Purpose
To investigate the frequency and types of systemic findings in patients with apparently isolated uveal coloboma.
Design
Cross-sectional observational study.
Methods
setting : Single-center ophthalmic genetics clinic. study population : Ninety-nine patients with uveal coloboma seen at the National Eye Institute. observational procedure : Results of audiology testing, echocardiogram, brain magnetic resonance imaging, renal ultrasound, and total spine radiographs. main outcome measure : Prevalence of abnormal findings on systemic testing.
Results
Uveal coloboma affected only the anterior segment in 8 patients, only the posterior segment in 23 patients, and both anterior and posterior segments in 68 patients. Best-corrected visual acuity (BCVA) of eyes with coloboma was ≥20/40 in 45% of eyes; 23% of eyes had BCVA of ≤20/400. The majority of patients (74%) had good vision (>20/60) in at least 1 eye. Ten of the 19 patients (53%) who underwent echocardiography had abnormalities, with ventral septal defects being the most prevalent. Abnormal findings were observed in 5 of 72 patients (7%) who had a renal ultrasound and in 5 of 29 patients (17%) who underwent a brain MRI. Audiology testing revealed abnormalities in 13 of 75 patients (17%), and spine radiographs showed anomalies in 10 of 77 patients (13%). Most findings required no acute intervention.
Conclusions
Although some patients with coloboma had evidence of extraocular abnormalities, the majority of findings on routine clinical examination did not require acute intervention, but some warranted follow-up. Results from the systemic evaluation of patients with coloboma should be interpreted with caution and in view of their clinical context.
Uveal coloboma is a rare eye malformation caused by failure of the optic fissure to close during the fifth to seventh weeks of fetal life. It has an estimated prevalence of 1 in 10 000 in the United States. A coloboma may appear as an isolated finding or as part of a broader systemic syndrome. The most common syndromic form of coloboma is the CHARGE syndrome, an acronym for c oloboma, h eart defects, a tresia choanae, r etarded growth and development, g enitourinary anomalies, and e ar anomalies/deafness. Important clinical features not reflected in the CHARGE acronym include orofacial clefts, facial palsies, and vestibular abnormalities. While many patients with syndromic forms of uveal coloboma will present clinically in infancy, the phenotypic spectrum is quite wide.
This broad phenotypic spectrum raises an important question for the practicing ophthalmologist and clinical geneticist, namely: in a new patient presenting with seemingly isolated uveal coloboma, are there additional systemic tests that should be completed to rule out a mild form of syndromic involvement?
In this study, we reviewed our 8 years of experience with comprehensive ocular and systemic phenotyping at the National Institutes of Health (NIH) Clinical Center of patients with uveal coloboma. The purpose of this study was to evaluate the yield of systemic testing, such as audiology, renal ultrasound, echocardiography, and neuroimaging, and the prevalence of non–clinically evident abnormalities among patients with uveal coloboma.
Methods
This was an observational, prospective cross-sectional study of patients who were seen at the National Eye Institute (NEI) between April 2004 and June 2012. Registration information is available at the National Institutes of Health database at http://www.clinicaltrials.gov (identifiers: NCT00076271 , NCT00368004 , NCT01778543 , and NCT000708955). The study was approved by the NEI Institutional Review Board or the Combined Neuroscience Institutional Review Board of the NIH, depending on the time frame. Informed consent/assent was obtained from the patients and/or their parents. The study conformed to all federal or state laws. All methods adhered to the tenets of the Declaration of Helsinki for research involving human subjects, and the study was conducted in accordance with Health Insurance Portability and Accountability Act regulations.
Because the purpose of this study was to assess the yield of systemic testing on patients presenting with coloboma to an ophthalmologist, subjects with CHARGE syndrome or another clearly identifiable syndrome were excluded from analysis ( Supplemental Table 1 , available at AJO.com ). Patients who appeared otherwise generally healthy, but who had abnormalities detected on specialized testing (such as karyotype), were also excluded. Some patients were excluded because of developmental eye abnormalities described as “coloboma” by the referring physician, but who had defects not related to optic fissure closure (eg, macular “coloboma”).
If available, existing outside medical records were reviewed and included in this analysis. Tests that had been previously performed and documented as normal were not repeated. A detailed history was obtained, including questions about birth, development, and family history. Ophthalmologic evaluation included assessment of best-corrected visual acuity (BCVA), ocular motility and alignment, anterior segment examination, and dilated funduscopy. For infants and developmentally delayed children who could not participate in formal visual acuity assessment, the ability of the patient to fix and follow, the presence of any ocular fixation preference, and/or binocular Teller visual acuity was noted. Because of the age of most participants, microphthalmia was judged by clinical examination, as axial lengths could only rarely be obtained. All patients were examined by the same pediatric ophthalmologist (B.P.B.).
Depending on the patient’s age, developmental status, cooperation, and history of previous testing, further systemic investigations were obtained. Systemic testing included audiology evaluation, brain magnetic resonance imaging (MRI), skeletal x-rays, echocardiogram, kidney ultrasound, routine blood chemistries including kidney and liver function testing, and urinalysis. After a preliminary analysis of approximately 60 subjects, some systemic testing (eg, echocardiography in the absence of a detectable heart murmur) was eliminated because of its low clinical yield. In addition, systemic testing was performed only on those individuals able to cooperate without sedation. As such, not every patient received every test.
Results
Patient Characteristics
A total of 99 patients with an initial diagnosis of nonsyndromic uveal coloboma were investigated in the NEI Ophthalmic Genetics Clinic over an 84-month period. The mean age at the time of initial examination was 9.5 years (range 4 months – 43 years). There were 52 female and 47 male patients. The majority of the patients (80%) were white. The remaining patients were Latino (9%), black or African-American (5%), Asian (5%), and American Indian (1%).
Ocular Findings
Of all 99 patients with uveal coloboma, bilateral involvement was observed in 71 patients (71%). Among the 28 patients with unilateral involvement, the right eye was affected in 15 patients and the left eye was involved in 13 patients. Among the 71 patients with bilateral involvement, 4 had bilateral anterior segment involvement (lens and/or iris) only, 14 had bilateral posterior segment involvement (optic disc and/or retina) only, and 53 had involvement of both the anterior and posterior segments. Twenty-one of the 71 patients with bilateral involvement had discordance of the location of coloboma between the 2 eyes. In 19 patients, 1 eye had only anterior involvement with both anterior and posterior segments involved in the fellow eye. Interestingly, only 1 patient had only posterior involvement in 1 eye and anterior and posterior involvement in the fellow eye; similarly, 1 patient had only anterior involvement in 1 eye and only posterior involvement in the fellow eye. Systemic anomalies appeared in approximately equal frequency between patients with bilateral and unilateral colobomas (42% vs 39%; odds ratio 1.1; 95% confidence interval 0.5-2.8; P = .78).
Visual acuity could not be quantitated in 33 patients because of either young age or developmental delay. Among the 66 patients in whom visual acuity could be assessed, 49 patients (74%) had good visual function (>20/60 in at least 1 eye), 8 patients (12%) were visually impaired (<20/60 but >20/200 in at least 1 eye), and 9 patients (14%) were legally blind (≤20/200 in the better eye). Visual acuity of the eye affected with coloboma ranged from 20/12.5 to no light perception (NLP). Most of the affected eyes had 20/40 or better vision ( Table 1 ). However, 27 of the 117 eyes (23%) analyzed were 20/400 or worse. Figure 1 depicts the visual acuities based on coloboma location. All eyes with only anterior segment involvement had vision ≥20/40. Eyes with combined retinal and optic disc involvement, as well as eyes that were microphthalmic, had a higher frequency of visual impairment.
| Visual Acuity | n (%) |
|---|---|
| ≥20/40 | 53 (45) |
| 20/50-20/70 | 11 (9) |
| 20/80-20/160 | 16 (14) |
| 20/200-20/300 | 10 (9) |
| ≤20/400 | 27 (23) |
| HM | 14 |
| CF | 3 |
| LP | 1 |
| NLP | 1 |
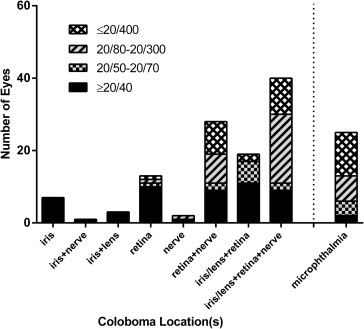
Eight patients (8%) had involvement of the anterior segment only, 23 patients (23%) had involvement of the posterior segment only, and the remaining 68 subjects (69%) had both anterior and posterior segment findings ( Table 2 ). Anterior segment-only findings included 7 patients with isolated iris coloboma and 1 patient with both iris and lenticular colobomas. Among the patients with isolated posterior segment involvement, chorioretinal coloboma was present in 3 patients and combined optic disc and chorioretinal colobomas were present in 20 patients. A total of 69 patients (153 eyes) had involvement of the optic nerve. Of these 153 eyes, the visual acuity could be measured in 106 eyes. Forty-one eyes (39%) had a visual acuity of 20/40 or better, 36 eyes (34%) had a vision of <20/40 but >20/400, and 29 eyes (27%) had a visual acuity of 20/400 or worse. Concurrent ocular abnormalities are summarized in Table 3 . In order of decreasing frequency, the most common coexisting ocular anomalies were microphthalmia (29%), strabismus (19%), cataract (15%), microcornea (14%), and nystagmus (14%).
| Location of Coloboma | Unilateral Involvement | Bilateral Involvement | Total |
|---|---|---|---|
| Anterior segment, n/N (%) | 8/99 (8) | ||
| Iris | 3 | 4 | 7 |
| Lens | 0 | 0 | 0 |
| Iris and lens | 1 | 0 | 1 |
| Posterior segment, n/N (%) | 23/99 (23) | ||
| Optic disc | 0 | 0 | 0 |
| Retina | 2 | 1 | 3 |
| Optic disc and retina | 6 | 14 | 20 |
| Anterior and posterior segments, n/N (%) | 68/99 (69) | ||
| Iris and optic disc | 1 | 0 | 1 |
| Iris and retina | 6 | 8 | 15 |
| Iris, optic disc, and retina | 3 | 33 | 36 |
| Iris, lens, retina | 0 | 5 | 5 |
| Iris, lens, optic disc, retina | 7 | 5 | 12 |
| Total | 28 | 71 | 99 |
| Other Ocular Disorders | Total, n/N (%) |
|---|---|
| Microphthalmia | 29/99 (29) |
| Microcornea | 14/99 (15) |
| Amblyopia | 10/99 (10) |
| Nystagmus | 14/99 (14) |
| Cataract | 15/99 (16) |
| Anisometropia | 1/99 (1) |
| Retinal detachment | 1/99 (1) |
| Fetal vascular remnant | 6/99 (6) |
| Strabismus | 18/99 (19) |
| Esotropia | 14 |
| Exotropia | 2 |
| Mixed | 2 |
Physical Examination and Developmental Status
A detailed physical examination was performed either by the pediatric or internal medicine service at the NIH or by the patient’s own physician. Thirty-three patients had their examination done at the NIH. Table 4 lists the details of the significant findings, which included growth retardation, failure to thrive, developmental delay, dysmorphic features, and skin findings. When identifiable syndromes were excluded, the dysmorphic features did not follow any specific pattern. High-resolution karyotype was initially performed on 36 patients; 3 had abnormal results, but these were excluded from this analysis, given that they were clearly syndromic patients. As such, we discontinued sending karyotype on apparently nonsyndromic patients.
| Finding | n/N (%) |
|---|---|
| Growth abnormalities | 2/99 (2) |
| Failure to thrive | 1 |
| Retarded growth | 1 |
| Macrocephaly | 1/99 (1) |
| Dysmorphic features | 13/99 (13) |
| High-arched palate | 4 |
| Single palmar crease | 1 |
| Midfacial hypoplasia | 1 |
| Bifid thumb | 1 |
| Pectus excavatum | 1 |
| Incomplete Sydney crease | 1 |
| Craniosynostosis | 1 |
| Hypotonic face | 1 |
| Small jaw | 1 |
| Epicanthal folds | 1 |
| Skin findings | 7/99 (7) |
| Sacral dimple | 2 |
| Preauricular skin tags | 1 |
| Ear tags | 1 |
| Macular hyperpigmented lesion on occipital scalp | 1 |
| Capillary hemangioma on thigh | 1 |
| Forehead telangiectasia | 1 |
| Developmental delay | 16/99 (16) |
| Speech | 6 |
| Motor | 6 |
| Speech and motor | 4 |
Among the 16 patients with reported developmental delay, 3 patients (19%) had posterior colobomas and 13 patients (81%) had both anterior and posterior colobomas. Fourteen of the 16 patients (88%) had bilateral disease. There was not a statistically significant difference between coloboma laterality and developmental delay (Fisher exact test, P = .22). Among the 20 eyes affected with coloboma in the 16 patients with developmental delay, 8 eyes (40%) had visual acuities of >20/40, while 6 eyes (30%) had visual acuities of <20/200. Microphthalmia was observed in 5 patients (31%), and cardiac, urogenital, and central nervous system anomalies were present in 25% (4/16), 19% (3/16), and 38% (6/16) of the patients with developmental delay, respectively. There was no clear correlation between coloboma morphology and the presence of specific systemic findings.
Echocardiography
Of the 19 patients who were examined by echocardiography, 10 patients (53%) had cardiac anomalies ( Table 5 ). Seven individuals had a single finding: ventricular septal defect (VSD) (3 patients), atrial septal defect (ASD) (2 patients), mitral valve prolapse (1 patient), and patent foramen ovale (PFO) (1 patient). The other 3 patients each had 2 cardiac abnormalities: ASD and patent ductus arteriosus (PDA), pulmonary stenosis and PFO, and pulmonary stenosis and ASD. Three patients underwent cardiac surgical repair during infancy: 2 for ASD and 1 for VSD. In all cases, the abnormalities were ascertained in infancy and based on historical records.
| Abnormal Finding | n/N (%) |
|---|---|
| Cardiac abnormalities | 10/19 (53) |
| VSD | 3 |
| ASD | 2 |
| Mitral valve prolapse | 1 |
| PFO | 1 |
| ASD/PDA | 1 |
| Pulmonary stenosis/PFO | 1 |
| ASD/VSD | 1 |
| Urogenital abnormalities | 5/72 (7) |
| Bilateral hydronephrosis | 1 |
| Small left kidney with multiple small cysts | 1 |
| Slightly small left kidney | 1 |
| Cyst in left kidney | 1 |
| Missing left kidney | 1 |
| Skeletal abnormalities | 10/77 (13) |
| Osteopenia | 4 |
| Missing 2 thoracic vertebrae | 1 |
| Fused C2-C3 vertebrae | 1 |
| Spina bifida occulta T8 | 1 |
| Small left cervical rib | 1 |
| Missing T12 ribs | 1 |
| Incomplete blocked vertebrae at C6-C7 | 1 |
| Brain abnormalities | 5/29 (17) |
| Single focal subcortical white matter abnormality in right frontal lobe | 1 |
| Increased T1 signal in cerebellum | 1 |
| Prominent perivascular spaces | 1 |
| Small arachnoid cyst in left middle cranial fossa | 1 |
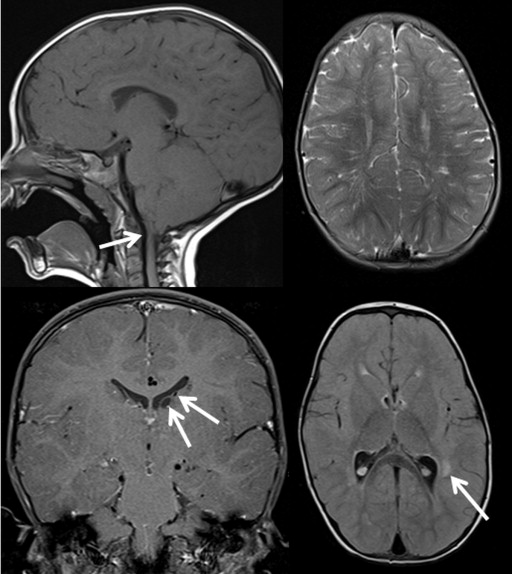
| 6-mm descent of cerebellar tonsils to C1 arch; prominent perivascular spaces; delayed myelination; periventricular white matter lesion of L temporal lobe; 2 L subependymal cysts | 1 |
| Audiology findings | 13/75 (17) |
| Bilateral conductive hearing loss | 5 |
| Unilateral conductive hearing loss | 5 |
| Bilateral mixed hearing loss | 1 |
| Bilateral sensorineural hearing loss | 2 |
Renal Ultrasonography
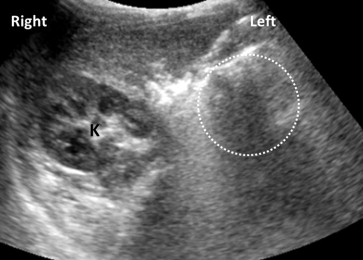
Renal ultrasonography was performed on 72 patients. Five patients (7%) had abnormal findings ( Table 5 ). The abnormal findings were bilateral hydronephrosis, slightly small kidney, small kidney with multiple cysts, absent kidney ( Figure 2 ), and a 6-mm cyst in the kidney. Blood pressure measurements taken during their NIH visit and laboratory analyses for blood urea nitrogen and creatinine were within normal limits for age and sex.
Spinal X-ray
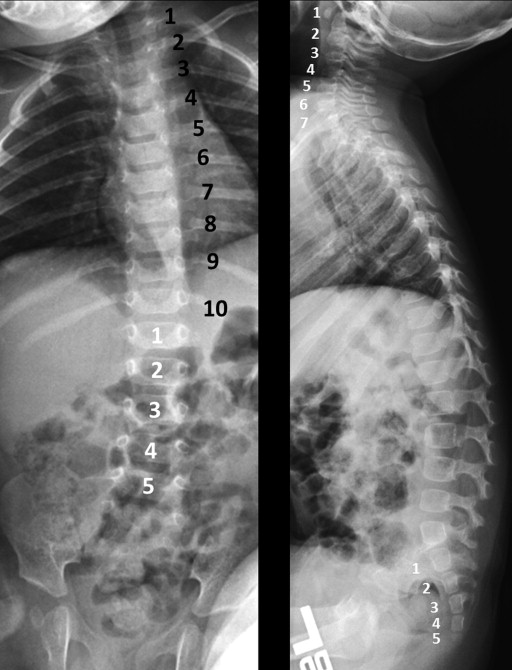
Skeletal or vertebral abnormalities were noted in 10 of the 77 patients (13%) who underwent imaging. Table 5 summarizes these findings, which included osteopenia and fused cervical vertebrae (Klippel-Feil anomaly).
In 2 unrelated and nonconsanguineous families, vertebral anomalies appear to co-segregate with uveal coloboma ( Supplemental Figures 1 and 2 , available at AJO.com ). In these families, vertebral findings include missing vertebral ribs ( Figure 3 ), scoliosis, transitional vertebra, and spina bifida occulta. Coloboma appears to be incompletely penetrant and exhibits variable expressivity in individuals from Family 1, several of whom were found to have variants of the spinal bones, particularly in those subjects who linked the 2 affected lineages in this family. In both families, an autosomal-dominant pattern of inheritance seems most likely, although an X-linked inheritance pattern could not be excluded based on the pedigree in Family 2. The proband in Family 2 was missing a kidney as well. A similar finding was reported, but not verified, in 2 individuals from Family 1: one has coloboma, while the other is the son of a female subject with a missing vertebra. Linkage analysis was unsuccessful in determining a possible locus for this coloboma-spine association. Whole exome sequencing analysis is currently in progress.
Brain Magnetic Resonance Imaging
A brain MRI was performed in 29 patients. The mean age of these patients was 7.2 years (range 4 months – 27 years). Anomalies of the central nervous system were documented in 5 patients (17%). The mean age of the patients with anomalies was 10.9 years (range 3.1-34.7 years). The findings are documented in Table 5 . One patient had multiple findings, including type 1 Chiari malformation, prominent perivascular spaces, periventricular white matter lesions, and subependymal cysts ( Figure 4 ). This patient also had speech and motor developmental delay.