Cost Analyses for the Treatment of Unilateral Childhood Cataracts
David Stager Jr
Joost Felius
Medical decision and policy making are increasingly driven by cost-effectiveness data. Ideally, for decisions on resource allocation, a comprehensive societal perspective is taken that includes all costs and benefits, regardless of who incurs the costs and who reaps the benefits.1 However, calculation of the cost-effectiveness from the societal perspective is complicated and depends on numerous unknown variables. A third-party payer perspective is typically more constrained and thus more straightforward to calculate, and the results are useful for the evaluation of specific procedures or for comparing alternative treatment approaches. As a worked-out example of establishing a cost-utility framework for pediatric cataract care, we present a third-party payer perspective cost assessment for the treatment and care of congenital unilateral cataracts.
EXAMPLE
A spreadsheet (Microsoft® Excel, Redmond, WA) was constructed to calculate the costs associated with a basic scenario as well as selected complications. The basic scenario (Fig. 10.1) consisted of extraction of a congenital unilateral cataract with anterior vitrectomy during the first few months of life, followed by contact lens optical correction until placement of a secondary intraocular lens (IOL) at age 6 years and spectacle correction thereafter. The scenario also included a regimen of alternate-day patching of the fellow eye from the time of cataract removal until age 8 years, as well as follow-up care until age 12 years. Two comprehensive and two intermediate office examinations annually as well as one additional contact lens visit each year were included. Exams under anesthesia were assumed to take place annually during the first 4 years and once in the year of IOL placement. The corresponding direct costs were based on 2011 Current Procedural Terminology (CPT) codes and Medicare payment information2 for procedures and examinations (including anesthesia and facility fees; Table 10.1) and on costs and quantities of medications, optical aids, and patches, thus taking a third-party payer perspective.
In addition to the basic scenario, known sequelae and complications of cataract extraction in infants were included and weighed by published rates of incidence (Table 10.1). Lens reproliferation or secondary membranes were assumed to occur in 20% of cases.3,4 Management requires membrane removal in the operating room and one follow-up examination in the office (in addition to follow-up included in the basic scenario). Clinically significant strabismus was assumed to occur in 70% of cases.5 In an estimated 80% of those cases, management requires one extraocular muscle surgery, whereas in the remaining 20% of the strabismus cases a second extraocular muscle surgery is needed for ocular alignment.
Again, one extra office examination following each surgical procedure was included. Glaucoma was assumed to occur in 15% of cases,6,7,8,9,10,11,12 half of which are treated with drops (estimated one 5-mL bottle of generic timolol per month, at $17 each) while the other half receives a glaucoma implant. We assumed that glaucoma occurs around age 6 years. All patients with glaucoma have a follow-up schedule of six examinations in the year of occurrence and three examinations in the following years. Retinal detachment was assumed to occur in 1% of cases, with management consisting of a scleral buckling procedure. Endophthalmitis after pediatric cataract surgery is rare and was modeled at 0.1% incidence,13,14 with usual treatment consisting of a vitrectomy and antibiotics. The management of retinal detachment and endophthalmitis also included one extra office examination following each surgical procedure.
This example yielded the following cost estimates. The costs associated with the basic scenario ($20,091 per patient) and with the typical complications ($2,485) are
presented in Table 10.2. The total estimated costs in this model (sum of basic scenario and typical complications) are then $12,824 per patient for operating room procedures (including surgical procedures and examination under anesthesia, facility fees, anesthesia), $4,202 for office examinations (comprehensive and intermediate exams, contact lens checkups), $5,287 for optical aids (spectacles, contact lenses) and patches, and $263 for medications (glaucoma drops). These numbers combined yielded $22,576 per patient for a point estimate of the total cost associated with this particular management approach of a congenital unilateral cataract.
presented in Table 10.2. The total estimated costs in this model (sum of basic scenario and typical complications) are then $12,824 per patient for operating room procedures (including surgical procedures and examination under anesthesia, facility fees, anesthesia), $4,202 for office examinations (comprehensive and intermediate exams, contact lens checkups), $5,287 for optical aids (spectacles, contact lenses) and patches, and $263 for medications (glaucoma drops). These numbers combined yielded $22,576 per patient for a point estimate of the total cost associated with this particular management approach of a congenital unilateral cataract.
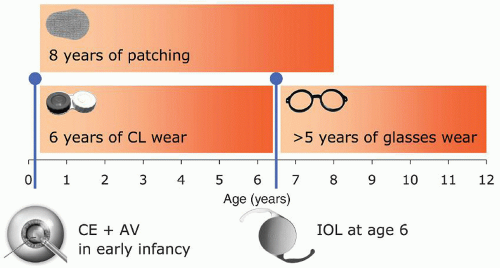 Figure 10.1. Schematic overview of the basic scenario, including lens removal (CE + AV) in the first year of life, placement of a secondary IOL at age 6 years, and follow-up until age 12 years. Bars indicate regimens of optical correction and patching. |
Table 10.1 COST ELEMENTS FOR THE BASIC SCENARIO AND TYPICAL COMPLICATIONS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



