First “wall”: Orbital fat
2–3 mm
Second wall: Lateral wall
3–6 mm
Third wall: Medial wall
4–7 mm
Fourth wall: Orbital floor
5–9 mm
Fig. 11.1
General conceptual frameworks for preoperative planning for TED patients
Customizing Orbital Decompression
Graded Axial Proptosis Reduction: Type of Disease (Fat vs. Muscle Predominant)
Determination of disease type is the first step in creating a customized plan for orbital decompression. Clinical examination and orbital imaging both aid to categorize a patient’s disease as fat or muscle predominant. As stated before, many patients may demonstrate expansion of both tissues. Patients with fat predominant disease typically have more proptosis, and reduced rates of diplopia and compressive optic neuropathy as compared to patients with muscle predominant disease [14]. Furthermore, patients with fat predominant disease generally have reduced resistance to retropulsion. On CT scan, proptosis is observed without substantial enlargement of extraocular muscles. In such patients, isolated fat decompression can significantly reduce axial proptosis with minimal risk of consecutive diplopia. Heterogenous fibrosis of orbital fat may influence the decompressive effect; however, this has not yet been fully elucidated. Figure 11.2 demonstrates the computed tomography (CT) scan of a patient with fat predominant disease. Notably, the extraocular muscles appear to be of normal caliber on imaging. This patient underwent bilateral orbital fat decompression, with significant improvement in proptosis and symptoms of exposure keratopathy. An improvement in inferior scleral show was also noted, thus obviating the need for lower lid retraction repair (Fig. 11.2c, d). In cases where fat decompression alone is not sufficient to achieve the desired degree of proptosis reduction (for example in cases with significant fibrosis of fat or severe proptosis), it can be combined with bony decompression of the lateral orbital wall for additional proptosis reduction with minimal postoperative risk of diplopia.
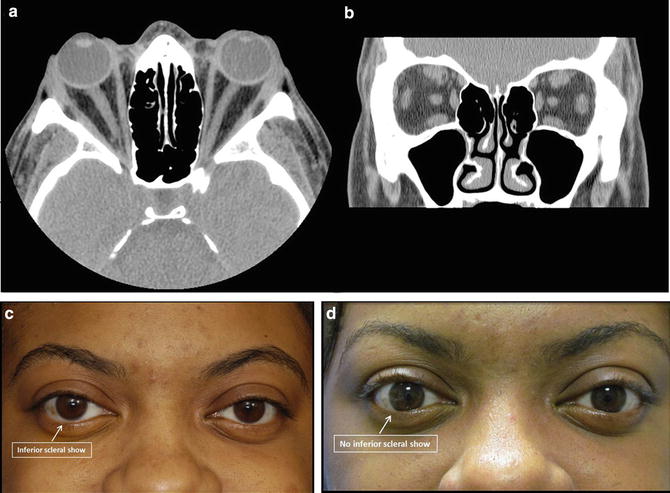
Fig. 11.2
Axial (a) and coronal (b) non-contrast CT scans of a 27 year-old woman with fat predominant TED. Note proptosis without significant enlargement of extraocular muscles. External photographs of the patient before (c) and after (d) orbital fat decompression. Note improvement in lower eyelid retraction following decompression
In cases of muscle predominant disease, fat decompression is rarely used as an isolated procedure to decompress the orbit. This is due to the fact that fat decompression may be more technically challenging due to minimal fat expansion, variable fibrosis of fat, potentially increased risk for muscle injury due to enlargement, and propensity for bleeding related to increased orbital congestion and dilation of vasculature. Therefore in these cases, removal of bone is generally always performed in the stepwise approach as listed in Table 11.1, while also taking into consideration the individualized factors in Fig. 11.1. If the patient has no preoperative diplopia and mild to moderate exophthalmos (less than 6 mm), fat and lateral wall (including deep, lateral orbit) decompression is a preferred surgical approach as it provides excellent proptosis reduction while minimizing postoperative diplopia. In cases of severe exophthalmos (greater than 6 mm) where “maximal” axial proptosis reduction is required, one may consider additional decompression of the medial wall despite the increased risk for diplopia. Although this modified “3 wall” (balanced bone and fat) decompression poses an increased risk for diplopia compared to lateral and fat decompression, the risk appears to be less than traditional 3 wall bony decompression of the orbital floor, medial and lateral walls [13]. Furthermore, sparing of the anterior orbital strut provides a “ledge” for the globe, preventing inferomedial globe dystopia [15].
If additional axial proptosis reduction is required, removal of the deep portion of the frontal bone in the superolateral orbit can be performed to maximize the decompressive effect, as shown in the CT scan in Fig. 11.3. This can also be performed through an eyelid crease incision during standard lateral decompression, obviating the need for craniotomy. In this manner the bone surrounding the superior orbital fissure (greater wing of sphenoid and frontal bones) can be removed in entirety baring dura and substantially expanding orbital volume.
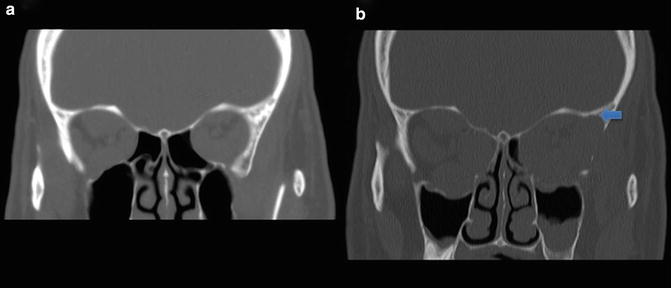
Fig. 11.3
Pre (a) and postoperative (b) coronal CT scan of a patient with TED. The patient underwent right medial decompression for CON and left lateral and medial wall decompression. Note the removal of bone in the left superolateral quadrant, as marked by the arrow
Restrictive Strabismus
As previously discussed, postoperative diplopia is one of the most bothersome complications following orbital decompression. Patients must be counseled regarding the relative risk based upon muscle predominant disease, surgical approach(es), etc. Patients with pre-existing strabismus often require multidisciplinary counseling and planning prior to orbital decompression. A tentative plan for strabismus surgery including the laterality of surgery and the proposed muscles is helpful to plan decompression surgery to ensure symmetry in the final stages. Most commonly, recession of extraocular muscles for TED related restrictive strabismus is performed, though rarely muscles may be resected. Recession of extraocular muscles may lead to worsening axial proptosis [72]; therefore, the surgeon should take into consideration any future plans for muscle recessions, and “over” decompress on the side(s) of the planned strabismus surgery in anticipation of such shifts. In our practice, we generally plan 1–2 mm of additional decompression for patients who will be undergoing recession of extraocular muscles.
Patients with restrictive strabismus typically have muscle predominant disease, most commonly involving the inferior and medial recti muscles. Patients with large muscles exhibit congestive features and often derive substantial benefit from removal of the posteromedial orbit, including the palatine and ethmoid bones during medial wall decompression. Decompression of the posterior orbit yields substantial decompressive effect and has the additional benefit of reducing congestive orbitopathy. Of note, the anterior strut is spared to minimize postoperative globe dystopia and diplopia.
Increased Interpupillary Distance
Widening of the IPD is a subtle, but not uncommon, finding in patients with GD and should not be overlooked as it may contribute to the altered facial morphology of TED. Due to the nonparallel, divergent nature of the lateral orbital walls, axial proptosis is accompanied by increased IPD, an acquired form of hypertelorism. Many astute patients notice the facial alteration especially when accompanied by cheek or buccal fat hypertrophy. Enlargement of the medial rectus muscle may also contribute to lateral globe displacement. Isolated lateral bony decompression often does not adequately address this finding, and therefore careful review of photographs is critical prior to surgery for operative planning (Fig. 11.4). Balanced medial and lateral wall decompression can be considered in such cases, with a nasal shift in globe position achieving a result similar to the patient’s pre-morbid appearance [16].





Fig. 11.4
External photograph of a 59 year old woman with TED. Note progressive nonaxial globe displacement (left to right) leading to increased interpupillary distance
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
