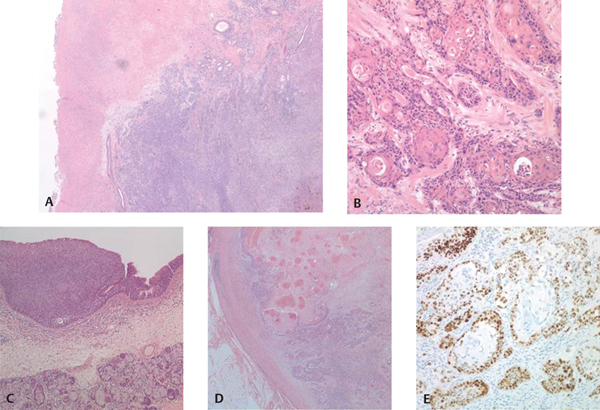
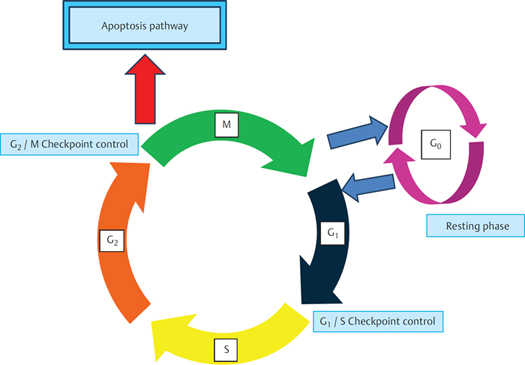
5 Current Perspectives on the Molecular Biology of the Larynx Although the larynx may be the site of origin for many different types of cancer, squamous carcinomas account for 95% of cases.1 While the incidence of laryngeal carcinoma is increasing in some areas of the world, there are still notable geographic variations and epidemiological trends in the incidence. Laryngeal cancer is most commonly diagnosed in individuals over the age of 60, with diagnoses below the age of 40 being uncommon. In the United Kingdom, laryngeal cancer is the 18th most common type of cancer affecting men, with a male:female ratio of approximately 5:1 based on figures from 2008. The incidence of this form of cancer has remained approximately 1 in 100,000 for women. There has been some variation in the incidence of laryngeal carcinoma in men, but over the past 30 years the incidence in the United Kingdom has been between 5 and 7 per 100,000 and recently has remained around 5.3 per 100,000.2 Laryngeal Cancer •Squamous carcinomas account for 95% of cases of laryngeal malignancies. •Laryngeal cancer is most commonly diagnosed in individuals over the age of 60, with diagnoses below the age of 40 being uncommon. •Incidence in the United Kingdom has been between 5 and 7 per 100,000. •Male:female ratio is approximately 5:1. The development of laryngeal squamous cell carcinoma (SCC) may be viewed in the same manner as the paradigm for stepwise carcinogenesis defined by significant pathological and molecular rate-limiting steps in cellular proliferation, described originally for colorectal carcinoma.3 As with sporadic colorectal carcinoma, the epidemiological data are compatible with cumulative exposure to carcinogenic agents that result in neoplastic transformation of cell(s) within the laryngeal epithelium. It is proposed that laryngeal SCC emerges after a prolonged period of time during which there is an accumulation of genetic abnormalities within a transformed cell and its progeny consequent upon the action of carcinogenic agents. As a result, the affected cells acquire morphologically identifiable changes. An initial hyperplastic phase is followed by a period during which the affected epithelial cells exhibit cytological changes associated with architectural disarray of variable severity within the epithelium that the pathologist recognizes as dysplasia. Such dysplastic lesions are represented by a spectrum of lesions that can be collectively termed squamous intraepithelial lesions. These changes could progress further as within the abnormal cell population the increasing mutational load may lead to the emergence of a clone of cells with invasive properties, thus heralding the onset of SCC. Stepwise Carcinogenesis •The development of laryngeal SCC may be viewed in the same manner as the paradigm for stepwise carcinogenesis defined by significant pathological and molecular rate-limiting steps in cellular proliferation, described originally for colorectal carcinoma.3 •The epidemiological data are compatible with cumulative exposure to carcinogenic agents that result in neoplastic transformation of cell(s) within the laryngeal epithelium. •Dysplastic lesions are represented by a spectrum of lesions that can be collectively termed squamous intraepithelial lesions. •Increasing mutational load may lead to the emergence of a clone of cells with invasive properties, thus heralding the onset of SCC. These models of cancer development are likely to represent a rather simplistic view for what is an incredibly complex process. Indeed the paradigm of colorectal carcinoma now reflects this notion as it is now evident that the original model does not seem to apply in all cases. In this particular system, it is now accepted that there are distinct routes by which various molecular alterations can be acquired within cells, leading ultimately to the onset of malignancy.3–5 It seems likely that a similar argument could be advanced for laryngeal SCC, especially as now several important and distinct etiological factors have been recognized. Furthermore, with regard to the larynx, although the model systems proposed might suggest that lesions will necessarily progress to SCC, it is evident that this need not be the case, particularly for lesions showing relatively minor histological abnormalities. Nevertheless, it is equally well recognized that in some cases lesions with low-grade histological change can progress rapidly to invasive disease.6 However, an important challenge for clinicians at this time is to appreciate which lesions are likely to progress to malignancy and over what time frame might this occur. Having an awareness of environmental factors that might perpetuate these events may offer further scope for intervention that will moderate or attenuate progression of the disease. Many environmental factors have been linked to the development of laryngeal squamous carcinomas. Foremost among these and the most widely recognized are smoking and alcohol usage, and in virtually all populations, most cases of SCC occur in patients with a history of tobacco use and consumption of alcohol. These two risk factors have a synergistic influence on the risk of developing laryngeal SCC. Smoking carries a greater risk of developing carcinomas arising from the glottis compared with other regions of the larynx. Conversely, alcohol consumption has stronger associations with carcinomas arising in the supraglottis and hypopharynx.1,7 The body of evidence that now links smoking to laryngeal SCC is overwhelming, and many studies have shown that the risk of developing laryngeal SCC in smokers is proportional to the number of years over which an individual smokes, the degree to which the patient inhales their smoke, and the type of tobacco used. Smoking traditionally is associated with an increased risk of mutational events affecting genes (Fig. 5.1), such as p53 that would predispose the cell to further errors of proliferation culminating in the development of cancer.8 The role of alcohol is less clearly understood, but it has been proposed that it acts as a promoter, driving the proliferation of abnormal cells and thus also accelerating the acquisition of further abnormalities. Figure 5.1 Squamous cell carcinoma of the larynx arises as a result of an accumulation of genetic damage within laryngeal squamous epithelial cells. Such tumors may present as locally advanced disease with ulcerated lesions of the vocal cord with underlying infiltration of the structures of the laryngeal wall by squamous carcinoma (A and B). However, it is well established that hyperplastic and dysplastic lesions precede the onset of overt malignancy (C). With invasive growth and progression of disease, lymph node metastasis may occur (D). In many laryngeal squamous carcinomas, mutation of the p53 gene can be interred by the strong nuclear staining of the malignant cells for p53 protein using immunohistochemical staining (E). Such staining techniques can be used to investigate molecular events that may have led to malignant transformation of epithelial cells or provide clues to the etiology of some cancer types, for example, nuclear staining for p16 may indicate underlying infection with human papillomavirus (not shown). However, several other environmental factors (dietary and occupational exposure to dusts and chemicals) have been linked with the risk of developing laryngeal SCC. Overall, it is likely that these will either be much less commonly identified in patients with SCC and/or a causal association with individual cases of SCC will be difficult to prove. Nevertheless, an extremely unusual condition associated with laryngeal SCC is worthy of note. Patients with Bloom syndrome appear to have an increased risk of developing laryngeal SCC.9 This condition is a rare autosomal recessive genetic disorder caused by mutations in BLM, a member of the RecQ deoxyribonucleic acid (DNA) helicase family.10 A characteristic feature of this condition is the accumulation of chromosomal abnormalities associated with chromosomal breaks and high rates of sister chromatid exchange. Although a rare association with laryngeal SCC in young patients, this condition provides a clear link between chromosome breakage, genetic damage, and the onset of malignancy at this site. This consolidates the popular models of carcinogenesis that propose that environmental carcinogens cause cancer in exposed cell populations by generating or facilitating an accumulation of genetic damage, that is, aberrations, of the tumor suppressor genes and oncogenes within cells, which is associated with an increased mutational load with consequent ability to drive the cells along the cell cycle (Fig. 5.2) and preventing their entry into the resting phase (Go). These acquired mutations are responsible for the genetic infidelity that allows the cancer cells to bypass the natural control through apoptosis. Two other factors that have recently gained wide interest are infection with high-risk serotypes of the human papillomavirus (HPV) and laryngopharyngeal reflux (LPR) disease. These factors are of particular interest as they may account for most cases of laryngeal SCC in the subgroup of patients without any history of smoking or alcohol intake; therefore, it may point toward different and important molecular events and pathways that might be implicated in the etiology of laryngeal SCC. Figure 5.2 Simplified sketch of the cell cycle and its various phases. Progression through the cell cycle is dependent upon the sequential activation and degradation of cyclin/cyclin-dependent kinase complexes. Cyclin D/cdk4/6 activity early in G1 gives way to cyclin E/cdk2 toward the G1/S transition. Progression through the S and G2 phases is associated with cyclin A/cdk2 activity, with cyclin B/cdk1 operating through mitosis. In addition, the cell cycle checkpoints must be permissive for progression to the next phase of the cell cycle. Restrictions are present in both the S phase and mitosis, but key tumor suppressor pathways operate at G1/S and G2/M. At the former, activation of p53 increases expression of p21 leading to arrest of the cells in G1. In addition, sequestration of E2 promoter binding factor transcription factors by the retinoblastoma protein will prevent entry to S phase. The tumor suppressor p53 also operates at the G2/M transition, its effects here being mediated by 14–3-3σ. G1+S+G2 = Interphase; M = Mitosis; S phase = DNA synthesis phase. Note: (1) DNA damage can activate apoptosis pathways as well as pathways that act at key checkpoints to mediate cell cycle arrest. (2) Cancer cells do not enter the G0 phase. High-risk serotypes of HPV, particularly HPV 16, have been linked to carcinomas arising at various sites within the head and neck region, with the highest viral load being consistently identified within tonsillar tissue. This is consistent with studies that show that the strongest and clinically the most significant associations of HPV infection are with tonsillar carcinoma as well as those arising in the oral cavity.11 In clinical terms, identification of HPV-associated cases of oropharyngeal squamous carcinoma is relevant; tumors associated with HPV have characteristic histological appearances, are often associated with strong expression of surrogate marker p16, are particularly responsive to chemotherapy/radiotherapy, and, paradoxically, have a relatively favorable prognosis.12 However, HPV does not carry the same degree of risk at all sites within the regions of the oral and upper aerodigestive tract, although it has been suggested that HPV may also be an important etiological factor for laryngeal carcinoma. There is considerable debate within the published literature regarding the frequency with which cases of laryngeal SCC are associated with HPV infection. Depending on the individual study, the frequency with which HPV is claimed to be associated with laryngeal SCC ranges from 3 to 85%. It might be argued that different techniques or reagents used in different studies could account for this striking variability in the results obtained, and the criteria by which cases are defined as HPV positive or negative may vary. Furthermore, it has been shown that in normal appearing larynges, both clinically and histologically, molecular evidence of HPV infection has been found in up to 25% of cases, which is a very intriguing finding indeed. Human Papillomavirus •High-risk serotypes of HPV, particularly HPV 16, have been linked to carcinomas arising at various sites within the head and neck region, with the highest viral load being consistently identified within tonsillar tissue. •Clinically the most significant associations of HPV infection are with tonsillar carcinoma as well as those arising in the oral cavity.11 •Tumors associated with HPV have characteristic histological appearances, are often associated with strong expression of surrogate marker p16, are particularly responsive to chemotherapy/radiotherapy, and, paradoxically, have a relatively favorable prognosis.12 Despite all of these caveats, a meta-analysis of cases reported in the literature suggests that about one quarter of cases of laryngeal SCC may be HPV related.11 Therefore, the prevailing opinion that HPV plays a relatively minor role in laryngeal SCC seems validated, but equally the role of HPV cannot be discounted, and consideration of the molecular events involved in HPV-related carcinogenesis will have some relevance to laryngeal SCC. However, laryngeal papillomatosis (recurrent respiratory papillomatosis) is an uncommon but well-recognized condition associated with HPV infection and yet malignant transformation in this setting is uncommon and most often associated with other recognized predisposing factors, such as smoking or following irradiation.13 This suggests that HPV infection may be a cofactor in the progression to malignancy but in and of itself may not be sufficient to cause laryngeal SCC, although certain viral serotypes (types 11, 16, and 18) appear to be associated with more aggressive disease and an increased risk of progression to malignancy. The role of LPR in the pathogenesis of laryngeal carcinoma has also now gained wider recognition. Since early reports linking reflux diseases to the onset of laryngeal neoplasia and the increased risk of laryngeal carcinoma for patients after gastric surgery, it is interesting to note that in those cases of laryngeal carcinoma occurring in patients without exposure to the major risk factors of smoking and alcohol, evidence of reflux disease is now often identified.14 Furthermore, reflux disease is associated with alcohol intake, raising the possibility that these factors may act synergistically as cofactors in laryngeal carcinogenesis. Laryngopharyngeal Reflux •The role of LPR in the pathogenesis of laryngeal carcinoma has also now gained wider recognition. •Reflux disease is associated with alcohol intake, raising the possibility that these factors may act synergistically as cofactors in laryngeal carcinogenesis. •In combination with acid, pepsin is believed to be a prime cause of injury to the laryngeal epithelium. •Scientific studies have recognized that the composition of the refluxate is complex (Fig. 5.3) and have sought to define which component(s) of the refluxate have a pivotal role driving the onset and progression of esophageal neoplasia. •Bile acids and their salts have gained wider recognition as agents implicated in the pathogenesis of a variety of cancers of the gastrointestinal (GI) tract.29,32,45
Etiological Factors for Laryngeal Squamous Cell Carcinoma
Established Etiological Factors
New Concepts in Laryngeal Carcinogenesis
Human Papillomavirus Infection
Laryngopharyngeal Reflux
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


