Physiology: Introduction
The cornea functions both as a protective barrier and as a “window” through which light rays pass to the retina. Its transparency is due to its uniform structure, avascularity, and deturgescence (see Chapter 1). Deturgescence, or the state of relative dehydration of the corneal tissue, is maintained by the bicarbonate “pump” provided by the endothelium and the barrier function of the epithelium and endothelium. The endothelium is more important than the epithelium in the mechanism of dehydration, and damage to the endothelium is far more serious than damage to the epithelium. Destruction of the endothelial cells causes edema of the cornea and loss of transparency, which is more likely to persist because of the limited potential for recovery of endothelial function. Damage to the epithelium usually causes only transient, localized edema of the corneal stroma that clears with the rapid regeneration of epithelial cells. Evaporation of water from the precorneal tear film produces hypertonicity of the film. Together with direct evaporation, this draws water from the superficial corneal stroma in order to maintain the state of dehydration.
Penetration of the intact cornea by drugs is biphasic. Fat-soluble substances can pass through intact epithelium, and water-soluble substances can pass through intact stroma. Therefore, to pass through the cornea, drugs must be soluble in both lipids and water.
The epithelium is an efficient barrier to the entrance of microorganisms into the cornea. If the epithelium is defective, the avascular stroma and Bowman’s layer become susceptible to infection with a variety of organisms, including bacteria, Acanthamoeba, and fungi. Streptococcus pneumoniae (the pneumococcus) is a true bacterial corneal pathogen; other pathogens require a heavy inoculum, compromised barrier function, or a relative immune deficiency to produce infection.
Moraxella liquefaciens, which occurs mainly in alcoholics (as a result of pyridoxine depletion), is a classic example of the bacterial opportunist, and in recent years a number of new corneal opportunists have been identified. Among them are Serratia marcescens, Mycobacterium fortuitum-chelonei complex, viridans streptococci, Staphylococcus epidermidis, and various coliform and proteus organisms, along with viruses, Acanthamoeba, and fungi.
Local or systemic corticosteroids modify the host immune reaction in several ways and may allow opportunistic organisms to invade and flourish.
Since the cornea has many pain fibers, most superficial or deep corneal lesions cause pain and photophobia. The pain of epithelial disease is worsened by movement of the lids (particularly the upper lid) over the cornea and usually persists until healing occurs. Since the cornea serves as the “window” of the eye and refracts light rays, corneal lesions usually blur vision, especially if centrally located.
Photophobia in corneal disease is the result of painful contraction of an inflamed iris. Dilation of iris vessels is a reflex phenomenon caused by irritation of the corneal nerve endings. Photophobia, severe in most corneal disease, is minimal in herpetic keratitis because of the hypesthesia associated with the disease, which can be a valuable diagnostic sign.
Although tearing and photophobia commonly accompany corneal disease, there is usually no discharge except in purulent bacterial ulcers.
Obtaining a thorough history is important. A history of trauma can often be elicited, foreign bodies and abrasions being the two most common corneal lesions, and eliciting any history of corneal disease in the patient or the family can be critical. The keratitis of herpes simplex infection is often recurrent, but since recurrent erosion is extremely painful and herpetic keratitis is not, these disorders can be differentiated by their symptoms. The patient’s use of topical medications should be investigated, since corticosteroids may have been used and may have predisposed to bacterial, fungal, or viral disease, especially herpes simplex keratitis. Immuno-suppression also occurs with systemic diseases, such as diabetes, AIDS, and malignant disease, as well as with specific immunosuppressive therapy. All medications and preservatives can cause contact dermatitis or corneal toxicity; the importance of toxicity as a cause of corneal and conjunctival disease should not be underestimated.
The keys to examination of the cornea are adequate illumination and magnification. The slitlamp is essential in proper examination of the cornea; in its absence, a loupe and bright illumination can be used for gross inspection. Examining the light reflection, while moving the light carefully over the entire cornea, will identify rough areas indicative of epithelial defects. Fluorescein staining can highlight superficial epithelial lesions that might otherwise not be apparent. Examination, particularly after trauma, is often facilitated by instillation of a local anesthetic, but sterile drops must be used. Confocal microscopy assists diagnosis, particularly in suspected Acanthamoeba or fungal infection.
To select the proper therapy for corneal infections, especially due to bacteria, fungi, or Acanthamoeba laboratory aid is essential. Since a delay in identifying the correct organism may severely compromise the ultimate visual result, it should be achieved as soon as possible. Examination of corneal scrapings, stained with Gram’s and Giemsa’s stains, may allow identification of the organism, particularly bacteria, while the patient waits. Polymerase chain reaction (PCR) may provide rapid identification of herpes viruses, Acanthamoeba, and fungi. Cultures for bacteria are usually obtained in all cases at first presentation. Cultures for fungi, Acanthamoeba, or viruses may be undertaken if the clinical features are typical or there is lack of response to treatment for bacterial infection. Appropriate therapy is instituted as soon as the necessary specimens have been obtained. It is important that therapy is not withheld if an organism cannot be identified on microscopic examination of corneal scrapings, although it may have to be empirical based upon the clinical features.
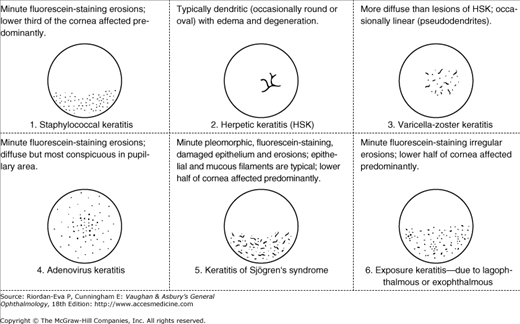
The corneal epithelium is involved in most types of conjunctivitis and keratitis and in rare cases may be the only tissue involved (eg, in superficial punctate keratitis). The epithelial changes vary widely from simple edema and vacuolation to minute erosions, filament formation, partial keratinization, etc. The lesions vary also in their location on the cornea. All of these features have important diagnostic significance (Figure 6–1), and slitlamp examination with and without fluorescein staining should be a part of every external eye examination.

There are a number of important types of discrete subepithelial lesions, often secondary to epithelial keratitis (eg, the subepithelial infiltrates of epidemic keratoconjunctivitis, caused by adenoviruses 8 and 19).
The responses of the corneal stroma to disease include infiltration, representing accumulation of inflammatory cells; edema manifested as corneal thickening, opacification, or scarring; “melting” or necrosis, which may lead to thinning or perforation; and vascularization. The patterns of these responses are less specific for disease entities than those seen in epithelial keratitis, and the clinician often must rely on other clinical information and laboratory studies for clear identification of causes.
Dysfunction of the corneal endothelium results in corneal edema, initially involving the stroma and later the epithelium. Stromal edema often produces “folds” or “wrinkles” in Descemet’s membrane. This contrasts with corneal edema due to raised intraocular pressure, in which the epithelium is affected before the stroma. As long as the cornea is not too edematous, it is often possible to visualize morphologic abnormalities of the corneal endothelium with the slitlamp. Inflammatory cells on the endothelium (keratic precipitates or “KPs”) are less commonly an indication of endothelial disease, when they are usually localized, than due to anterior uveitis, which may or may not accompany stromal keratitis, when they tend to be more generally distributed.
Corneal Ulceration
Cicatrization due to corneal ulceration is a major cause of blindness and impaired vision throughout the world (see Chapter 20). Most of this visual loss is avoidable by early diagnosis and prompt appropriate treatment, but also by minimizing predisposing factors.
Central ulcers usually are infectious ulcers secondary to corneal epithelial damage. The lesion is situated centrally, away from the vascularized limbus. It is often accompanied by hypopyon, a collection of inflammatory cells seen as a pale layer in the inferior anterior chamber that also occurs in severe anterior uveitis (see Chapter 7). Although hypopyon is sterile in bacterial corneal ulcers unless there has been a rupture of Descemet’s membrane, in fungal ulcers it may contain fungal elements.
Central suppurative ulceration was once caused almost exclusively by S pneumoniae infection complicating corneal trauma, particularly occurring in patients with obstructed nasolacrimal ducts. The commonest predisposing factor in developed countries has become contact lens wear, being particularly associated with Pseudomonas and Acanthamoeba keratitis. More widespread use of compromising systemic and local medications has increased the incidence of corneal ulcers due to opportunistic bacteria, fungi, and viruses.
Many types of bacterial corneal ulcers look alike and vary only in severity. This is especially true of ulcers caused by opportunistic bacteria (eg, alpha-hemolytic streptococci, Staphylococcus aureus, S epidermidis, Nocardia, and M fortuitum-chelonei), which often cause indolent corneal ulcers that tend to spread slowly and superficially.
Pneumococcal corneal ulcer usually manifests 24–48 hours after inoculation of an abraded cornea. It typically produces a gray, fairly well-circumscribed ulcer that tends to spread erratically from the original site of infection toward the center of the cornea. The advancing border shows active ulceration and infiltration as the trailing border begins to heal. (This creeping effect gave rise to the term “acute serpiginous ulcer.”) The superficial corneal layers become involved first, and then the deep parenchyma. The cornea surrounding the ulcer is often clear. Hypopyon is common. Scrapings from the leading edge of a pneumococcal corneal ulcer usually contain gram-positive lancet-shaped diplococci. Drugs recommended for use in treatment are listed in Tables 6–1 and 6–2. Concurrent dacryocystitis and nasolacrimal duct obstruction should also be treated.
| Organisms | Initial Therapies2 | Alternative Therapies2 |
|---|---|---|
| No organisms identified; ulcer suggestiv of bacterial infection | Moxifloxacin, gatifloxacin, or tobramycin with cefazolin | Ciprofloxacin, levofloxacin, gentamicin, ceftazidime, or vancomycin |
| Gram-positive cocci: lancet-shaped with capsule = S pneumoniae | Moxifloxacin, gatifloxacine, or cefazolin | Levofloxacin, penicillin G, vancomycin, or ceftaxidime |
| Gram-positive cocci: methacillin-resistant S aureus (MRSA) | Vancomycin | |
| Gram-positive rods: slender and varying in length—Mycobacterium fortuitum, Nocardia species, Actinomyces species | Amikacine, moxifloxacin, or gatifloxacin | Other fluoroquinolones |
| Other gram-positive organisms: cocci or rods | Cefazolin, moxifloxacin, or gatifloxacin | Other fluoroquinolones, penicillin G, vancomycin, or ceftazidime |
| Gram-negative cocci3 | Ceftriaxone3 | Penicillin G, cefazolin, or vancomycin |
| Gram-negative rods: thin = Pseudomonas | Moxifloxacin, gatifloxacin, ciprofloxaxin, tobramycin, or gentamicin | Other fluoroquinolones, polymyxin B, or carbenicillin |
| Gram-negative rods: large, a square-ended diplobacilli = Moraxella | Moxifloxacin, gatifloxacin, or ciprofloxacin | Tobramyin or getamicin with cefazolin, or penicillin G |
| Other gram-negative rods | Moxifloxacin, gatifloxacin, or tobramycin | Ceftazidime, getamicin, or carbenicillin |
| No organism identified; ulcer suggestive of fungal infection | Natamycin, voriconazole, or posaconazole | Amphotericin B, nystatin, miconazole, or flucytosine |
| Yeast-like organism = Candida species4 | Amphotericin B, voriconazole, or posaconazole | Amphotericin B, nystatin, miconazole, or flucytosine |
| Hyphae-like organisms = fungal ulcer | Natamycin, voriconazole, or posaconazole | Amphotericin B or nystatin |
| Cyst, trophozoites = Acanthamoeba | Propamidine and/or polyhexamethylene biguanide | Chlorhexidine or neomycin |
| Drug | Topical1 | Subconjunctival | Systemic |
|---|---|---|---|
| Amikacin | 50–100 mg/mL | 25 mg/0.5 mL/dose | 10–15 mg/kg/d IV or IM in two doses |
| Amphotericin B | 1.5–3 mg/mL | 0.5–1 mg | … |
| Carbenicillin | 4 mg/mL | 125 mg/0.5 mL/dose | 100–200 mg/kg/d IV in four doses |
| Cefazolin | 50 mg/mL | 100 mg/0.5 mL/dose | 15 mg/kg/d IV in four doses |
| Ceftazidime | 50 mg/mL | 250 mg (0.5 mL) | 1 g IV or IM every 8–12 hours (adult dose) |
| Ceftriaxone | … | … | 1–2 g/d IV or IM |
| Ciprofloxacin | 3 mg/mL | … | 500–750 mg orally every 12 hours |
| Flucytosine | 1% solution | … | 50–150 mg/kg/d orally in four doses |
| Gatifloxacin | 3 mg/mL solution | … | … |
| Gentamicin | 10–20 mg/mL (fortified) | 20 mg/0.5–1 mL/dose | … |
| Miconazole | 1% solution or 2% ointment | 5–10 mg; 0.5–1 mL/dose | … |
| Moxifloxacin | 5 mg/mL solution | … | … |
| Natamycin | 5% suspension | … | … |
| Neomycin | 20 mg/mL | … | … |
| Nystatin | 50,000 units/mL or cream (100,000 units/g) | … | … |
| Paromomyocin | 10 mg/mL | … | … |
| Penicillin G | 100,000 units/mL | 1 million units/dose (painful) | 40,000–50,000 units/kg IV in four doses; or continuously, 2–6 million units IV every 4–6 hours |
| Polyhexamethylene biguanide | 0.01%–0.02% solution | … | … |
| Polymyxin B | 1–2 mg/mL | 10 mg/0.5 mL dose | … |
| Posaconazole | 1% solution | 400 mg orally every 12 hours | |
| Propamidine | 0.1 mg/mL solution; 0.15% ointment | … | … |
| Tobramycin | 10–20 mg/mL (fortified) | 20 mg/0.5 mL/dose | … |
| Vancomycin | 50 mg/mL | 25 mg/0.5mL/dose | … |
| Voriconazole | 1% solution | 200–300 mg orally every 12 hours; or 200 mg every 12 hours IV |
Pseudomonas corneal ulcer begins as a gray or yellow infiltrate at the site of a break in the corneal epithelium (Figure 6–3). Severe pain is common. The lesion tends to spread rapidly in all directions because of the proteolytic enzymes produced by the organisms. Although superficial at first, the ulcer may quickly affect the entire cornea with devastating consequences, including corneal perforation and severe intraocular infection. There is often a large hypopyon that tends to increase in size as the ulcer progresses. The infiltrate and exudate may have a bluish-green color. This is due to a pigment produced by the organism and is pathognomonic of P aeruginosa infection.

Today, especially in developed countries, Pseudomonas corneal infection often is associated with soft contact lenses—especially extended-wear lenses. The organism has been shown to adhere to the surface of soft contact lenses. Some cases have been reported following the use of contaminated fluorescein solution or eye drops. It is mandatory that the clinician use sterile medications and sterile technique when caring for patients with corneal injuries.
Scrapings from the ulcer may contain long, thin Gram-negative rods that are often few in number. Drugs recommended for use in treatment are listed in Tables 6–1 and 6–2.
M liquefaciens (diplobacillus of Petit) causes an indolent oval ulcer that usually affects the inferior cornea and progresses into the deep stroma over a period of days. There is usually no hypopyon or only a small one, and the surrounding cornea is usually clear. M liquefaciens ulcer often occurs in a patient with alcoholism, diabetes mellitus, or other causes of immunosuppression. Scrapings may contain large, square-ended Gram-negative diplobacilli. Drugs recommended for use in treatment are listed in Tables 6–1 and 6–2. Treatment can be difficult and prolonged.
Central corneal ulcers caused by beta-hemolytic streptococci have no identifying features. The surrounding corneal stroma is often infiltrated and edematous, and there is usually a moderately large hypopyon. Scrapings often contain gram-positive cocci in chains. Drugs recommended for use in treatment are listed in Tables 6–1 and 6–2.
Central corneal ulcers caused by these organisms are now being seen more often, many of them in corneas compromised by topical corticosteroid use. The ulcers are often indolent, but may be associated with hypopyon and some surrounding corneal infiltration. They are often superficial, and the ulcer bed feels firm when scraped. Scrapings may contain Gram-positive cocci—singly, in pairs, or in chains. Infectious crystalline keratopathy (in which the cornea has a crystalline appearance) has been described in patients receiving long-term therapy with topical corticosteroids; the disease is often caused by alpha-hemolytic streptococci as well as nutritionally deficient streptococci. Tables 6–1 and 6–2 show recommended drug regimens.
Ulcers due to M fortuitum-chelonei and Nocardia are rare. They often follow trauma and are often associated with contact with soil. The ulcers are indolent, and the bed of the ulcer often has radiating lines that make it look like a cracked windshield. Hypopyon may or may not be present. Scrapings may contain acid-fast slender rods (M fortuitum-chelonei) or gram-positive filamentous, often branching organisms (Nocardia). See Tables 6–1 and 6–2 for recommended drug regimens.
Fungal corneal ulcers once were seen only in agricultural settings, but with the advent of contact lenses, immunosuppressive disease and corticosteroid use, these infections are seen in a variety of populations. The use of corticosteroids is not indicated in fungal disease; by altering the natural immune response and enhancing collagenase activity, these drugs are counterproductive.
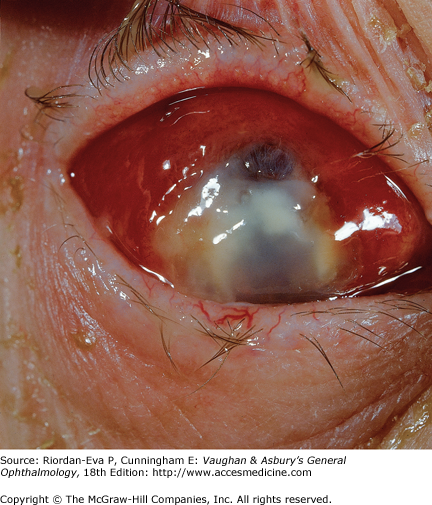
Fungal ulcers are indolent and have a gray infiltrate with irregular edges, often a hypopyon, marked inflammation of the globe, superficial ulceration, and satellite lesions (usually infiltrates at sites distant from the main area of ulceration) (Figure 6–4). Underlying the principal lesion—and the satellite lesions as well—there is often an endothelial plaque associated with a severe anterior chamber reaction. Corneal abscesses frequently occur.

Most fungal ulcers are caused by opportunists such as Candida, Fusarium, Aspergillus, Penicillium, Cephalosporium, and others. There are no identifying features that help to differentiate one type of fungal ulcer from another.
Scrapings from fungal corneal ulcers, except those caused by Candida, contain hyphal elements; scrapings from Candida ulcers usually contain pseudohyphae or yeast forms that show characteristic budding. Tables 6–1 and 6–2 list the drugs recommended for the treatment of fungal ulcers.
Herpes simplex keratitis occurs in two forms: primary and recurrent. It is the most common cause of both corneal ulceration and corneal blindness in the United States. The epithelial form is the ocular counterpart of labial herpes, with which it shares immunologic and pathologic features as well as having a similar time course. The only difference is that the clinical course of the keratitis may be prolonged because of the avascularity of the corneal stroma, which retards the migration of lymphocytes and macrophages to the lesion. Herpes simplex virus (HSV) ocular infection in the immunocompetent host is often self-limited, but in the immunologically compromised host, including patients treated with topical corticosteroids, its course can be chronic and damaging. Stromal and endothelial disease has previously been thought to be a purely immunologic response to virus particles or virally induced cellular changes. However, there is increasing evidence that active viral infection can occur within stromal and possibly endothelial cells as well as in other tissues within the anterior segment, such as the iris and trabecular endothelium. This highlights the need to assess the relative role of viral replication and host immune responses prior to and during therapy for herpetic disease. Topical corticosteroids may control damaging inflammatory responses but at the expense of facilitation of viral replication. Thus, whenever topical corticosteroids are to be used, antivirals are likely to be necessary. Any patient undergoing topical corticosteroid therapy for herpetic eye disease must be under the supervision of an ophthalmologist.
Serologic studies suggest that most adults have been exposed to the virus, although many do not recollect any episodes of clinical disease. Following primary infection, the virus establishes latency in the trigeminal ganglion. The factors influencing the development of recurrent disease, including its site, have yet to be unraveled. There is increasing evidence that the severity of disease is at least partly determined by the strain of virus involved. Most HSV infections of the cornea are still caused by HSV type 1 (the cause of labial herpes), but in both infants and adults, a few cases caused by HSV type 2 (the cause of genital herpes) have been reported. The corneal lesions caused by the two types are indistinguishable.
Scrapings of the epithelial lesions of HSV keratitis and fluid from skin lesions contain multinucleated giant cells. The virus can be cultivated on the chorioallantoic membrane of embryonated hens’ eggs and in many tissue cell lines—for example, HeLa cells, on which it produces characteristic plaques. In most cases, however, diagnosis can be made clinically on the basis of characteristic dendritic or geographic ulcers and greatly reduced or absent corneal sensation. PCR methods are used for accurate identification of HSV from tissue and fluid as well as from corneal epithelial cells.
Primary ocular herpes simplex is infrequently seen, but manifests as a vesicular blepharoconjunctivitis, occasionally with corneal involvement, and usually occurs in young children. It is generally self-limited, without causing significant ocular damage. Topical antiviral therapy may be used as prophylaxis against corneal involvement and as therapy for corneal disease.
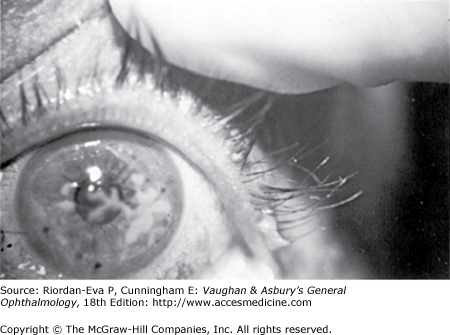
Attacks of the common recurrent type of herpetic keratitis (Figure 6–5) are triggered by fever, overexposure to ultraviolet light, trauma, the onset of menstruation, or some other local or systemic source of immunosuppression. Unilaterality is the rule, but bilateral lesions develop in 4%–6% of cases and are seen most often in atopic patients.

Symptoms— The first symptoms of an HSV infection are usually irritation, photophobia, and tearing. When the central cornea is affected, there is also some reduction in vision. Since corneal anesthesia usually occurs early in the course of the infection, the symptoms may be minimal and the patient may not seek medical advice. There is often a history of fever blisters or other herpetic infection, but corneal ulceration can occasionally be the only sign of a recurrent herpetic infection.
Lesions— The most characteristic lesion is the dendritic ulcer, which occurs in the corneal epithelium, has a typical branching, linear pattern with feathery edges, and has terminal bulbs at its ends (Figure 6–6). Fluorescein staining makes the dendrite easy to identify, but unfortunately herpetic keratitis can also simulate many corneal infections and must be considered in the differential diagnosis of many corneal lesions.
Geographic ulceration is a form of chronic dendritic disease in which the delicate dendritic lesion takes a broader form. The edges of the ulcer lose their feathery quality. Corneal sensation, as with dendritic disease, is diminished. The clinician should always test for this sign.
Other corneal epithelial lesions that may be caused by HSV are a blotchy epithelial keratitis, stellate epithelial keratitis, and filamentary keratitis. All of these are usually transitory, however, and often become typical dendrites within a day or two.
Subepithelial opacities can be caused by HSV infection. A ghost-like image, corresponding in shape to the original epithelial defect but slightly larger, can be seen in the area immediately underlying the epithelial lesion. The “ghost” remains superficial but is often enhanced by the use of antiviral drugs, especially idoxuridine. As a rule, these subepithelial lesions do not persist for more than a year.
Disciform keratitis is the most common form of stromal disease in HSV infection. The stroma is edematous in a central, disk-shaped area, without significant infiltration and usually without vascularization. The edema may be sufficient to produce folds in Descemet’s membrane. Keratic precipitates may lie directly under the disciform lesion but may also involve the entire endothelium because of the frequently associated anterior uveitis. The pathogenesis of disciform keratitis is generally regarded as an immunologic reaction to viral antigens in the stroma or endothelium, but active viral disease cannot be ruled out. Like most herpetic lesions in immunocompetent individuals, disciform keratitis is normally self-limited, lasting weeks to months. Edema is the most prominent sign, and healing can occur with minimal scarring and vascularization. A similar clinical appearance is seen with primary endothelial keratitis (endothelitis), which can be associated with anterior uveitis together with raised intraocular pressure and a focal inflammation of the iris. This is thought to be due to viral replication within the various anterior chamber structures.
Stromal HSV keratitis in the form of focal areas of infiltration and edema, often accompanied by vascularization, is likely to be predominantly due to viral replication. Corneal thinning, necrosis, and perforation may develop rapidly, particularly if topical corticosteroids are being used. If there is stromal disease in the presence of epithelial ulceration, it may be difficult to differentiate bacterial or fungal superinfection from herpetic disease. The features of the epithelial disease need to be carefully scrutinized for herpetic characteristics, but a bacterial or fungal component may be present and the patient must be managed accordingly. Stromal necrosis also may be caused by an acute immune reaction, again complicating the diagnosis with regard to active viral disease. Hypopyon may be seen with necrosis as well as secondary bacterial or fungal infection.
Peripheral lesions of the cornea can also be caused by HSV. They are usually linear and show a loss of epithelium before the underlying corneal stroma becomes infiltrated. (This is in contrast to the marginal ulcer associated with bacterial hypersensitivity, for example, to S aureus in staphylococcal blepharitis, in which the infiltration precedes the loss of the overlying epithelium.) Separation of the two disorders is important since the treatment of marginal immune ulcers can include use of corticosteroids, a medication not indicated the treatment of active viral infection. Testing for corneal sensation is unreliable in peripheral herpetic disease. The patient is apt to be far less photophobic than a patient with nonherpetic corneal disease.
The treatment of HSV keratitis should be directed at eliminating viral replication within the cornea while minimizing the damaging effects of the inflammatory response.
Debridement— An effective way to treat dendritic keratitis is epithelial debridement, since the virus is located in the epithelium and debridement will also reduce the viral antigenic load to the corneal stroma. Healthy epithelium adheres tightly to the cornea, but infected epithelium is easy to remove. Debridement is accomplished with a tightly wound cotton-tipped applicator. A cycloplegic/mydriatic agent such as homatropine 5% is then instilled into the conjunctival sac, and a pressure dressing is applied. The patient should be examined daily and the dressing changed until the corneal defect has healed, usually within 72 hours. Adjunctive therapy with a topical antiviral accelerates epithelial healing. Topical drug therapy without epithelial debridement for epithelial keratitis offers the advantage of not requiring patching but involves a hazard of drug toxicity.
Drug therapy—The topical antiviral agents used in herpetic keratitis are idoxuridine, trifluridine, vidarabine, ganciclovir, and acyclovir. (Topical acyclovir for ophthalmic use is not approved in the United States.) Ganciclovir and acyclovir are much more effective in stromal disease than the others. Idoxuridine and trifluridine are frequently associated with toxic epitheliopathy. Oral antivirals like acyclovir are of critical importance in the treatment of herpetic eye disease, particularly in atopic individuals who are susceptible to aggressive ocular and dermal (eczema herpeticum) herpetic disease. Dosage for active disease is 400 mg five times daily in nonimmunocompromised patients and 800 mg five times daily in compromised and atopic patients. Prophylactic dosage in recurrent disease is 400 mg twice daily. Famciclovir or valacyclovir may also be used.
Viral replication in the immunocompetent patient, particularly when confined to the corneal epithelium, usually is self-limited and scarring is minimal. It is thus unnecessary and potentially highly damaging to use topical corticosteroids. Regrettably, particularly when there is stromal disease, concerns about permanent scarring due to the corneal inflammation often result in the use of topical corticosteroids, but this is based on the misconception that reducing inflammation reduces disease severity. Even when the inflammatory response is thought to be purely immunologically driven, such as in disciform keratitis, topical corticosteroids are often best avoided if the episode is likely to be self-limited. Once topical corticosteroids have been used, this usually commits the patient to requiring the drug to control further episodes of keratitis, with the potential for uncontrolled viral replication and other steroid-related side effects, such as bacterial and fungal superinfection, glaucoma, and cataract. Topical corticosteroids may also accelerate corneal thinning, thus increasing the risk of corneal perforation. If it becomes necessary to use topical corticosteroids because of the severity of the inflammatory response, it is absolutely essential that appropriate antiviral therapy be used to control viral replication. Problems in the management of HSV keratitis are often due to inappropriate use of multiple topical treatments, including antivirals, antibiotics, and corticosteroids, resulting in adverse effects including epithelial toxicity. Frequently, using oral antivirals and tapering the corticosteroids will result in marked improvement.
Surgical treatment— Penetrating keratoplasty may be indicated for visual rehabilitation in patients with severe corneal scarring, but it should not be undertaken until the herpetic disease has been inactive for many months. Postoperatively, recurrent herpetic infection may occur as a result of the surgical trauma and the topical corticosteroids necessary to prevent corneal graft rejection. It may also be difficult to distinguish corneal graft rejection from recurrent stromal disease. Systemic antiviral agents should be used for several months after keratoplasty to cover the use of topical corticosteroids.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


