Purpose
To evaluate topographic and tomographic changes in fellow eyes in unilateral keratoconus (KCN) patients by comparing them with normal eyes.
Design
Retrospective comparative case series.
Methods
Fourteen eyes of 14 patients with unilateral KCN and 34 eyes of 34 refractive surgery candidates were divided into 3 diagnostic groups using a Pentacam rotating Scheimpflug camera: advanced KCN eyes of unilateral KCN (KCN group, 14 eyes), normal fellow eyes of unilateral KCN (fellow eye group, 14 eyes), and refractive surgery candidates (normal group, 34 eyes). Topographic and tomographic parameters, which were obtained from Pentacam using sagittal curvature, elevation, and corneal thickness maps, were compared among the 3 groups. Receiver operating characteristic (ROC) curves were used to identify cutoff points in discriminating between fellow and normal eyes.
Results
Keratometric asymmetry, topometric indices, and elevation differences (maximum − minimum) on both the anterior and posterior surfaces were statistically different ( P < .05). On ROC curve analysis, keratometric asymmetry and topometric index were best at discriminating fellow eyes from normal, followed by elevation differences (maximum − minimum) on the posterior and anterior cornea surface.
Conclusions
Fellow eyes in unilateral KCN showed differences in several parameters that were not detectable with the Pentacam detection program, when compared with normal. However, each single parameter alone is not sufficient to detect early changes; thus, elevation indices as well as indices of anterior curvature should be considered together.
Corneal ectasia is one of the most serious complications of refractive surgery. Risk factors identified for post–laser in situ keratomileusis (LASIK) ectasia include high myopia, low residual stromal bed thickness, and defined topographic abnormalities such as keratoconus (KCN) and pellucid marginal corneal degeneration. Although the majority of these risk factors are identifiable preoperatively, missed preoperative topographic abnormalities are a major independent risk factor. As a result, detection of early KCN in the preclinical stage is very important for preventing post-LASIK ectasia. Advanced KCN can be diagnosed with typical biomicroscopic, retinoscopic, and topographic findings. However, detection of the disease in the preclinical stage is difficult.
Several terms have been employed to describe the preclinical stages of the KCN condition, including subclinical keratoconus, keratoconus suspect (KCS), and forme fruste keratoconus (FFKC). The term KCS was reserved for the cornea with some anterior topographic changes of KCN but without evidence of clinical KCN in either eye. The term FFKC was first described by Amsler as an incomplete, abortive, or unusual form of a syndrome of disease, meaning corneas that have subtle topographic characteristics that do not reach the threshold of keratoconus suspect. However, because of the ambiguity of definition and significant overlap between these designations, there are no definitive criteria to help discriminate subclinical KCN from normal.
Placido disk–based topography had been the most sensitive method to detect KCN, and several indices and artificial intelligence methods have been developed to help diagnose subclinical KCN. With recent advances in Orbscan slit-scanning topography (Bausch & Lomb, Rochester, New York, USA) and the Pentacam rotating Scheimpflug camera (Oculus, Wetzlar, Germany), anterior and posterior corneal elevation and pachymetric maps provide useful data to discriminate subclinical KCN from normal. Recent studies have found that pachymetric progression and elevation data can help to identify subclinical KCN not detected by Placido disk–based topography. Ambrosio and associates proposed new tomographic-derived pachymetric parameters, such as relation thickness, which were better able to differentiate normal and keratoconic corneas. This suggests that several tomographic data from elevation and pachymetric values could be more sensitive to detect subclinical KCN before changes of anterior curvature in Placido disk–based topography. Several studies described topographic and tomographic differences between subclinical KCN and normal controls, which were not detectable using Placido disk–based topography. But there has not been any report about the subclinical KCN with normal elevation and pachymetric-derived parameters.
The purpose of this study was to investigate the characteristics of the subtle changes in subclinical KCN and compare it with normal. Previous research indicates that true unilateral KCN is very rare, and that the normal fellow eye is also thought to have subclinical KCN. Thus, the normal fellow eye in unilateral KCN may be the ideal model for the mildest form of subclinical KCN. In the present study, normal fellow eyes in unilateral KCN patients were considered as the mildest form of subclinical KCN and topographic and tomographic parameters were analyzed using Pentacam.
Subjects and Methods
Subjects
This study included patients with unilateral KCN diagnosed by Pentacam and candidates for refractive surgery with normal corneas. Clinical records of 48 patients (62 eyes) seen at the Samsung Medical Center between January 2009 and March 2011 were retrospectively analyzed. The study protocol was reviewed and approved by the Sungkyunkwan University Institutional Review Board, and a waiver of informed consent was granted because of the low risk of this research. The tenets of the Declaration of Helsinki were followed for all study procedures.
The study subjects were divided into 3 groups: advanced KCN eyes of unilateral KCN patients (KCN group, 14 eyes), normal fellow eyes of unilateral KCN patients (fellow eye group, 14 eyes), and refractive surgery candidates (normal group, 34 eyes). Eyes were diagnosed as KCN on the basis of Pentacam rotating Scheimpflug camera–derived topographic/tomographic parameters and criteria used in the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) study. Patients who had advanced KCN in 1 eye and a normal fellow eye were considered unilateral KCN. In this study, fellow eyes in unilateral KCN should not only be clinically normal but also satisfy all of the following criteria determined by the Pentacam: normal index of topographic keratoconus classification (use of keratometric values on the anterior corneal surface to detect ectatic changes) and final D value <1.6 SD from the Belin/Ambrósio Enhanced Ectasia Display II. Normal control patients were candidates for refractive surgery with clinically normal corneas and topographic/tomographic values that were within normal limits determined by the Pentacam. All normal control patients underwent uncomplicated refractive surgery (femto-LASIK or laser-assisted subepithelial keratectomy) and had a 2-year follow-up without any evidence of ectatic corneal changes. In the normal group, only left eyes were used in the study analysis.
None of the patients had a history of previous ocular surgery or trauma, and they were asked to stop wearing contact lenses for at least 3 weeks for rigid contact lenses and 1 week for soft contact lenses prior to examination. KCN subjects with corneal scarring significant enough to disturb Pentacam evaluation were excluded from this study.
Procedure
All subjects underwent a clinical, topographic, and tomographic evaluation. Clinical examinations included slit-lamp biomicroscopy, retinoscopy, and fundus examination. Topographic and tomographic examinations were performed using the Pentacam rotating Scheimpflug camera (Oculus, Wetzlar, Germany). The sagittal curvature, anterior elevation, posterior elevation, corneal thickness, and Belin/Ambrósio Enhanced Ectasia Display II were evaluated. Elevation data were taken from a fixed 8.0-mm zone (best fit sphere [BFS] set to Manual, Float, Sphere, Diameter = 8.0 mm) centered on the corneal apex.
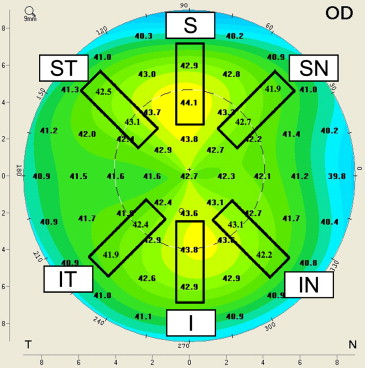
The following data were analyzed in Pentacam: (1) keratometric values: flat keratometry (K1), steep keratometry (K2), and mean keratometry (Km) for the central 3.0 mm of the cornea; (2) keratometric asymmetry: inferior-superior asymmetry at 4 and 6 mm (4 mm I-S and 6 mm I-S), superotemporal-inferonasal asymmetry at 4 and 6 mm (4 mm ST-IN and 6 mm ST-IN), and superonasal-inferotemporal asymmetry at 4 and 6 mm (4 mm SN-IT and 6 mm SN-IT) radius ring of the cornea ( Figure ); (3) topometric indices in an 8-mm zone, which were derived via Placido disk–based data: index of surface variance, index of vertical asymmetry, keratoconus-index, center keratoconus-index, index of height asymmetry, index of height decentration, and radii minimum; (4) elevation values: diameter of BFS, elevations (maximum and minimum), elevation differences (maximum − minimum) on anterior and posterior cornea in the central 2.0-mm zone; (5) corneal thickness: corneal thickness at the apex and at the thinnest point; (6) Belin/Ambrósio Enhanced Ectasia Display II: D values representing the front surface (Df), back surface (Db), pachymetric progression (Dp), thinnest point (Dt), thinnest point displacement (Dy), and final (D), pachymetric progression indices: pachymetric progression indices (maximum, minimum, and average); (7) Ambrósio’s relational thickness values calculated by the following formula: Ambrósio’s relational thickness maximum = thinnest pachymetry/pachymetric progression index maximum and Ambrósio’s relational thickness average = thinnest pachymetry/pachymetric progression index average.
Statistical Analysis
The normality of all data samples was first checked using the Shapiro-Wilk test. When parametric analysis was possible, paired t tests for paired data or Student t tests for unpaired data with Bonferroni correction were used to compare groups (KCN, fellow eye, and normal). When parametric analysis was not possible, Wilcoxon signed rank tests for paired data and Mann-Whitney U tests for unpaired data were used. Null hypotheses of no difference were rejected if P values were less than .05, and statistical calculations used PASW (PASW, version 17.0 for Windows; SPSS, Chicago, Illinois, USA). The receiver operating characteristic (ROC) curve was analyzed for parameters that were different between cases of fellow eye and normal groups. Cutoff values were determined as the maximized sum of sensitivity and specificity. Internal validation was evaluated by the bootstrap method. A single dataset with the same sample size as the original dataset was generated with replacement by using the Proc Survey select procedure from SAS software, version 9.1.3 (SAS Institute Inc, Cary, North Carolina, USA), and the cutoff values of the corneal parameters were determined given the results from this dataset. This procedure was repeated 1000 times, and 95% confidence intervals were developed from these cutoff values using the 2.5th and the 97.5th percentiles. Statistical analyses were performed using SAS software, version 9.1.3 (SAS Institute Inc).
Results
Fourteen eyes of 14 unilateral KCN patients and 34 eyes of 34 normal refractive surgery candidates were analyzed. The ratio of male to female patients was 13:1 in the unilateral KCN group and 13:21 in the normal group, respectively. There were significantly more men in the unilateral KCN than in the normal ( P < .001). The mean age was 25.08 ± 6.39 (range: 18–43) years in the unilateral KCN and 28.00 ± 5.93 (range: 19–41) years in the normal, which was not statistically different.
KCN vs Fellow Eye
There were significant differences between the KCN and fellow eye in all measured parameters ( Table 1 ).
| KCN (14 Eyes) | Fellow Eye (14 Eyes) | Normal (34 Eyes) | KCN vs Fellow Eye | KCN vs Normal | Normal vs Fellow Eye | |
|---|---|---|---|---|---|---|
| Mean ± SD | P Value | |||||
| Keratometry of anterior surface | ||||||
| K1 (D) | 45.26 ± 4.22 | 42.20 ± 1.08 | 42.57 ± 1.65 | .020 a | .036 b | .365 b |
| K2 (D) | 50.47 ± 8.45 | 43.40 ± 1.36 | 43.90 ± 1.49 | .001 c | <.001 d | .268 b |
| Km (D) | 47.53 ± 5.01 | 42.79 ± 1.20 | 43.21 ± 1.52 | .003 a | .007 b | .318 b |
| 4 mm I-S (D) | 12.05 ± 5.28 | 1.68 ± 1.20 | 0.65 ± 0.55 | <.001 a | <.001 d | .002 d |
| 4 mm ST-IN(D) | 6.41 ± 4.53 | 1.09 ± 0.64 | 0.50 ± 0.41 | .002 c | <.001 d | .002 d |
| 4 mm SN-IT(D) | 11.08 ± 4.91 | 0.86 ± 0.61 | 0.58 ± 0.53 | <.001 a | <.001 d | .182 d |
| 6 mm I-S(D) | 8.93 ± 4.26 | 1.42 ± 1.20 | 0.78 ± 0.59 | .002 c | <.001 d | .908 d |
| 6 mm ST-IN(D) | 4.55 ± 4.35 | 0.79 ± 0.72 | 0.55 ± 0.36 | .009 c | <.001 d | 1.0 d |
| 6 mm SN-IT(D) | 8.30 ± 3.34 | 0.92 ± 0.67 | 0.74 ± 0.45 | <.001 a | <.001 b | 1.0 b |
| Topometric index | ||||||
| Index of surface variance | 103.29 ± 44.85 | 20.07 ± 7.11 | 17.88 ± 4.48 | <.001 a | <.001 d | .539 d |
| Index of vertical asymmetry | 1.12 ± 0.42 | 0.18 ± 0.08 | 0.12 ± 0.04 | <.001 c | <.001 d | .023 b |
| Keratoconus index | 1.23 ± 0.13 | 1.03 ± 0.03 | 1.02 ± 0.02 | <.001 a | <.001 b | .092 d |
| Central keratoconus index | 1.11 ± 0.18 | 1.00 ± 0.01 | 1.01 ± 0.01 | .005 c | .003 d | .251 d |
| Index of height asymmetry | 37.47 ± 24.84 | 5.72 ± 4.27 | 3.48 ± 3.39 | <.001 a | <.001 d | .066 d |
| Index of height decentration | 0.09 ± 0.04 | 0.01 ± 0.00 | 0.01 ± 0.00 | <.001 a | <.001 d | .007 d |
| Radii minimum | 5.95 ± 1.02 | 7.56 ± 0.33 | 7.59 ± 0.28 | <.001 a | <.001 b | .807 b |
| Anterior elevation | ||||||
| BFS (mm) | 7.69 ± 0.37 | 7.91 ± 0.41 | 7.90 ± 0.28 | .013 c | .067 b | .468 d |
| Elevation Max (μm) | 32.86 ± 14.69 | 5.07 ± 2.95 | 3.32 ± 1.15 | <.001 a | <.001 d | .195 d |
| Elevation Min (μm) | −8.21 ± 10.57 | −1.36 ± 2.17 | −0.56 ± 1.28 | .035 c | <.001 d | .156 d |
| Elevation difference (Max − Min) (μm) | 41.07 ± 16.85 | 6.43 ± 3.84 | 3.88 ± 1.55 | <.001 a | <.001 b | .031 d |
| Posterior elevation | ||||||
| BFS (mm) | 6.29 ± 0.29 | 6.51 ± 0.25 | 6.40 ± 0.26 | .003 a | .198 b | .185 b |
| Elevation Max (μm) | 56.14 ± 28.70 | 8.71 ± 4.76 | 5.77 ± 2.49 | <.001 a | <.001 d | .161 d |
| Elevation Min (μm) | −13.71 ± 17.40 | -2.93 ± 3.63 | −1.21 ± 2.38 | .039 c | .010 d | .357 b |
| Elevation difference (Max − Min) (μm) | 69.86 ± 37.18 | 11.64 ± 5.89 | 6.97 ± 3.35 | <.001 c | <.001 b | .033 d |
| Corneal thickness | ||||||
| Apex (μm) | 511.14 ± 50.15 | 535.29 ± 26.37 | 549.06 ± 30.24 | .017 c | .017 b | .127 b |
| Thinnest (μm) | 478.93 ± 58.37 | 533.07 ± 25.58 | 546.35 ± 30.06 | .001 c | .001 b | .132 b |
| Pachymetric progression index | ||||||
| Max | 2.99 ± 1.57 | 1.21 ± 0.16 | 1.23 ± 0.17 | .005 c | <.001 d | 1.0 b |
| Min | 1.66 ± 0.89 | 0.74 ± 0.09 | 0.76 ± 0.12 | .007 c | <.001 d | 1.0 d |
| Ave | 2.10 ± 0.95 | 1.00 ± 0.12 | 1.02 ± 0.12 | .005 c | <.001 d | 1.0 d |
| D value | ||||||
| Df | 12.30 ± 6.87 | 0.54 ± 0.64 | 0.19 ± 0.88 | .001 a | <.001 b | .787 b |
| Db | 9.54 ± 7.56 | 0.03 ± 0.80 | −0.15 ± 0.87 | .004 a | .004 b | 1.0 b |
| Dp | 8.07 ± 6.37 | 0.65 ± 0.83 | 0.76 ± 0.70 | .001 c | <.001 d | 1.0 b |
| Dt | 1.60 ± 1.47 | 0.15 ± 0.71 | −0.19 ± 0.81 | .002 a | .005 b | .950 b |
| Dy | 1.39 ± 1.00 | 0.37 ± 0.82 | 0.74 ± 0.85 | .010 a | .322 b | 1.0 b |
| Final D | 9.65 ± 5.74 | 1.03 ± 0.57 | 1.04 ± 0.54 | .001 a | <.001 d | 1.0 d |
| Ambrósio’s relational thickness | ||||||
| Max | 204.15 ± 90.82 | 450.46 ± 76.57 | 452.97 ± 69.49 | <.001 a | <.001 b | 1.0 d |
| Ave | 281.13 ± 121.30 | 540.87 ± 75.12 | 541.98 ± 67.67 | <.001 a | <.001 b | 1.0 b |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


