Cosmetic Uses of Neurotoxins and Injectable Fillers
Grant S. Gillman
Nonsurgical techniques for facial rejuvenation have become the fastest growing area of many cosmetic practices. The use of botulinum toxin and injectable fillers, either alone or in combination, has proven over time to be an effective, minimally invasive and extremely popular treatment option for facial rhytids. Improved safety profiles, lower costs, negligible downtime and increasing duration of effect have led to the veritable explosion of interest in the nonsurgical treatments of facial aging.
One should begin by understanding the basic difference between the neuromodulators and injectable fillers. Whereas botulinum toxin injections are used to eliminate or soften specific dynamic facial lines (i.e., wrinkles produced during animation with active contraction of the facial muscles) by selectively weakening the underlying muscles, the fillers as a group are generally used to help efface facial wrinkles or creases that are apparent even at rest. In that sense, botulinum toxin can be thought of as preventing selected facial wrinkles from developing or deepening, while the injectable fillers on the other hand are used for the treatment of already established rhytids. In many cases, the combination of the two might yield a better result than either product alone.
Distinct facial regions are affected by the aging process in different ways. In general, aging of the upper face results more from repetitive action of smaller muscles with the secondary development of dynamic lines—forehead, glabellar and periorbital (crow’s feet). Age-related volume loss (aside from the temporal area) contributes less to the aging of the upper face. Accordingly, the use of neuromodulators such as botulinum toxin plays a greater role in the nonsurgical rejuvenation of the upper face than the dermal fillers. On the other hand, gravitational descent, hollowing and volume loss are the primary determinants of aging changes seen in the midface where the approach to volume restoration and nonsurgical rejuvenation focuses primarily more on the use of fillers than neurotoxins. In the lower face, volume loss in the lips and prejowl sulcus as well as deepening of the nasolabial creases are seen with aging in addition to the development of dynamic perioral lines (vertical upper lip rhytids, marionette lines). In the lower face therefore, selective application of either the fillers or neuromodulators can be useful means of addressing the aging changes seen in this region.
While the risk/benefit ratio for these products is extremely favorable, familiarity with the actions, indications, contraindications, treatment expectations and proper patient selection is vital to maximizing patient satisfaction and minimizing complications. Knowledge of the regional anatomy and proper technique are an equally important part of the foundation upon which successful use of these products is built.
REGIONAL ANATOMY
For the most common cosmetic applications of botulinum toxin, one must be intimately familiar with the relevant muscular anatomy of the forehead, glabella, brow, periorbital and perioral regions, and neck (Fig. 197.1).
Horizontal forehead rhytids are caused by repeated contraction of the frontalis muscle—the sole elevator of the brow. In general, there is a midline separation between the two frontalis muscles, and the vertical contraction of those muscles elevates the brow and scalp leading to the formation of transverse lines in the forehead. The frontalis muscle originates from the galea aponeurotica superiorly and interdigitates with the brow depressors inferiorly. From a clinical perspective, it is important to recognize that isolated treatment of the frontalis muscle—the only brow elevator—leaves the action of the brow depressor muscles unopposed. In some patients, this can result in brow ptosis or a heavy, visor-like feeling to the brow.
Brow elevation by the frontalis muscles is opposed by muscles that function as the brow depressors. These
include the procerus, the corrugator supercilii, the orbicularis oculi and the depressor supercilii (the fibers of the orbicularis below the medial brow).
include the procerus, the corrugator supercilii, the orbicularis oculi and the depressor supercilii (the fibers of the orbicularis below the medial brow).
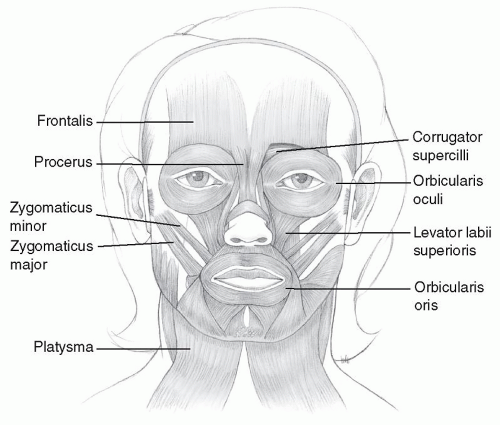 Figure 197.1 Facial musculature. |
The procerus muscle originates inferiorly from the lower nasal bones in the midline and runs vertically to blend with the frontalis and insert in the soft tissue between the brows. Contraction of the procerus creates the visible transverse crease at the root of the nose.
The paired corrugator supercilii muscles originate deep to the frontalis and orbicularis muscles near the medial supraorbital ridge where the frontal and nasal bones meet and run superolaterally to insert into the skin and subcutaneous tissue just above the mid-brow. Contraction of the corrugator muscles causes the vertical glabellar lines between the brows (the “frown” lines).
The orbicularis oculi muscle consists of two parts—the orbicular (the outermost portion) and the palpebral, with the latter being divided into preseptal and pretarsal portions. The muscle broadly encircles the orbit, interdigitating with the corrugator muscle medially and superiorly and the frontalis muscle superiorly. Contraction of the orbital portion of the muscle is what produces the lateral orbital rhytids or “crow’s feet.” Some of the medial fibers of the orbicularis oculi known as the depressor supercilii insert into the skin below the medial eyebrow and also act as medial brow depressors.
The orbicularis oris muscle encircles the mouth and functions both as an oral sphincter and to protrude the lips. Its fibers merge with the depressor anguli oris and the risorius muscles lateral to the oral commissure and the zygomaticus major and minor superiorly. Contraction of the orbicularis oris will result in the fine vertical rhytids that radiate around the upper and lower lips.
The platysma muscle is responsible for horizontal neck creases and vertical bands in the neck. It originates from the fascia overlying the upper chest and clavicle and extends superiorly to insert on the lower mandible and mentum medially and blends with the perioral muscles centrally. More posteriorly and superiorly, the platysma is continuous with the SMAS in the lower two-thirds of the face.
BOTULINUM TOXIN (NEUROTOXINS)
Botulinum toxin injections have become by far the most frequently performed cosmetic procedure over the last decade. In 2008, the use of neurotoxins accounted for almost 25% of all nonsurgical aesthetic procedures (1). Cosmetic applications have expanded, and an increasing number of nonaesthetic applications have been reported as well.
A number of commercially available neuromodulators have been FDA approved for cosmetic applications in the United States. Two of these are formulations of botulinum toxin type A (BoNTA)—onabotulinum toxin A (BoNTAONA), which is sold as Botox Cosmetic (Allergan, Inc., Irvine, CA), and abobotulinum toxin A (BoNTA-ABO), which is sold under the trade name Dysport (Medicis Aesthetics, Scottsdale, AZ). Both of these have been approved for the treatment of glabellar lines in addition to their nonaesthetic indications. A third neurotoxin, a formulation of botulinum toxin B, marketed as Myobloc (Solstice Neurosciences, South San Francisco, CA), is FDA approved for nonaesthetic (medical) use and will not be discussed at any length in this chapter. Beyond their FDA-approved medial and aesthetic indications, each of these has been used technically “off-label” in the cosmetic treatment of non-glabellar hyperkinetic facial lines as well.
In addition to differences in the formulation itself, commercial preparations may differ with respect to pH, protein content, purification and manufacturing methods as well as other characteristics (2). It is likely that these differences
account somewhat for the variations in clinical characteristics and performance. As a result, there is no single conversion factor that yields exact equivalents of efficacy, safety and diffusion between the various preparations, and BoNTA-ABO units are not interchangeable with BoNTA-ONA units (the two main botulinum toxin preparations used clinically). In general, however, BoNTA-ABO (Dysport) is less active on a per unit basis than BoNTA-ONA (Botox Cosmetic), which means that more units are required to achieve a comparable effect. That said, the literature with respect to dose conversions can be confusing, variable in rigor and validity and not free of commercial bias. More recently published literature suggests that one unit of BoNTA-ONA (Botox Cosmetic) is roughly equivalent to 2 to 4 units of BoNTA-ABO (Dysport) for a ratio of 2:1 to 4:1 (3).
account somewhat for the variations in clinical characteristics and performance. As a result, there is no single conversion factor that yields exact equivalents of efficacy, safety and diffusion between the various preparations, and BoNTA-ABO units are not interchangeable with BoNTA-ONA units (the two main botulinum toxin preparations used clinically). In general, however, BoNTA-ABO (Dysport) is less active on a per unit basis than BoNTA-ONA (Botox Cosmetic), which means that more units are required to achieve a comparable effect. That said, the literature with respect to dose conversions can be confusing, variable in rigor and validity and not free of commercial bias. More recently published literature suggests that one unit of BoNTA-ONA (Botox Cosmetic) is roughly equivalent to 2 to 4 units of BoNTA-ABO (Dysport) for a ratio of 2:1 to 4:1 (3).
Mechanism of Action
Clostridium botulinum is a gram-positive anaerobic bacteria that produces eight antigenically distinct toxins (A, B, C1, C2, D, E, F, and G), seven of which are neuroparalytics. The neurotoxin produces a temporary chemical denervation by inhibiting the release of acetylcholine from the presynaptic neuron at the motor end plates of voluntary muscle. All seven serotypes share the same mechanism of action, inhibiting acetylcholine release at peripheral nerve endings, but differ with respect to molecular complex size, presence or absence of complexing proteins and specific details in their sequence of action (4).
The flaccid paralysis that follows is temporary in nature. Chemodenervation is followed by a two-stage recovery process. Initially, there is growth and sprouting of new axonal collaterals which establish new connections at the motor end plate. At about 3 months, neural transmission through the original (primary) nerve terminal is reestablished and the collateral axons regress (5). This correlates with clinical recovery of function typically in the range of 3 to 4 months postinjection.
Indications and Contraindications
Botox Cosmetic is currently FDA approved for therapeutic use in cervical dystonia, strabismus, blepharospasm and hyperhidrosis and cosmetically for the temporary improvement in vertical glabellar rhytids caused by the action of the corrugator and procerus muscles. Dysport is FDA approved for therapeutic use in the treatment of cervical dystonia in adults and cosmetically for the temporary improvement in glabellar lines. Although technically “off-label,” the clinical use of these BoNTA preparations has expanded widely to include the treatment of many other conditions including other facial hyperkinetic lines, migraine headaches, hyperhidrosis, bruxism, Frey syndrome, muscle tension dysphonia, torticollis and bilateral masseteric hypertrophy to name a few.
The use of any botulinum toxin is contraindicated in individuals with preexisting neuromuscular disorders (e.g., myasthenia gravis, amyotrophic lateral sclerosis, Eaton-Lambert syndrome) and patients with a sensitivity to any other botulinum toxin product, an albumin allergy, or cow’s milk protein allergy (in the case of Dysport; as distinct from patients who are lactose intolerant). Use in pregnant women or lactating mothers is not recommended as there is no safety data regarding use in such circumstances.
Cosmetic Applications of Botulinum Toxin
Commercially available Botox Cosmetic is supplied in a crystalline form as 100 unit vials, whereas Dysport is supplied with 300 units per vial. Both products are diluted with sterile, preservative free normal saline. The volume of dilution depends on the preference of the treating physician. Most prefer dilutions that yield concentrations of 2 to 5 units of Botox Cosmetic per 0.1 mL as this product is typically injected in 2 to 5 unit aliquots (per injection site). Dysport is generally diluted to yield concentrations of either 10 units per 0.1 mL or 10 units per 0.05 mL as this product is typically injected in 10-unit aliquots (per injection site).
The volume of dilution (and hence the concentration) can vary with the clinician’s preference, but the underlying principle is that high concentration-low volume injections will help minimize unwanted dispersion of the toxin to surrounding tissues. According to the product information, it is recommended that once reconstituted botulinum toxin should be used within 4 hours, although many clinicians have refrigerated any unused toxin for use up to 30 days (6) and found it to still be clinically effective. In one study of timing of onset and duration of effect in the treatment of forehead rhytids, no difference was found between freshly reconstituted Botox Cosmetic as compared to the same product which was either reconstituted and stored in a refrigerator for 2 weeks or reconstituted and stored in a freezer for 2 weeks prior to use (7).
Following injection, the onset of muscle weakness with BoNTA generally occurs between 2 and 5 days. Botulinum toxin type B (Myobloc) has been shown to have a faster rate of onset than BoNTA formulations—often within 24 hours (8). In general, the duration of response to the BoNTA preparations is similar to one another and should last on average 3 to 4 months before full muscle recovery is noted, though comparative studies looking at physician and patient evaluations of improvement and satisfaction suggest that Botox Cosmetic may have a longer duration of effect than Dysport (9,10). Myobloc on the other hand has a shorter duration of action than either formulation of BoNTA, with efficacy lasting only up to 8 weeks (8).
Although there are many potential applications for the use of botulinum toxin, this chapter will review in general terms only the most common uses for improving facial aesthetics— the treatment of glabellar rhytids (“frown lines”), transverse forehead rhytids, lateral periorbital rhytids (“crow’s feet”), the adjustment of brow contour and position (the “ chemical”
browlift), the treatment of platysmal banding in the neck and vertical upper lip rhytids.
browlift), the treatment of platysmal banding in the neck and vertical upper lip rhytids.
Differences in either injection site specifics or individual adjustments in dose will be apparent from patient to patient and may result from variations in muscle bulk, animation pattern, severity of rhytids, previous results and unique anatomic variations. Keeping detailed treatment records with respect to site, dosage and differences will facilitate reproducibility and improve patient satisfaction. Injection technique is essentially the same regardless of which formulation is used.
Glabellar Rhytids
Glabellar rhytids include the vertical “frown” lines produced by contraction of the corrugator supercilii muscles as well as the transverse crease at the nasion produced by contraction of the procerus. Injection points for glabellar rhytids should target the procerus in the region of the nasion at the intersection of two lines, each of which extends from the medial brow to the opposite medial canthus. Each corrugator muscle is injected medially and laterally into the belly of the muscle above the medial brow roughly in line with the medial canthus and further laterally along the muscle, staying medial to the mid-pupillary line (Fig. 197.2). The latter two injections should always be at or above a transverse line drawn though the mid-eyebrow and above the superior orbital rim to minimize the chance of diffusion into the levator palpebrae of the upper lid which could result in a transient eyelid ptosis (11).
Transverse Forehead Rhytids
As the frontalis muscle is the only elevator of the brow, isolated treatment of horizontal forehead lines must be done with caution. In the patient with heavy glabellar rhytids or a very low brow one should assume that the brow depressors are quite strong and active, in which case isolated treatment of the frontalis muscle may cause or further aggravate brow ptosis. In such cases, concomitant treatment of the brow depressors (corrugators, procerus) should at the very least be discussed with the patient.
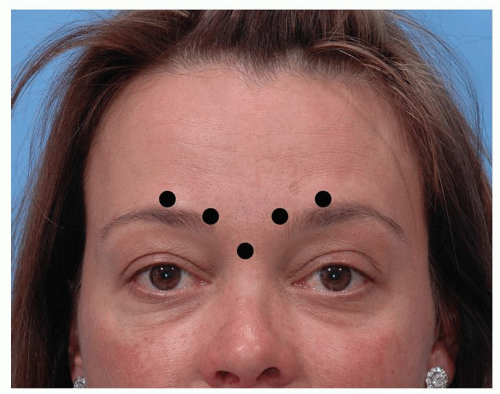 Figure 197.2 Typical botulinum toxin injection pattern for glabellar rhytids/corrugator creases. |
 Figure 197.3 Typical grid-like botulinum toxin injection pattern for transverse forehead rhytids. |
Effective treatment of the transverse forehead rhytids involves subcutaneous or intramuscular injections into the frontalis muscle, either in a relatively uniform grid-like fashion across the forehead (Fig. 197.3) or at four to five equally spaced sites on a horizontal line between the eyebrows and the hairline. Care is taken to stay a minimum of 1 to 1.5 cm above the brow for all injections to minimize the risk of eyebrow ptosis. Simultaneous treatment of brow depressors, if undertaken, can involve the procerus and/or corrugators and/or the lateral orbicularis oculi above the orbital rim and just below the tail of the brow.
Lateral Periorbital Rhytids
Lateral periorbital rhytids (“crow’s feet”) result from repeated contraction of the lateral portion of the orbicularis oculi muscles. As this muscle is very thin and superficial, intradermal or immediately subdermal injections are sufficiently deep and will help minimize the bruising that can occur commonly in this area. Injections should also be on an arc at least 1.5 cm lateral to the lateral canthus and 1 cm outside the lateral orbital rim to minimize the chance of any diffusion through the lid into the levator palpebrae superioris which could result in upper eyelid ptosis. Treatment of the crow’s feet is best avoided in anyone with a preexisting upper eyelid ptosis, lagophthalmos or upper facial palsy.
Having the patient smile or squint will help identify the specific area or lines in need of treatment. Multiple serial injections are then used, typically two to four, perpendicular to the muscle and just outside the orbital
rim (Fig. 197.4). The amount injected per site will depend on the distribution of the lines and the activity of the underlying orbicularis oculi.
rim (Fig. 197.4). The amount injected per site will depend on the distribution of the lines and the activity of the underlying orbicularis oculi.
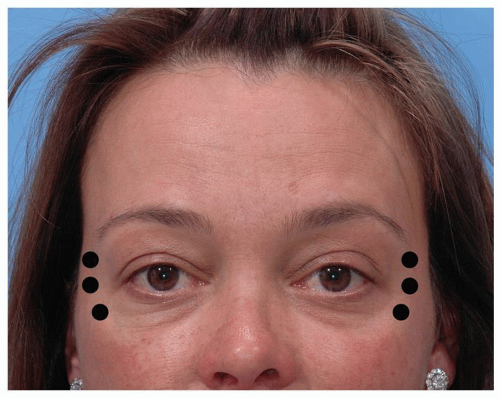 Figure 197.4 Typical botulinum toxin injection pattern for lateral periorbital rhytids. |
Adjustment of Brow Position and Contour (The “Chemical Browlift”)
At least to some degree, brow position is the result of an equilibrium reached between the action of the brow elevator (the frontalis) and the opposing action of the brow depressors (the corrugator, the procerus, the orbicularis oculi and the depressor supercilii) (12,13). As such, selective weakening of the brow depressors with botulinum toxin, either medially or laterally, may result in a modest (several mm) “pharmacologic” brow lift.
Elevation of the entire brow will require attention to both the medial and the lateral brow depressors. Frequently, elevation of only one end of the brow or the other might be desired in which case it suffices to address those muscles only. For elevation of the medial brow, treatment of the corrugators and procerus as well as the depressor supercilii is required. The latter muscle is treated with an injection of a small dose just below and just lateral to the medial head of the brow, taking care to remain outside the orbital rim to avoid unwanted diffusion into adjacent muscles. Elevation of the lateral brow requires a subdermal injection of the orbicularis oculi muscle just below the eyebrow lateral to the high point of the brow, once again remaining outside the orbital rim. One to three injection sites may be required.
Platysmal Banding
Administration of botulinum toxin to platysmal bands can be a useful adjunct in the treatment of the senescent neck (14). Best results are seen with mild to moderate banding (15), and the changes are most appreciable with dynamic contraction of the platysma than at rest.
Having the patient contract the muscle will best demonstrate the platysmal bands, which are then grasped and injected with botulinum toxin at multiple sites each 1 to 1.5 cm apart, from below the jawline to the lower neck. Typically, each band will receive a total of about 15 units of Botox Cosmetic or 40 to 80 units of Dysport per band. Caution must be exercised to avoid excessive doses and to inject into the muscle but not deep to it. Overly deep injections can increase the risk of dysphagia and/or neck weakness.
Vertical Lip Rhytids
Very low doses of botulinum toxin injected into the orbicularis oris muscle of the upper lip can help efface or soften vertical upper lip lines. This treatment may be an alternative to perioral chemical peels or laser resurfacing and can be used alone or in combination with injectable fillers. In order to avoid problems with oral incompetence the injections are kept very superficial (subdermal), and very small doses are used initially. Nonetheless, professional public speakers and wind instrument musicians may not be ideal candidates for this treatment.
Four evenly spaced injections are given across the upper lip at or immediately above the vermilion border. Starting with lower doses and increasing if necessary is most prudent. In addition to reducing the depth of apparent vertical lip lines, some degree of lip eversion is also frequently noted.
Botulinum Toxin Complications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


