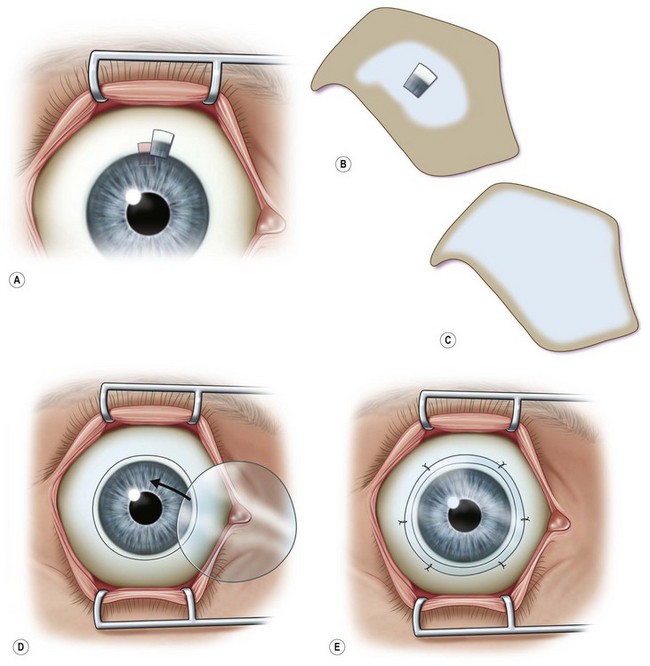
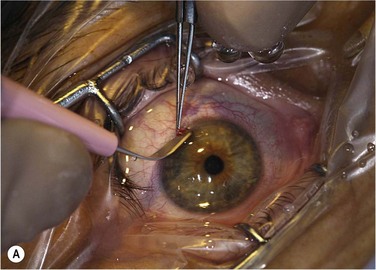
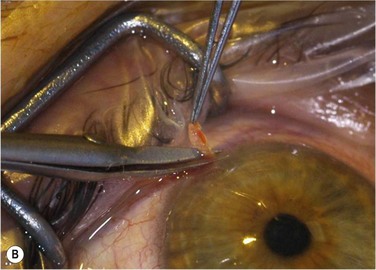
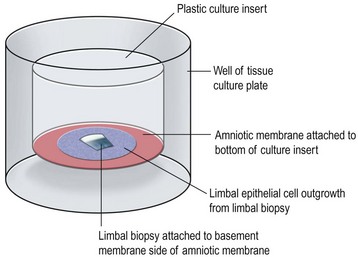
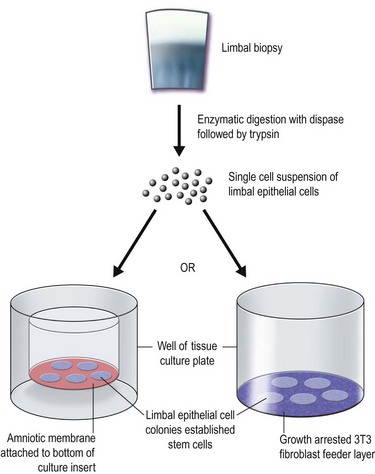
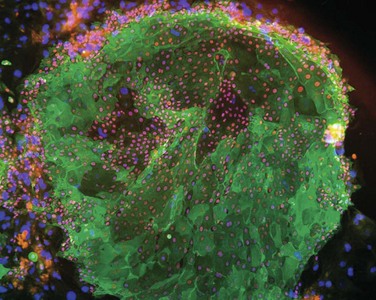
44 The possibility to serially propagate limbal epithelial stem cells (LESCs) in the cell culture laboratory has made these cells amenable to further study in vitro, but has also been used as a therapeutic approach. Cultivated sheets of LESCs can be transplanted with the aim of reconstructing a stem cell-deficient corneal surface. A recent study followed 112 patients with ocular surface disease due to corneal burns which received transplantation of autologous LESCs expanded on a fibrin gel. Clinical success (defined as a transparent, avascular and stable corneal surface) was seen in more than 75% of the study eyes.1 Cultured limbal epithelium has also been used to treat other causes of limbal stem cell deficiency with varying success rates.2 Although there is currently a lack of evidence to show that transplantation of cultivated LESCs is superior to conventional techniques involving whole limbal tissue transplants, there are theoretical advantages. In this chapter, the authors outline the concept and practice of cultured LESCs for reconstruction of the corneal surface and provide an overview of its current clinical significance and potential. Transplantation of healthy limbal tissue for treatment of total limbal stem cell deficiency can be obtained from the contralateral eye,3,4 a relative of the patient, or from the eye of a cadaveric donor. There is a very low risk for the healthy eye of a living donor unless repeated limbal biopsies are required. Therefore, the concept of ex vivo expansion of LESCs is regarded as a potential beneficial to increase cell yields prior to transplantation, allowing the size of the limbal biopsy to be reduced (Figs 44.1, 44.2). In exceptional cases, using this technique, autologous LESCs can also be obtained from a small, healthy region of a partially stem cell-deficient eye.5 In addition, cultured sheets of allogeneic epithelium have been purported to be less prone to immune rejection, since antigen-presenting cells are deemed to be absent following cell culture. Human corneal epithelium was first grown successfully in culture in 1977. This was made possible by the use of the 3T3 co-culture method, which had been described 2 years earlier by Rheinwald and Green.3,4 They reported that in the presence of mouse embryonic 3T3 fibroblasts, which had been growth-arrested by irradiation, single epithelial cells showed clonal expansion and could be serially propagated in vitro. However, it was not until 20 years later that transplantation of autologous, cultured limbal epithelial cells was shown to be beneficial in clinical cases of limbal stem cell deficiency. In 1997, Pellegrini and coworkers successfully transplanted cultured cell sheets obtained from autologous limbal tissue in two patients with alkali burns. Since then, numerous studies have focused on transplantation of cultured limbal epithelium.6,7 These interventions were performed in a number of different conditions, using different culture systems and yielding varying, yet promising results (see below). Currently it remains unclear what the precise mechanisms are by which grafting cultivated LESCs contributes to ocular surface healing. One would expect transplanted LESCs to improve the corneal surface by replenishing the depleted stem cell pool. However, Daya et al.8 determined the genotype of corneal epithelial cells following their transplantation to the corneal surface in humans, and were unable to detect donor DNA from as early as 1 month postoperatively. This may mean that rather than integrating into the recipient corneal surface (re-integration theory), transplanted corneal epithelium may allow or actively stimulate the recovery of an endogenous stem cell population (biological bandage theory). The two main techniques available for isolation and ex vivo expansion of corneal epithelium are the explant culture system and the somewhat more common suspension culture system. The former consists of placing a piece of limbal tissue (e.g. 2×2 mm) in culture as a whole (Fig. 44.3). The latter uses enzymatic digestion to remove the epithelial cells from the limbal tissue (Fig. 44.4). In this system, dispase is most frequently used to digest the epithelial basement membrane, while trypsin is employed subsequently to disrupt intercellular adhesions, producing a suspension of epithelial cells. Epithelial outgrowth from the explant or clonal growth around single isolated LESCs can be observed when appropriate culture conditions are being used (see below). Favorable clinical results have been obtained in a number of studies using either isolation strategy, and although limbal epithelial cell suspensions may contain a higher proportion of stem cells, clinical superiority of either of the two methods has not been formally established.2 Baylis et al. have proposed that impression cytology should be performed on the donor eye to rule out subclinical LESC deficiency, which could be made manifest by performing a limbal biopsy or which may predict culture failure.6 Also, several studies have suggested an uneven distribution of LESCs along the limbus.9 Knowledge regarding the localization of LESCs is important for targeting limbal biopsies to stem cell-rich regions. Most frequently, LESCs have been proposed to be more abundant in the superior and inferior limbal regions. However, the lack of definitive markers for unequivocal identification of LESCs continues to hamper the development of efficient methods not only for isolation, but also for propagation and delivery of LESCs. When cells are harvested from a living donor, the limbal palisades should be identified, and a specimen of 1–6 mm2 is obtained under local anesthesia (see Fig. 44.2). Although this technique maximizes the yield of clonogenic LESCs and therefore, the chances of successfully initiating an LESC culture, it remains unknown whether it also has a positive effect on the clinical performance of the graft. In a similar vein, where cadaveric corneal tissue needs to be relied upon, the duration of storage of ocular tissue in the eye bank has been suggested to negatively influence the rate of successfully initiating LESC cell culture; however, this has not been shown to affect the suitability of successfully established cell sheets for transplantation.2 Likewise, characteristics of tissue donors may influence attachment, survival and proliferation of LESCs. It has been reported that donor age has an influence on putative limbal stem cell markers, as well as morphological niche parameters, and that colony forming efficiency of LESCs declines with age.10,11 Additionally, it has been shown that corneal wound healing is impaired in diabetes mellitus, and limbal basal cells from diabetic human donors have been suggested to express fewer putative stem cell markers than those from normal subjects.12 This exemplifies that LESCs may be affected by systemic disease present in the donor. Again, whether this is likely to affect culture and transplantation of human limbal epithelial cells remains to be determined. Transplantation of limbal epithelium is deemed a stem cell therapy. This notion is supported, for instance, by the observation that a minimum of 3000 transplanted putative limbal stem cells was associated with a higher success rate in patients with ocular surface disease due to chemical and thermal burns.1 However, expanded limbal epithelial cell sheets contain a considerable fraction of differentiated daughter cells (Fig. 44.5). Also, LESCs have only a finite life span when propagated in culture, although one of the most important features describing stem cell populations is that of indefinite self-renewal. The current conception is that the maintenance of limbal stem cells is governed by a number of intrinsic, but also extrinsic factors, the latter of which are provided in vivo by the local microenvironment present at the corneoscleral limbus. Rather than being a mere transition zone between cornea and sclera, the limbus provides some unique anatomical specializations that are believed to be important for maintaining the stem cell population (see Chapter 5). In addition to a protective limbal anatomy, signals received from extracellular matrix and surrounding cells are believed to contribute to regulating LESC function and fate. For instance, extracellular matrix components were found to be expressed differentially in different areas of the ocular and corneal surface and may play a role in regulating LESC proliferation and differentiation.13 Likewise, soluble factors secreted by limbal fibroblasts have been proposed to have regulatory effects on limbal basal epithelium. The notion of adjacent structures and cells influencing stem cell behavior corresponds well to what has been termed the ‘stem cell niche.’ A system which removes LESCs from their niche to expand the cells for transplantation will need to replicate the stem cell niche in order to retain ‘stemness’ of the cells. In the first two cases of cultured LESC transplantation reported by Pellegrini and coworkers, transfer of the cultured epithelial sheet to the recipient ocular surface was performed using petroleum gauze in one patient, while a soft contact lens served as a carrier in the other. Subsequent works have frequently used fibrin gels. These gels have been shown to support LESC growth and attachment in culture, while they are degraded within 24 hours following transplantation (Fig. 44.6). However, these matrices do not actively contribute to the preservation of stem cell properties during expansion and engraftment. To provide a surrogate niche for LESCs throughout ex vivo culture and after transfer to the ocular surface, amniotic membrane (AM) has become a popular substrate. AM is the innermost membrane of the fetal sac, which can be obtained from healthy volunteers during routine caesarean sections. Properties which make AM well suited for ocular surface reconstruction are its avascularity, relative transparency, low immunogenicity, expression of anti-inflammatory and antiangiogenic proteins, as well as growth factors (see Chapter 37
Cultured Limbal Epithelial Stem Cells for Reconstruction of the Corneal Epithelium
Introduction
History and Rationale
Isolation Methods
The Limbal Stem Cell Niche in Culture
Amniotic Membrane as a Culture Substrate
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine