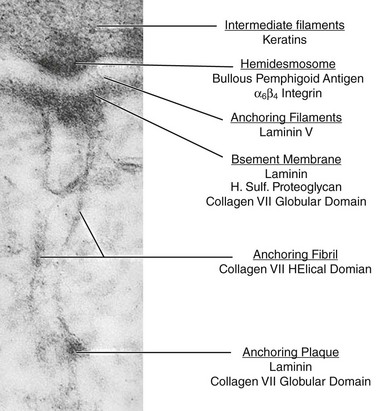
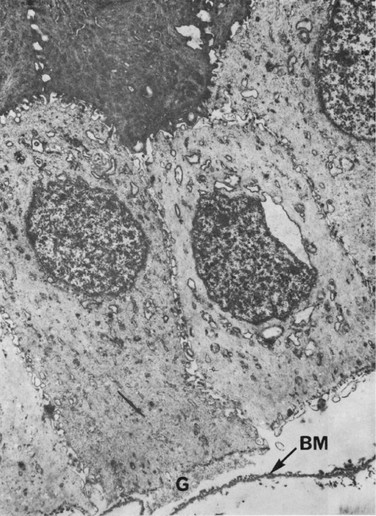
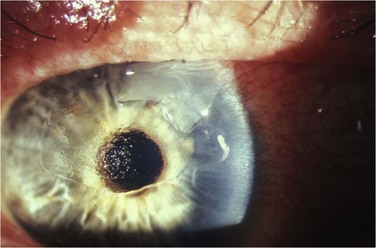
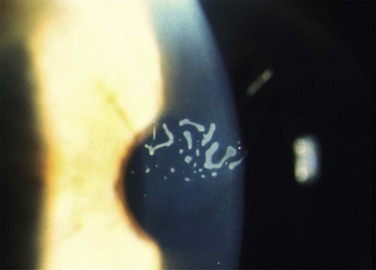
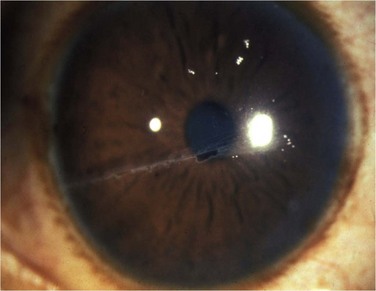
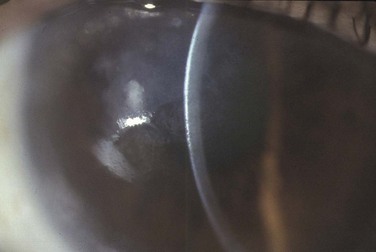
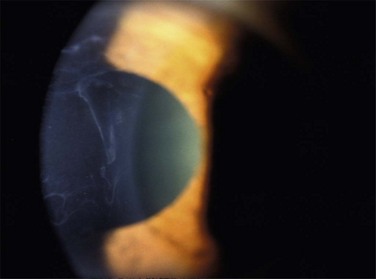
26 Normal Anatomy of the Epithelial Adhesion Complex There are two major adherence mechanisms for corneal epithelial cells to adhere to basement membrane. One mechanism is through direct molecular interaction of receptors with ligands located in the extracellular matrix. Three major families of such molecular interactions have been identified. These include the N-CAM family, the cadherin family, and the integrins, which are a family of integral membrane proteins interacting with an extracellular matrix ligand at cell–matrix interfaces.1 The second mechanism of cell–matrix adhesion is through adhesive junctions, called hemidesmosomes (Fig. 26.1).2 The hemidesmosomes are located on the basal membranes of the epithelial cells. On the external side of the cell membrane at the hemidesmosome, an electron-dense line parallels the membrane and, from it, anchoring filaments extend through the lamina lucida to the lamina densa of the basement membrane (Fig. 26.1). Opposite the lamina densa, anchoring fibrils insert from the stromal side. These fibrils form an intertwining network in the anterior stroma. Distal from their insertions in the basement membrane, anchoring fibrils insert into anchoring plaques, which appear structurally as small segments of basement membrane (Fig. 26.1). Collectively, all these structurally linked components, including intermediate filaments, hemidesmosomes, anchoring filaments, anchoring fibrils and anchoring plaques, are termed the adhesion complex.3 As basal cells of the corneal epithelium begin to migrate to cover a wound, they lose their hemidesmosomes.4 Re-establishment of the tight adhesion of the corneal epithelium is associated with re-formation of hemidesmosomes and components of the adhesion complex.5 An interim adhesion junction, termed ‘focal adhesion,’ is constructed along the cell–matrix interface of epithelial cells during migration, as evident by a dramatic increase in protein synthesis during migration to cover a wound.6 Ultrastructural studies of the cornea in RCE have demonstrated defective junctional complexes following epithelial trauma, resulting in delayed adhesion of epithelial cells to underlying structures (Fig. 26.2).5,7 These adhesion complex defects are characterized primarily by the focal absence of the basement membrane and of the hemidesmosomes. The basement membrane may appear multilayered and folded between epithelial cells. In addition, some of the basal corneal epithelial cells appear pale and swollen.7,8 Areas of healthy epithelium contain intraepithelial pseudocysts, with collections of cellular and amorphous debris.7 This cellular debris is probably the result of entrapment of the epithelium by aberrant basement membrane. The abnormal adhesion complexes between the basal epithelial cells and the basement membrane, may lead to focal areas of elevation of the epithelium and the accumulation of underlying cellular debris (Fig. 26.2). This leads to formation of abnormal basement membrane, with further focal detachments of the basal epithelium and accumulation of cellular debris, leading to a vicious cycle of aberrant epithelial adhesion and recurrent erosions. The timing of the erosion corresponds with an abrupt opening of the lids, which is why these episodes occur at night time or while awakening from sleep in the morning. During sleep and lid closure, there is no air between the lids and the tear film, and the surface tension of the tears creates sealing of the lid margins. Abrupt opening the lids creates a shearing force, which is greater than the force of adherence of the epithelium to its basement membrane, and this may result in epithelial avulsion.9 A higher incidence of severe meibomian gland disease (MGD) and acne rosacea was noted in non-traumatic RCE.10 These patients had inspissation of the meibomian glands, reduced tear film break-up time, conjunctival injection, and facial manifestations of acne rosacea, including facial erythema, flushes, papules, and pustules. The location of the corneal erosions was at the inferior cornea, which was explained by a longer contact with the tear film, containing its inflammatory mediators, typical of MGD.10 MGD is associated with higher levels of inflammatory cytokines and matrix-degrading enzymes in the tear film, which may potentially disturb the normal healing process, by interfering with the formation of normal hemidesmosomes and adhesion complexes. Increased bacterial lipase has been demonstrated in patients with MGD, which is responsible for the production of free fatty acids, which can interfere with the assembly of the adhesion complexes.11,12 In addition, inflammatory cytokines and matrix-degrading enzymes, such as interleukin-1 and MMP-9 were found to be elevated in the tears of patients with MGD,13 further contributing to the damaged healing patterns of the corneal epithelium in RCE. Elevated levels of MMP-2 and MMP-9 have been observed in the tear fluid of patients with RCE. These matrix-degrading enzymes were found to be up-regulated in human epithelia affected by recurrent erosion. These enzymes are concentrated in basal epithelial cells where they may play an important role in degradation of the epithelial anchoring system and result in recurrent epithelial slippage and erosion.14 Recurrent corneal erosions are the clinical end result of multiple disorders of the corneal epithelium and basement membrane. Although most of the patients with unilateral RCE will present after a history of acute trauma to the cornea with sloughing or erosion of the corneal epithelium (Fig. 26.3), careful consideration must be given to a wide spectrum of causes, specifically in patients with a bilateral disease, having no prior injury to the cornea. The etiology of RCE may be classified into primary and secondary disorders (Box 26.1).9 Primary disorders include genetic disorders, chiefly the corneal dystrophies that involve the epithelium, basement membrane or anterior stroma. Primary disorders are usually bilateral, symmetrical, and may occur in multiple locations in the cornea. The most common of these etiologies is the map-dot finger print dystrophy (Figs 26.4, 26.5). RCE is a common manifestation in lattice dystrophy, which involves the anterior stroma (Fig. 26.6).15 Box 26.1 Etiology of RCE Genetically related basement membrane abnormalities (dystrophies) After Ramamurthi S, Rahman MQ, Dutton GN, et al. Pathogenesis, clinical features and management of recurrent corneal erosions. Eye (Lond) 2006;20:635–644. Figure 26.4 Map-like changes in epithelial basement membrane dystrophy. (Courtesy Peter Laibson, MD.) The secondary basement membrane disorders leading to RCE are more common. They are usually acquired disorders, appear in one eye, and are often limited to a single location in the cornea. Of these, minor trauma to the corneal epithelium is the most common cause for RCE. Trauma to the epithelium can be caused by a fingernail, plant material, sharp domestic objects, or the edge of a piece of paper (Fig. 26.7).16 Salzmann’s nodular degeneration is another common acquired disorder that may be associated with recurrent erosions (Fig. 26.8).
Corneal Epithelial Adhesion Disorders
Pathophysiology
Epithelial Cell Adhesions in Recurrent Corneal Erosions
Meibomian Gland Disease and Inflammatory Mediators
Etiology
Corneal Epithelial Adhesion Disorders