 1-360 months). Thirty-two eyes (19.3%) had had previous surgical interventions: ASP in 10 eyes, epithelial debridement in 10 eyes, diamond burr polishing in 6 eyes, excimer laser PTK in 3 eyes, ASP and epithelial debridement in 2 eyes, ASP and PTK in 1 eye. Dry eye syndrome was present in 28.9% (48/166) of eyes and blepharitis in 24.7% (41/166) of eyes. Patients were grouped according to the treatment modality. The etiology and baseline characteristics in each group are outlined in Tables 1 and 2 .
| Conservative (n = 120) | Diamond Burr (n = 68) | PTK (n = 7) | Epithelial Debridement (n = 4) | ASP (n = 3) | |
|---|---|---|---|---|---|
| Epithelial basement membrane dystrophy | 61 (50.8%) | 37 (54.4%) | 0 (0%) | 3 (75%) | 0 (0%) |
| Trauma | 29 (24.2%) | 21 (30.9%) | 0 (0%) | 1 (25%) | 3 (100%) |
| Epithelial basement membrane dystrophy with trauma | 14 (11.7%) | 8 (11.7%) | 1 (14.3%) | 0 (0%) | 0 (0%) |
| Others | 13 (10.8%) | 2 (2.9%) | 6 (85.7%) | 0 (0%) | 0 (0%) |
| Unknown | 3 (2.5%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Conservative n = 120 | Diamond Burr n = 68 | PTK n = 7 | Epithelial Debridement n = 4 | ASP n = 3 | |
|---|---|---|---|---|---|
| Presentation (acute:chronic) | 20:100 | 14:54 | 0:7 | 2:2 | 1:2 |
| Duration of symptoms median (range), months | 12 (0.06-156) | 6.5 (0.2-36) | 12 (0.5-12) | 12 (4-24) | 1 (1-12) |
| Time from trauma, median (range), months | 15 (1-360) | 8 (1-180) | 24 | 2 (1-36) | |
| Previous surgery | ASP: 8 Epithelial debridement: 7 Diamond burr: 2 PTK: 4 | ASP: 6 Epithelial debridement: 5 Diamond burr: 5 PTK: 2 | Diamond burr: 1 PTK: 2 | Epithelial debridement: 1 | None |
| Follow-up, median (range), months | 9 (1.5-68) | 6 (0-53) | 9 (2-52) | 3 (1.5-12) | 1 |
Treatment Outcomes
Forty-six of 166 conservatively treated eyes (27.7%) had <6 weeks of conservative treatment. Of these 46 eyes, 35 eyes underwent diamond burr polishing, 1 underwent PTK, and 1 had epithelial debridement less than 6 weeks after starting the conservative treatment. Nine of 46 conservatively managed eyes were lost to follow-up. One hundred twenty of 166 eyes (72.3%) were followed up after more than 6 weeks of conservative treatment. Recurrence was observed in 56.7% of eyes (68/120 eyes). Rate of recurrence was 0.74/eye-year. Forty-four of these 120 eyes (36.7%) failed conservative treatment and subsequently underwent surgical intervention: diamond burr polishing in 33 eyes, PTK in 5 eyes, ASP in 3 eyes, and epithelial debridement in 3 eyes. In all, diamond burr polishing was done in 68 of 166 eyes (40.9%). Median duration of conservative treatment before diamond burr polishing was 1 month (mean 2.8, range 0-24 months). To calculate the recurrence rate, 54 of 68 eyes (79.4%) with >6 weeks of follow-up were analyzed. Recurrence was observed in 8 of 54 eyes (14.8%). Rate of recurrence was 0.19 eye-years. Additional procedures were done in 7.4% of eyes (4/54); 3 eyes had repeat diamond burr polishing and 1 eye had excimer laser PTK. Two of these 4 eyes had further recurrent symptoms.
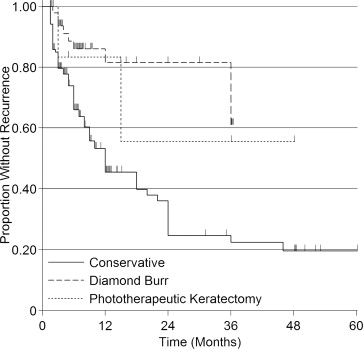
Excimer laser PTK was done in 7 of 166 eyes (4.2%), all of which had >6 weeks of follow-up. Recurrence was seen in 2 of 7 eyes. Rate of recurrence was 0.23 eye-years. One eye underwent repeat PTK and did not show further symptoms. Mechanical epithelial debridement was done in 4 of 166 eyes (2.4%); all had >6 weeks of follow-up. Recurrence was observed in 2 of 4 eyes. Rate of recurrence was 1.2 eye-years. Repeat procedures were done in 2 of these eyes; 1 had repeat epithelial debridement and 1 had diamond burr polishing, but further follow-up after the repeat procedures was not available. Anterior stromal puncture was done in 3 of 166 eyes (1.8%). All 3 eyes had less than 6 weeks of follow-up and were excluded from the calculation of recurrence of erosions. Kaplan-Meier survival analysis ( Figure ) shows the cumulative probability of recurrence-free survival of 81.5% at 1 year, 81.5% at 2 years, and 61.1% at 3 years with diamond burr polishing. With conservative management, recurrence-free survival was 45.5% at 1 year, 24.6% at 2 years, 22.4% at 3 years, and 19.6% at 4 and 5 years. The characteristics of the patients with or without recurrence after conservative treatment and diamond burr polishing are summarized in Table 3 .