Purpose
To report a large consecutive case series of patients who developed delayed-onset and acute-onset endophthalmitis after cataract surgery.
Design
Retrospective consecutive case series.
Methods
The current study is a retrospective consecutive case series of patients treated between January 2000 and December 2009 for culture-proven endophthalmitis after cataract surgery. The study defined 2 groups after cataract surgery: acute-onset endophthalmitis (≤6 weeks after surgery) and delayed-onset endophthalmitis (>6 weeks after surgery).
Results
A total of 118 patients met study criteria; cases included 26 delayed-onset cases and 92 acute-onset cases. The following clinical features and outcomes occurred in delayed- vs acute-onset cases: 1) the presenting visual acuity was ≤5/200 in 31% vs 89%; 2) hypopyon was found in 46% vs 80%; 3) the most frequent isolate was Propionibacterium acnes (11/26) vs coagulase-negative Staphylococcus (57/92); and 4) patients with the most frequent isolate achieved a visual outcome of ≥20/100 in 91% vs 56%. In delayed-onset cases, the intraocular lens was removed or exchanged in 19 of 26 cases (73%). Of these 19 cases, 13 achieved a visual outcome of ≥20/100.
Conclusions
Patients with delayed-onset endophthalmitis generally presented with better initial visual acuities, had a lower frequency of hypopyon, and had better visual outcomes compared to acute-onset patients. Propionibacterium acnes and coagulase-negative Staphylococcus species were the most common organisms cultured in delayed- and acute-onset categories, respectively, and were associated with the best visual acuity outcomes in each group.
Endophthalmitis is a serious sight-threatening condition that can be classified into 2 broad categories: acute-onset and delayed-onset. As used in the Endophthalmitis Vitrectomy Study, acute-onset postoperative endophthalmitis was defined as infections within 6 weeks of surgery. By contrast, delayed-onset postoperative endophthalmitis has been defined as greater than 6 weeks after the surgery. These 2 categories may differ in their incidence, clinical features, microbiology, and visual acuity outcomes.
The reported incidence of acute-onset endophthalmitis after cataract surgery ranges from 0.03% to 0.15%. Since the mid-1990s, cataract surgical techniques have evolved to clear corneal, sutureless techniques. In spite of this change in technique, the nature of acute-onset endophthalmitis in both settings is virtually identical. Acute-onset postoperative endophthalmitis is characterized by a rapid onset of visual loss and marked intraocular inflammation and is frequently caused by coagulase-negative Staphylococcus .
In 1 single-center study, the reported rate of delayed-onset endophthalmitis following cataract surgery was 0.017%. In delayed-onset postoperative endophthalmitis, the onset is frequently insidious and the inflammation is often low grade, and is caused by less virulent bacteria and fungi. Propionibacterium acnes has been reported to be a common organism isolated in published series.
The purpose of the current study was to compare the clinical features, causative organisms, and visual acuity outcomes associated with delayed-onset vs acute-onset endophthalmitis after cataract surgery in a contemporary series from a university referral center.
Methods
The clinical and microbiology records were reviewed for all patients treated at Bascom Palmer Eye Institute between January 1, 2000 and December 31, 2009 for clinically diagnosed, culture-positive endophthalmitis following cataract surgery. The study included patients who were operated elsewhere and referred for care, as well as patients who underwent cataract surgery at Bascom Palmer Eye Institute. Patients were excluded from the study if the endophthalmitis was not associated with cataract surgery or if consequent to combined procedures (glaucoma and cataract surgery). Patients with preexisting macular degeneration, diabetic retinopathy, or glaucoma were not excluded from the study.
Intraocular fluid specimens were plated directly on chocolate agar, 5% sheep blood agar, CDC anaerobic blood agar, Sabouraud agar, and thioglycolate medium. Chocolate and blood agar plates and thioglycolate broth were incubated for up to 2 weeks at 35 C in 5% CO 2 . Anaerobic plates were incubated in an anaerobic jar in non-CO 2 for up to 2 weeks. Sabouraud agar was incubated at 35 C for 72 hours and then at 25 C for up to 2 weeks. To be considered a positive culture, a specimen must have demonstrated growth of the same organism on 2 or more solid culture media or growth on a single medium after identification on an initial smear.
Because the current study was a retrospective case series, there was no rigid protocol for managing these patients, although the practice algorithm is fairly consistent for all investigators. Intravitreal antibiotics were injected at the time of initial treatment in all patients. The use of vitrectomy was at the discretion of the treating physician, although the guidelines of the Endophthalmitis Vitrectomy Study (EVS) were generally followed for acute-onset cases. Recorded data included clinical features, visual acuity at diagnosis, cultured organisms, and visual acuity at follow-up.
Results
Between January 1, 2000 and December 31, 2009, 118 patients met study criteria. Of these 118 patients, 26 (22%) had delayed-onset postoperative endophthalmitis and 92 (78%) had acute-onset postoperative endophthalmitis ( Tables 1 and 2 ). In this study, 71 of the 118 cases (60%) were from male patients and 47 (40%) were from female patients. The mean age at presentation was 74 years (range 52–87, SD 9) in the delayed-onset group and 76 years (range 48–90, SD 9) in the acute-onset group.
| Total n = 118 | VA ≤ 5/200 | Hypopyon | Mean Days to Diagnosis |
|---|---|---|---|
| Delayed-onset (n = 26) | 8 (31%) | 12 (46%) | 343 (median: 230, range: 48–1840) |
| Acute-onset (n = 92) | 82 (89%) | 74 (80%) | 9 (median: 7, range: 1–39) |
| Total n = 118 | ≥20/40 | ≥20/100 | ≤5/200 | NLP |
|---|---|---|---|---|
| Delayed-onset (n = 26) | 50% | 65% | 27% | 12% |
| Acute-onset (n = 92) | 27% | 41% | 35% | 4% |
Delayed-Onset Postoperative Endophthalmitis
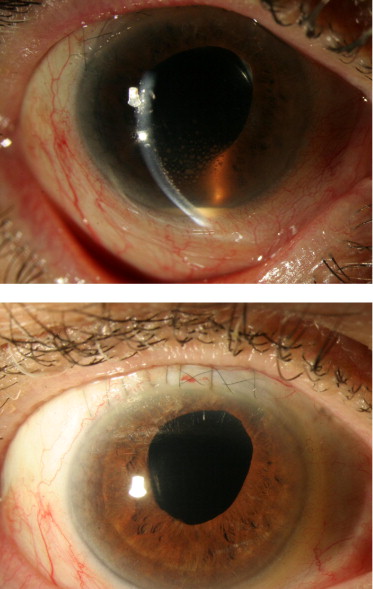
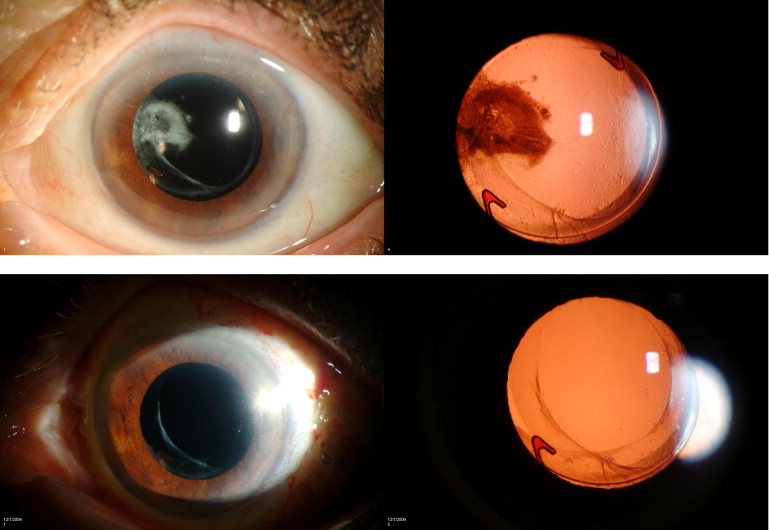
The mean time between surgery and the diagnosis of endophthalmitis was 343 days (range 48–1840, SD 379). Intraocular cultures became positive on days 2 to 7 after obtaining the specimen (mean time to culture positivity: 3.5 days). The average follow-up time after initial treatment was 804 days (range 61–3069, SD 774). A presenting visual acuity of ≤5/200 was noted in 8 of 26 patients (31%). Hypopyon was present in 12 of 26 patients (46%), and keratic precipitates were present in 19 of 26 patients (73%) ( Figure 1 ) . A white plaque associated with the capsular bag was noted in 17 of 26 patients (65%) ( Figures 2 and 3 ) . In the 26 delayed-onset cases, the following organisms were isolated: Propionibacterium acnes in 11 (42%), fungal species in 7 (27%), gram-negative species in 3 (12%), gram-positive species in 3 (12%), and Mycobacterium chelonae in 2 (8%).
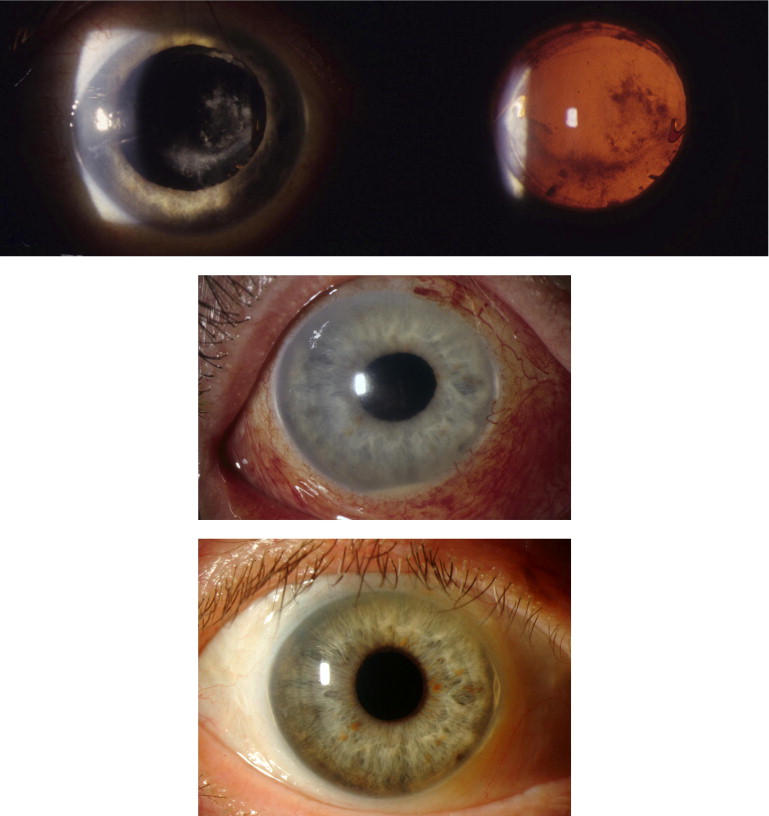
Initial treatment consisted of 3 different strategies: 1) vitreous tap and injection of intraocular antibiotics; 2) 3-port pars plana vitrectomy (PPV) with injection of intraocular antibiotics; and 3) 3-port pars plana vitrectomy with partial posterior capsulectomy and injection of intraocular antibiotics. No patients underwent initial treatment with total capsulectomy, intraocular lens (IOL) exchange, or IOL removal. However, 19 of 26 delayed-onset patients (73%) subsequently underwent combinations of these procedures because of recurrence of inflammation ( Figure 4 ) .
Of these 19 patients who underwent exchange or removal of the IOL, initial treatment included injection of intraocular antibiotics in 2, PPV with intraocular antibiotics in 8, and PPV with partial capsulectomy and intraocular antibiotics in 9. Seventeen of 19 patients (89%) underwent PPV with total capsulectomy and IOL removal or exchange as a secondary procedure. Only 2 of these 17 patients (12%) developed recurrence, which was managed by PPV with IOL removal in 1 patient and penetrating keratoplasty for keratitis in the other patient. Two patients who underwent PPV as a secondary procedure developed recurrence, which was treated with PPV, total capsulectomy, and IOL removal. In patients without recurrence, removal or exchange of the IOL was often the last procedure used to eliminate the infection.
Seven of 26 patients (27%) did not undergo exchange or removal of the IOL. Initial treatment in these patients included injection of intraocular antibiotics in 1, PPV with intraocular antibiotics in 2, and PPV with partial capsulectomy and intraocular antibiotics in 4. None of these patients had further recurrences or interventions after initial treatment.
Visual outcomes were ≥20/100 in 17 of 26 (65%) and ≤5/200 in 7 of 26 (27%) of delayed-onset patients. The distribution of visual outcomes according to the various isolates is displayed in Table 3 . Clinical features, presenting visual acuity, and visual outcomes of delayed-onset patients classified by those who underwent IOL exchange or removal are shown in Table 4 and Figure 4 .
| Delayed-Onset Endophthalmitis | ||||
|---|---|---|---|---|
| Total n = 26 | ≥20/40 | ≥20/100 | ≤5/200 | NLP |
| Propionibacterium acnes (n = 11) | 55% | 91% | 9% | 0 |
| Fungal species a (n = 7) | 57% | 57% | 29% | 0 |
| Mycobacterium chelonae (n = 2) | 50% | 50% | 50% | 50% |
| Gram-negative species (n = 3) | 0 | 0 | 67% | 33% |
| Other gram-positive species (n = 3) | 67% | 67% | 33% | 33% |
| Acute-Onset Endophthalmitis | ||||
|---|---|---|---|---|
| Total n = 92 | ≥20/40 | ≥20/100 | ≤5/200 | NLP |
| Coagulase-negative Staphylococcus (n = 57) | 38% | 56% | 13% | 0 |
| S. aureus (n = 11) | 0 | 0 | 100% | 0 |
| Streptococcus species (n = 8) | 0 | 0 | 67% | 33% |
| Other b (n = 16) | 11% | 22% | 67% | 11% |
a Fungal species include Candida parapsilosis (3), Aspergillus fumigatus , Penicillum citrinum , Paecilomyces variotti , Acremonium strictum .
| Patient | Eye | Days to Diagnosis | Organism | Visual Acuity at Diagnosis | Hypopyon | Keratic Precipitates | Visual Outcome |
|---|---|---|---|---|---|---|---|
| Delayed Onset Endophthalmitis With IOL Removal | |||||||
| 1 a | OD | 278 | Propionibacterium acnes | 20/60 | Y | Y | 20/25 |
| 2 | OD | 256 | Propionibacterium acnes | 5/200 | Y | Y | 20/20 |
| 3 a | OD | 476 | Propionibacterium acnes | 20/100 | N | N | 20/30 |
| 4 | OD | 735 | Propionibacterium acnes | 20/150 | N | Y | 20/80 |
| 5 a | OD | 127 | Propionibacterium acnes | 20/30 | N | Y | 20/40 |
| 6 a | OS | 808 | Propionibacterium acnes | 20/80 | N | Y | 20/60 |
| 7 | OS | 714 | Propionibacterium acnes | 20/40 | N | Y | LP c |
| 8 a | OD | 210 | Propionibacterium acnes | 20/40 | N | Y | 20/70 |
| 9 | OS | 331 | Candida parapsilosis | 20/200 | N | Y | 20/400 |
| 10 | OS | 125 | Candida parapsilosis | CF | N | Y | 5/200 |
| 11 | OD | 133 | Candida parapsilosis | 20/200 | N | Y | 20/25 |
| 12 | OD | 250 | Acremonium strictum | 20/200 | N | Y | 20/30 |
| 13 | OS | 125 | Aspergillus fumigatus | 20/60 | Y | Y | 20/20 |
| 14 | OD | 716 | Paecilomyces variotti | CF | Y | N | 5/200 |
| 15 b | OD | 154 | Mycobacterium chelonae | 20/30 | Y | Y | 20/25 |
| 16 | OS | 57 | Mycobacterium chelonae | 20/400 | Y | Y | NLP d |
| 17 | OD | 276 | Agrobacterium radiobacter | HM | Y | Y | LP |
| 18 a | OD | 202 | Staphylococcus epidermidis | 5/200 | Y | Y | 20/15 |
| 19 | OS | 104 | Staphylococcus epidermidis | 2/200 | Y | N | 20/40 |
| Delayed Onset Endophthalmitis Without IOL Removal | |||||||
| 20 | OS | 126 | Propionibacterium acnes | 20/50 | N | Y | 20/25 |
| 21 | OD | 111 | Propionibacterium acnes | 20/50 | N | Y | 20/100 |
| 22 | OS | 381 | Propionibacterium acnes | 20/40 | N | N | 20/25 |
| 23 | OD | 258 | Penicillum citrinum | 20/60 | N | Y | 20/30 |
| 24 | OD | 73 | Ewingella americana | 20/400 | Y | N | 20/300 |
| 25 | OS | 1840 | Haemophilus influenzae | LP | Y | N | NLP |
| 26 | OD | 48 | Streptococcus intermedius | LP | Y | N | NLP |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


