Purpose
To describe the effect of Descemet stripping automated endothelial keratoplasty (DSAEK) on intraocular pressure (IOP) and corneal graft survival in eyes with pre-existing glaucoma or ocular hypertension.
Design
Retrospective, observational case series.
Methods
We performed a retrospective review of 184 eyes that underwent DSAEK from January 2007 through May 2009 at the Singapore National Eye Centre. Eyes with pre-existing glaucoma or ocular hypertension that underwent DSAEK were included, whereas those with a follow-up period of less than 12 months were excluded. Main outcome measures were graft failure and need for additional IOP-lowering treatment after DSAEK.
Results
Forty-seven eyes (51% male; mean age, 66.6 years) with glaucoma underwent DSAEK and were followed-up for a mean of 27.3 ± 8.5 months. Before DSAEK, 60% were taking at least 1 topical IOP-lowering medication, whereas 14 eyes (30%) previously had undergone glaucoma filtration surgery. After DSAEK, visual acuity improved by a mean of 5.4 ± 3.7 Snellen lines. Seventeen percent of grafts failed at a mean of 12.8 ± 7.0 months. The mean IOP increased by 2.1 mm Hg to 16.0 ± 2.5 mm Hg, with 62% requiring additional IOP-lowering treatment and 28% needing filtration surgery at a mean of 9.3 months after DSAEK. Eyes without prior filtration surgery and eyes that underwent additional intraoperative procedures during DSAEK were 10 and 18 times more likely to require IOP-lowering treatment after DSAEK ( P = .002 and P = .008), respectively.
Conclusions
With prompt and appropriate intervention, IOP in glaucomatous eyes undergoing DSAEK can be controlled with minimal increase after DSAEK. Eyes with previous filtration surgery require fewer medications to control elevated IOP than eyes that have not had previous surgery.
Descemet stripping automated endothelial keratoplasty (DSAEK) is an emerging lamellar corneal transplantation procedure in which donor posterior lamellar tissue is used to replace diseased corneal recipient endothelium and Descemet membrane. DSAEK has been well recognized for its tectonic safety and favorable topographic and refractive outcomes, causing a shift from penetrating keratoplasty toward DSAEK as the primary procedure of choice for the management of endothelial dysfunction.
The development of de novo glaucoma or worsening of pre-existing glaucoma after penetrating keratoplasty ranges between 10% and 53% and is a well-recognized risk factor for graft failure and poor visual outcomes. However, reports on the effect of DSAEK on intraocular pressure (IOP) control in eyes with pre-existing glaucoma and subsequent graft failure have been limited. A recent study by Vajaranant and associates quoted the incidence of IOP elevation after DSAEK to be 45% in eyes of white persons with prior glaucoma and concluded that pre-existing glaucoma did not have a negative effect on visual acuity after DSAEK. Phillips and associates found DSAEK in eyes of white persons with previous trabeculectomies and glaucoma drainage devices to be performed without primary graft failure and with low graft dislocation and graft decentration rates, with excellent early postoperative outcomes. Similarly, various small case series involving eyes of white persons have reported DSAEK in eyes with prior glaucoma filtering surgery or tube shunts to be safe, suggesting that DSAEK be a viable and effective option in eyes with existing glaucoma and corneal endothelial dysfunction. More recently, Letko and associates reported that graft failure rates are higher in eyes with prior glaucoma filtering surgery or tube shunts. The aim of this study was to describe the effect of DSAEK on IOP control and corneal graft survival in Asian eyes with pre-existing glaucoma or ocular hypertension.
Methods
Consecutive eyes with pre-existing glaucoma or ocular hypertension that underwent DSAEK were identified from the Singapore National Eye Centre DSAEK database. Case records were reviewed retrospectively, and the following information was extracted: demographics (age at time of DSAEK, gender, and race), duration of follow-up after DSAEK, indications for DSAEK, pre-existing glaucoma diagnoses, interval between glaucoma diagnosis and DSAEK, visual acuity before DSAEK, IOP before DSAEK, glaucoma interventions and treatment before DSAEK, additional intraoperative procedures at the time of DSAEK, visual acuity after DSAEK (at last follow-up visit), DSAEK graft failures, IOP indices after DSAEK (mean IOP after DSAEK, change in mean IOP before and after DSAEK and IOP range after DSAEK), and IOP-lowering treatment after DSAEK. IOP measurements were not corrected for corneal thickness. Eyes with a follow-up period of less than 12 months were excluded.
Five consultant corneal surgeons (D.T., J.M., 3 independent surgeons) performed the DSAEK procedures, as described elsewhere in detail. In brief, donor graft lamellar dissection was achieved using an automated lamellar therapeutic keratoplasty microkeratome (Moria USA, Doylestown, Pennsylvania, USA). The residual posterior lamellar thickness was measured with ultrasound pachymetry, and trephination was performed using a standard Hanna punch trephine system with standard trephine sizes between 7.75 and 9 mm at 0.25-mm increments. A 5-mm scleral tunnel incision was made in all cases. Stripping of Descemet membrane and endothelium was performed with a reverse Sinskey hook under air followed by insertion of the donor graft by the taco-folded insertion technique or the Sheets glide-insertion technique. An inferior surgical iridectomy was performed. To enhance donor graft adhesion, a tamponading air bubble was injected into the anterior chamber and drainage of interface fluid was achieved through 4 paracentral vents. The air bubble was partially evacuated before the end of the procedure to leave an air bubble approximating the size of the graft.
The postoperative steroid regimen consisted of topical prednisolone acetate 1% every 3 hours for the first 7 days, gradually tapered to 4 times daily by 1 month, thrice daily by 3 months, twice daily by 6 months, and once daily by 1 year.
Pre-existing glaucoma and ocular hypertension were defined according to the European Glaucoma Society Terminology and Guidelines for Glaucoma. IOP-lowering treatment included any of the following: use of topical or systemic ocular hypotensive medication(s), or both; performance of laser peripheral iridotomy, iridoplasty, trabeculoplasty, or cyclodestructive procedure(s); and glaucoma filtration surgery with or without the use of antimetabolites, including glaucoma drainage device(s).
The IOP measurements were obtained at each postoperative visit. This was typically on the first and fifth postoperative day; second postoperative week; and first, second, third, sixth, ninth, and twelfth postoperative month. IOP measurements obtained at all visits between and after these typical periods also were included.
The mean postoperative IOP for each eye was calculated by averaging the IOP measurements at different postoperative times. Change in IOP before and after DSAEK was calculated by subtracting the preoperative IOP from the postoperative average IOP for each eye, and the mean of all the differences was calculated for all included eyes.
The mean highest IOP after DSAEK was calculated by dividing the sum of all the highest IOPs of each eye after DSAEK by the number of eyes. Similarly, the mean lowest IOP after DSAEK was calculated by dividing the sum of all the lowest IOPs of each eye after DSAEK by the number of eyes. IOP range after DSAEK was the difference between the minimum and maximum IOP recorded after DSAEK, and the mean range of IOP after DSAEK was calculated by dividing the sum of differences between maximum and minimum IOP of each eye after DSAEK by the number of eyes.
Additional intraoperative procedures at time of DSAEK referred to additional procedures not performed routinely in a standard DSAEK operation as described above, and included lens extraction by phacoemulsification, synechiolysis, anterior chamber intraocular lens exchange, and vitrectomy.
The main outcome measures were graft failure and the need for additional IOP-lowering treatment after DSAEK. Graft failure was defined as an irreversible edematous change of the cornea, with increased corneal thickness and poor visual acuity of 6/60 or worse, for a minimum of 2 months. Eyes with increased central corneal thickness alone and otherwise good cornea clarity, good visual acuity, or both were not considered to be graft failures. Additional IOP-lowering treatment after DSAEK was defined as the need for additional topical or systemic IOP-lowering medication, the performance of glaucoma filtration surgery or bleb needling with adjunctive antimetabolites, for example, 5-fluorouracil, to rescue an existing failing bleb, or glaucoma laser procedures aimed at lowering IOP after DSAEK, or a combination thereof. Additional IOP-lowering treatment was instituted when the intraocular pressure was more than 21 mm Hg.
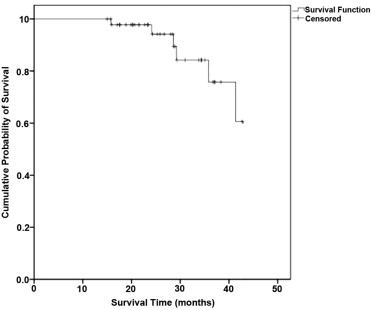
Statistical analysis was performed using SPSS software version 13.0 (SPSS, Inc, Chicago, Illinois, USA). Kaplan-Meier survival analysis was used to estimate the risk of graft failure ( Figure ). Univariate analysis was performed using the chi-square or t test as appropriate. Multivariate analysis was performed using logistic regression analysis for association of the main outcome measures of graft survival and need for additional IOP-lowering treatment after DSAEK with the following variables: age at time of DSAEK, gender, race, duration of follow-up, indications for DSAEK, pre-existing glaucoma diagnoses, interval between glaucoma diagnosis and DSAEK, IOP before DSAEK, glaucoma interventions and treatment before DSAEK, additional intraoperative procedures at the time of DSAEK, and IOP indices after DSAEK (mean IOP after DSAEK, change in mean IOP before and after DSAEK, and IOP range after DSAEK). Statistical significance was defined as P < .01.
Results
A total of 184 eyes underwent DSAEK from January 2007 through May 2009. A total of 47 eyes with pre-existing glaucoma or ocular hypertension were included. No eyes were excluded because of insufficient follow-up. The mean ± standard deviation (SD) age at the time of DSAEK was 66.6 ± 9.4 years, 24 (51.1%) of 47 patients were male, and 41 (87.2%) of 47 patients were Chinese. The mean ± SD duration of follow-up after DSAEK was 27.3 ± 8.5 months (range, 15.0 to 43.4 months). The main indications for DSAEK were pseudophakic bullous keratopathy (31.9%) and bullous keratopathy after laser peripheral iridotomy (23.4%).
Most pre-existing glaucoma diagnoses were secondary open-angle glaucoma (38.3%), primary angle-closure glaucoma (14.9%), and secondary angle-closure glaucoma (12.8%). Twenty-four eyes (51.1%) had closed angles and 24 (51.1%) of 47 patients had secondary glaucoma, with an overall mean ± SD interval between glaucoma diagnosis and DSAEK of 75.4 ± 69.3 months (range, 2.4 to 400.8 months). The preoperative characteristics of 47 eyes with pre-existing glaucoma undergoing DSAEK are summarized in Table 1 .
| No. | % | |
|---|---|---|
| Indications for DSAEK | ||
| PBK with PCIOL | 11 | 23.4% |
| PBK with ACIOL | 4 | 8.5% |
| BK after LPI | 11 | 23.4% |
| PBK with previous LPI | 3 | 6.4% |
| Failed penetrating keratoplasty | 11 | 23.4% |
| Fuchs endothelial dystrophy | 5 | 10.6% |
| Posterior polymorphous dystrophy | 1 | 2.1% |
| BK after glaucoma filtration surgery | 1 | 2.1% |
| Pre-existing glaucoma diagnoses | ||
| Acute primary angle closure | 2 | 4.3% |
| Primary angle closure | 4 | 8.5% |
| Primary angle-closure suspect | 5 | 10.6% |
| Primary angle-closure glaucoma | 7 | 14.9% |
| Primary open-angle glaucoma | 3 | 6.4% |
| Secondary angle-closure glaucoma | 6 | 12.8% |
| Secondary open-angle glaucoma | 18 | 38.3% |
| Ocular hypertension | 2 | 4.3% |
| Glaucoma filtration surgery before DSAEK | 14 | 29.8% |
| Trabeculectomy | 5 | |
| Trabeculectomy with 5-fluorouracil | 1 | |
| Trabeculectomy with mitomycin C | 6 | |
| Glaucoma drainage device | 1 | |
| Trabeculectomy and glaucoma drainage device | 1 |
Before DSAEK, 17 (36.2%) of 47 patients had undergone laser peripheral iridotomy, 14 (29.8%) of 47 patients had undergone prior glaucoma filtration surgery with antimetabolites, and 28 (59.6%) of 47 patients were taking at least 1 topical antiglaucoma medication, with the mean ± SD number of topical antiglaucoma medications being 0.94 ± 0.96.
Visual acuity before DSAEK was 6/60 or worse in 32 (68.1%) of 47 patients and 6/12 or better in 1 (2.1%) of 47 patients. The mean ± SD change in Snellen visual acuity after DSAEK was 5.40 ± 3.73 Snellen lines, with 36 (76.6%) of 47 patients improving by 2 or more Snellen lines, 11 (23.4%) of 47 patients maintaining vision within 2 Snellen lines, and none losing 2 or more Snellen lines of vision. At the last follow-up, 24 (51.1%) of 47 patients had visual acuity of 6/12 or better, which was statistically higher when compared with that before surgery ( P < .001).
Eight (17%) posterior lamellar grafts failed, after a mean ± SD interval of 12.8 ± 6.97 months after DSAEK (range, 2.0 to 25.1 months). Three (37.5%) underwent a repeat DSAEK, with 1 (33.3%) of 3 having a second DSAEK graft failure 12.1 months after repeat DSAEK. Four (50%) grafts failed secondary to endothelial rejection, 2 (25%) after additional intraocular procedures (repositioning of intraocular lens, trabeculectomy with mitomycin C complicated by gross hyphema), 1 (12.5%) because of a central graft–host dislocation cleft that failed to resolve after rebubbling (the patient declined further treatment), and 1 (12.5%) secondary to cytomegalovirus endotheliitis. The Kaplan-Meier estimated probabilities of graft survival at 1 and 2 years are 100% and 94.2%, respectively.
We included a control group of 137 eyes that underwent DSAEK by the same group of surgeons during the same period (January 2007 through May 2009), followed up to May 2010 (similar end point as the study group), but without pre-existing glaucoma. At the end of the study period, there were 8 (5.8%) graft failures in the control group. The percentage of DSAEK graft failures in eyes with pre-existing glaucoma (8/47; 17.0%) is not significantly higher than that in eyes without pre-existing glaucoma (11/137; 8.0%; P = .08).
The mean ± SD IOP before DSAEK was 13.9 ± 4.3 mm Hg. This increased by a mean of 2.1 ± 4.1 mm Hg to 16.0 ± 2.5 mm Hg after DSAEK ( P = .006; 95% confidence interval [CI] of difference, 0.6 to 3.5). The mean highest, lowest, and range of IOP after DSAEK were 27.4 ± 8.9 mm Hg, 9.2 ± 2.6 mm Hg, and 18.2 ± 9.6 mm Hg, respectively.
After DSAEK, 35 (74.5%) of 47 eyes were receiving at least 1 topical antiglaucoma medication (compared with 28 of 47 eyes before DSAEK; P = .05). The mean ± SD number of topical antiglaucoma medications after DSAEK was 2.0 ± 1.5, which equates to an increase of 1.1 ± 1.4 compared with that before DSAEK ( P < .001). Although 3 (6.4%) of 47 eyes required less IOP-lowering treatment after DSAEK, most (29/47; 61.7%) required additional IOP-lowering treatment after DSAEK. Twenty-one of these eyes (72.4%) required additional topical medication(s) only, whereas 8 (27.6%) of 29 eyes required glaucoma filtration surgery in addition to an increase in the number of topical medications administered, after a mean ± SD of 9.3 ± 6.9 months after DSAEK.
Of the 28 eyes that were receiving at least 1 topical antiglaucoma medication before DSAEK, 3 (10.7%) of 28 eyes required fewer antiglaucoma medications, 7 (25%) of 28 eyes required the same number of antiglaucoma medications, and 18 (64.3%) of 28 eyes required more antiglaucoma medications after DSAEK. Seven (25%) of the 28 eyes required subsequent trabeculectomy for IOP control.
Before DSAEK, 23 eyes achieved control of IOP with topical antiglaucoma medication alone and 9 eyes achieved control of IOP with glaucoma filtration surgery alone, whereas 5 eyes required both glaucoma filtration surgery and topical antiglaucoma medication for IOP control.
Of the 23 eyes requiring topical antiglaucoma medication alone before surgery, 1 (4.3%) required fewer topical medications, 4 (17.4%) required the same number of topical medications, 11 (47.8%) required additional topical medications alone, 2 (8.7%) required trabeculectomy alone, and 5 (21.7%) required trabeculectomy and topical medication together for IOP control after surgery.
In our series, 14 eyes (30%) had undergone glaucoma filtration surgery before DSAEK. Twelve eyes (85.7%) had undergone trabeculectomy with antimetabolites, 1 (7.1%) had undergone insertion of a glaucoma drainage device, and 1 (7.1%) had undergone 2 previous trabeculectomies as well as 2 glaucoma drainage device implantations before DSAEK. Additionally, all of these 14 eyes with previous trabeculectomies were receiving topical antiglaucoma medication before DSAEK. After DSAEK, 2 (14.3%) of 14 eyes required fewer topical antiglaucoma medications, 8 (57.1%) of 14 required the same number of topical antiglaucoma medications, and 4 (28.6%) of 14 required more topical antiglaucoma medications. Bleb needling with antimetabolites was not performed for any of these eyes. One eye (7.1%) proceeded on to require repeat trabeculectomy for IOP control.
On univariate analysis, demographics, indications for DSAEK, glaucoma diagnosis, the interval between glaucoma diagnosis and DSAEK, glaucoma treatment before DSAEK, secondary intraoperative procedures during DSAEK, IOP indices after DSAEK, and glaucoma treatment after DSAEK were not statistically significantly associated with graft failure after DSAEK ( Table 2 ).
| Risk Factors for Graft Failure | P Value | Odds Ratio | 95% Confidence Interval |
|---|---|---|---|
| Demographics | |||
| Age at DSAEK | .701 | 0.985 | 0.910 to 1.066 |
| Gender | .481 | 0.570 | 0.119 to 2.721 |
| Race | .171 | 4.000 | 0.548 to 29.174 |
| Duration of follow-up after DSAEK | .031 | 1.106 | 1.009 to 1.211 |
| Indications for DSAEK | |||
| Failed penetrating keratoplasty | .310 | 0.430 | 0.084 to 2.193 |
| Previous LPI | .999 | NA | NA |
| Pseudophakic bullous keratopathy | .647 | 1.500 | 0.265 to 8.489 |
| Glaucoma pathogenesis | |||
| Angle closure | .122 | 3.882 | 0.695 to 21.701 |
| Secondary glaucoma | .481 | 0.570 | 0.119 to 2.721 |
| Interval between glaucoma diagnosis and DSAEK | .484 | 0.995 | 0.980 to 1.010 |
| Pre-DSAEK IOP-lowering treatment | |||
| Pre-DSAEK LPI | .157 | 4.870 | 0.545 to 43.523 |
| Pre-DSAEK glaucoma filtration surgery | .498 | 0.575 | 0.116 to 2.851 |
| Interval between pre-DSAEK glaucoma surgery and DSAEK | .627 | 0.994 | 0.969 to 1.019 |
| No. of topical ocular hypotensive medications before DSAEK | .836 | 1.086 | 0.497 to 2.371 |
| Secondary intraoperative procedures during DSAEK | .187 | 4.375 | 0.488 to 39.184 |
| Post-DSAEK IOP indices | |||
| Mean IOP after DSAEK | .105 | 0.774 | 0.568 to 1.055 |
| Maximum IOP after DSAEK | .278 | 0.934 | 0.826 to 1.056 |
| Range of IOP after DSAEK | .732 | 0.985 | 0.906 to 1.071 |
| Post-DSAEK IOP-lowering treatment | |||
| No. of topical ocular hypotensive medications after DSAEK | .859 | 1.049 | 0.617 to 1.783 |
| Additional IOP-lowering treatment after DSAEK | .135 | 3.333 | 0.688 to 16.161 |
| Trabeculectomy after DSAEK | .710 | 1.531 | 0.162 to 14.517 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


