Cornea
Alex V. Levin
Thomas W. Wilson
David Rootman
Jerome Kazdan
The cornea develops from surface ectoderm (corneal epithelium) and neural crest cells (corneal stroma and endothelium). Developmental anomalies can result from inherited or spontaneous genetic mutations and insults during embryogenesis. Acquired disease can result from infection or other environmental or local contiguous processes. Multiple genes are involved in corneal formation. Mutations in these genes may result in isolated corneal malformation or associated abnormalities of the anterior and posterior segment.
As the most important refracting portion of the eye, corneal disease is likely to have a significant effect on vision. In the developing visual system of a child, superimposed amblyopia will almost certainly accompany most corneal disease. As the cornea has afferent neural pain fibers carried by the trigeminal nerve, photophobia and pain are also common symptoms of corneal disease. Its location does allow for topical treatment to be effective in many types of disease, but some corneal problems are not amenable to medical therapy. Corneal transplantation is available to clear the visual axis and relieve symptoms, but this process requires long-term follow-up and treatment, which itself can be uncomfortable and amblyogenic. In the setting of congenital obstruction of the visual axis, the poor success of infantile corneal transplantation has to be carefully weighed against the value of clearing the visual axis as soon as possible.
 Figure 5.1 Peters Anomaly Peters anomaly is due to defective separation of the lens, a surface ectoderm derivative, from the surface ectoderm during the fourth to seventh week of gestation. The resulting corneal opacity (left image), which is usually central, is associated with a defect in the posterior cornea (Descemet membrane and endothelium) to which the iris and/or lens remains attached (right image). The lens is often cataractous. It is bilateral in 80% of patients, and glaucoma is present in 50% of patients. When patients have associated heart defects, cleft palate, and skeletal anomalies, the syndrome is referred to as Peters Plus (Krause-Kivlin syndrome). Although most cases are sporadic, involvement of the PAX6, CYP1B1, and PITX2 has also been occasionally described. |
 Figure 5.2 Sclerocornea Sclerocornea is an opacification of the cornea, which is contiguous with the sclera. There is often associated microcornea, microphthalmia, or cornea plana. Visual prognosis is guarded even with early transplantation due to the associated ocular developmental abnormalities. Extensive vascularization may also contribute to corneal graft failure. Although the intraocular pressure may appear to be elevated by tonometry and glaucoma is associated, one must be careful to consider that the increased rigidity and thickness of the cornea may result in artifactitious measured pressure elevation. |
 Figure 5.3 Corneal Dermoid Corneal dermoids are round or oval vascular masses attached to the corneal surface. They often protrude, as seen here. They consist of ectodermally derived tissue and may contain hair and sweat glands within the corneal stroma. Therefore, these lesions are classified as choristomas. The lesions are most commonly located at the inferotemporal limbus but may also occur in the conjunctiva or central cornea. Astigmatic or occlusion amblyopia is a concern. Systemic associations include Goldenhar syndrome (Chapter 14: Craniofacial, Figs. 14.18, 14.19, 14.20 and 14.21). Lamellar keratoplasty and penetrating keratoplasty are performed for superficial and deep lesions, respectively. When isolated, this is usually a sporadic nongenetic anomaly. |
 Figure 5.4 Microcornea Microcornea is a corneal horizontal diameter of less than 10 mm after 2 years of age. Normative values for younger ages are also available. Microcornea can occur unilaterally or bilaterally and is associated with other ocular disorders including cataract, glaucoma, and coloboma. Note that microcornea can occur in the absence of microphthalmia (shortened axial length). There are numerous syndromic and chromosomal associations. Although vision is usually reduced, mild microcornea can be associated with vision as good as 6/12 in some patients. |
 Figure 5.5 Megalocornea Megalocornea is an increased horizontal diameter of greater than 13 mm by age 2 years. The intraocular pressure, cornea thickness, and endothelial density are typically normal. X-linked recessive transmission is typical, with affected males often having bilateral corneal diameters in excess of 14 mm and carrier females having diameters of 12 to 14 mm. Radial iris transillumination may be present. One characteristic sign, pictured here, is the ability to see the iridocorneal angle structures without gonioscopy. This can also be seen in some cases of buphthalmos due to infantile glaucoma, but there is no corneal edema or opacity in X-linked megalocornea. An autosomal recessive form (Neuhauser syndrome) associated with mental retardation is less common. |
 Figure 5.6 Congenital Cornea Ectasia Congenital corneal ectasia is a thinning and protrusion of the central cornea, if not a descemetocele or frank perforation at birth. Uveal tissue often lines the endothelial surface of the abnormal cornea. There is typically microphthalmia and increased intraocular pressure due to angle anomalies. Ectasia may be a manifestation of Peters anomaly (Fig. 5.1), congenital infections (e.g., cytomegalovirus, Chapter 19: Infectious Diseases, Figs. 19.9, 19.10 and 19.11), or an isolated ocular anomaly. Treatment includes urgent penetrating keratoplasty for tectonic support. Given the young age at which this procedure is required, the success rate is low. |
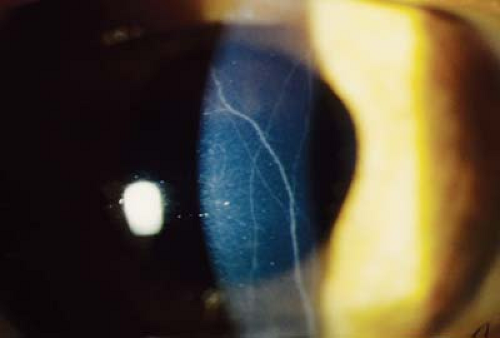 Figure 5.7 Prominent Corneal Nerves Increased visibility of corneal nerves in children is seen with neurofibromatosis type I, congenital glaucoma, keratoconus, multiple endocrine neoplasia type IIB, ichthyosis, corneal infection with herpes virus or acanthamoeba, leprosy, tuberculosis, and Refsum disease. The visual acuity is not typically affected by the corneal nerves but can be reduced by the associated ocular conditions. Corneal nerves are normally visible up to 2 mm anterior to the limbus. |
 Figure 5.8 Vertically Oval Cornea The normal cornea is typically oval with a wider horizontal diameter. When the cornea is vertically oval, it is otherwise normal and the vision is unaffected. Associated conditions include microphthalmia, interstitial keratitis, and Turner syndrome. No treatment is indicated. |
 Figure 5.9 Cornea Plana Cornea plana is an abnormally flat anterior corneal surface with corneal curvatures less than 40 diopters and often less than 36. The peripheral cornea is similar to sclera and may be more opaque than usual with features of sclerocornea (Fig. 5.2). Central cornea may also have decreased clarity. Most cases are sporadic, although autosomal dominant and autosomal recessive forms due to mutations in the keratocan gene at 12q also occur, as does association with systemic syndromes such as Ehlers-Danlos and Marfan. |
 Figure 5.10 Meesman Corneal Dystrophy
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|