(1)
Department of Pathology, Duke University Medical Center, Durham, NC, USA
Abstract
The cornea is a remarkable tissue; it can be thought of as “the window to the world.” Optimally – as with any window you are trying to see through – it must be clear and spotless. It is the eye’s main refractive element, and it normally is avascular.
Scarring, infection, inflammation, vascularization of the stroma, congenital anomalies, dystrophies, and neoplasia can be detrimental to vision. This chapter will introduce some of the basic and common pathology affecting the cornea.
The cornea and its tear film layer typically are not recognized when we look in our own eyes or the eyes of others. The tear film layer protects and coats the corneal surface and is composed of three distinct layers: from outer to inner they are the lipid layer, aqueous layer, and mucous layer. The lipid layer is produced by the meibomian (sebaceous) glands of the eyelid; the aqueous layer is produced by the serous glands of the lacrimal gland, and the mucous layer is produced by the goblet cells of the conjunctiva. A defective tear film layer can result in dry eye, which is a leading cause of eye-related disease.
The cornea is a remarkable tissue; it can be thought of as “the window to the world.” Optimally – as with any window you are trying to see through – it must be clear and spotless. It is the eye’s main refractive element, and it normally is avascular.
The cornea and its tear film layer typically are not recognized when we look in our own eyes or the eyes of others. The tear film layer protects and coats the corneal surface and is composed of three distinct layers: from outer to inner they are the lipid layer, aqueous layer, and mucous layer. The lipid layer is produced by the meibomian (sebaceous) glands of the eyelid; the aqueous layer is produced by the serous glands of the lacrimal gland, and the mucous layer is produced by the goblet cells of the conjunctiva. A defective tear film layer can result in dry eye, which is a leading cause of eye-related disease.
Scarring, infection, inflammation, vascularization of the stroma, congenital anomalies, dystrophies, and neoplasia can be detrimental to vision. This chapter will introduce some of the basic and common pathology affecting the cornea.
The normal cornea has five layers (Fig. 2.1). Let us examine the histology of each layer individually:
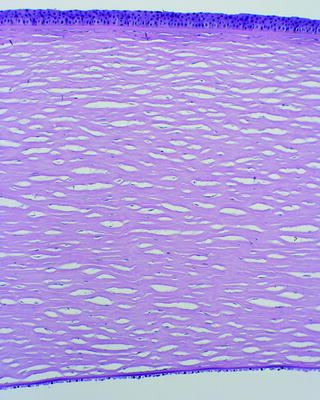
Fig. 2.1
Normal cornea showing the epithelium at the top of the field, Bowman’s layer, the corneal stroma, Descemet’s membrane, and corneal endothelium. The normal corneal stroma has an artifactual clefted or cracked appearance
1.
The surface epithelium (Fig. 2.2):
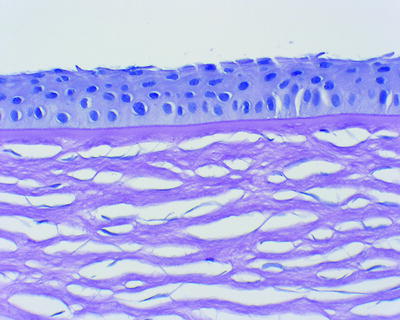
Fig. 2.2
Anterior cornea showing a nonkeratinized layer of squamous epithelium, a very thin basement membrane, Bowman’s layer, and the anterior stroma. The blue nuclei within the stroma are the nuclei of the keratocytes
Is normally four or five cell layers thick.
Is a nonkeratinizing squamous epithelium.
Has a smooth convex curvature.
In cases of corneal swelling (bullous keratopathy), the basal layer of epithelium may undergo significant hydropic change (Fig. 2.3).
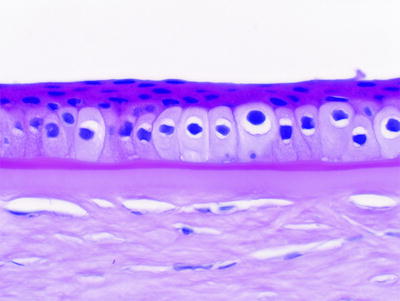
Fig. 2.3
Anterior cornea with hydropic change in the basal epithelial cells in a case of bullous keratopathy (corneal edema). Beneath the epithelium is a bright pink thickened basement membrane. This epithelial basement membrane is often not seen in hematoxylin and eosin-stained sections, although it can be thickened in certain diseases such as diabetes. Underlying the bright pink basement membrane is the light pink Bowman’s layer, and underneath that is the corneal stroma
There is a thin epithelial basement membrane which is often not recognizable histologically in normal corneas (although some authors may consider it to be its own layer). It can thicken in cases of trauma and diabetes (Fig. 2.3).
Following injury, the epithelium may become thickened (acanthosis) (Fig. 2.4).
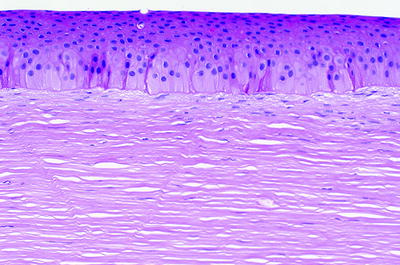
Fig. 2.4
Cornea with thickening or acanthosis of the epithelium, absence of Bowman’s layer, and scarring
2.
Bowman’s layer:
Named after Sir William Bowman, English ophthalmologist and anatomist (1816–1892). He also identified Bowman’s capsule in the kidney.
Bowman’s layer is a smooth eosinophilic band which acts as a protective barrier for the stroma.
Breaks or disruptions in Bowman’s layer are typically seen in cases of keratoconus (discussed below).
Pannus is fibrocollagenous or fibrovascular scar tissue between the epithelium and Bowman’s layer (see Fig. 2.5).
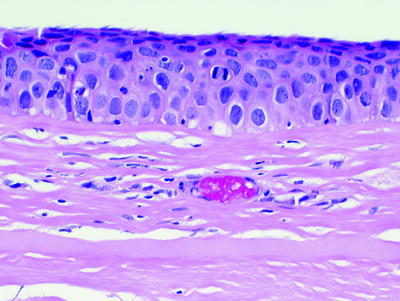
Fig. 2.5
Fibrovascular pannus between the cornea epithelium and Bowman’s layer. In this case, the overlying epithelium shows carcinoma in situ
Calcific band keratopathy is calcific stippling of Bowman’s layer.
3.
Stroma/substantia propria:
The stroma accounts for approximately 90% of the cornea. It is mostly collagen fibers, which, when examined ultrastructurally, are found to be in an organized pattern of alignment to reduce refraction of light. In contrast, the collagen fibers of the sclera are arranged haphazardly.
Identify the nuclei of the keratocytes. The keratocytes are the fibroblasts of the cornea, and they are not to be confused with the keratinocytes of the skin.
The normal corneal stroma is characterized by numerous cleft-like spaces. These spaces are artifacts; they are not lymphatics or blood vessels (vascularization of the cornea is abnormal and is bad for vision). Absence of these cleft-like spaces might indicate corneal swelling.
Following trauma, hemoglobin may stain the cornea and is known as corneal blood staining (Fig. 2.6).
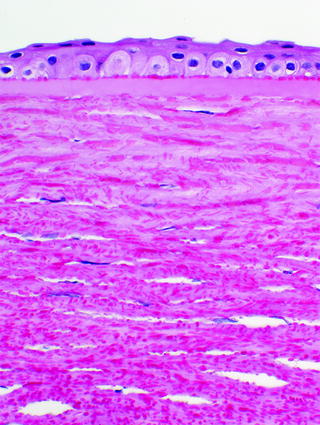
Fig. 2.6
Cornea with blood staining exhibiting innumerable blood fragments
The cornea is innervated by the ophthalmic branch of the trigeminal nerve. Peripheral nerve twigs are not normally seen in the cornea; however, they may become enlarged in certain clinical conditions including neurofibromatosis type 1 (Figs. 2.7, 2.8, 2.9).
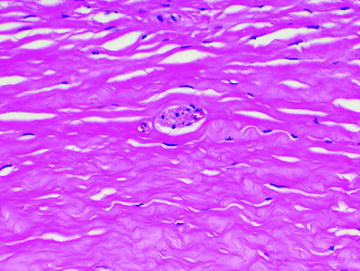
Fig. 2.7
Cornea stroma with a visible peripheral nerve twig. Peripheral nerves are typically too small to be seen on light microscopy
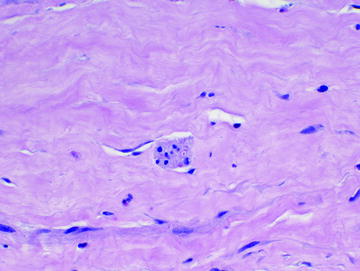
Fig. 2.8
Cornea stroma with a visible peripheral nerve twig. An axon in cross section is seen as a red dot
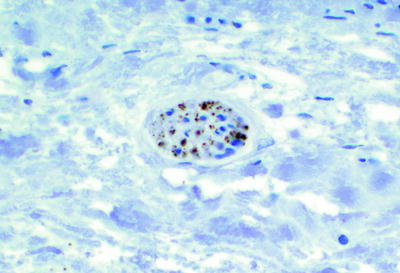
Fig. 2.9
Cornea peripheral nerve twig highlighted with a synaptophysin immunohistochemical stain
4.

Descemet’s membrane:
Get Clinical Tree app for offline access
Named after Jean Descemet, French physician (1732–1810).
The anterior gray band denotes the fetal/gestational layer of Descemet’s membrane (Fig. 2.10). This is a helpful clue in determining you are looking at Descemet’s membrane and not Bowman’s layer or the lens capsule. Additional nonbanded membrane is formed by the corneal endothelial cells throughout life.
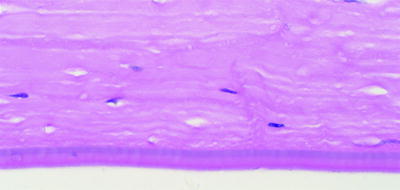
Fig. 2.10
Posterior corneal stroma and Descemet’s membrane. The gray band within the anterior aspect of Descemet’s membrane is the fetal/gestational banded layer of Descemet’s membrane. This is a useful clue to distinguish Descemet’s membrane from lens capsule or Bowman’s layer if the corneal epithelium is absent. Additional nonbanded Descemet’s membrane is formed by the corneal endothelial cells throughout life. In this case, Descemet’s membrane is markedly thickened, and there are no corneal endothelial cells
How do you know if Descemet’s membrane is too thick? It is advantageous to examine normal autopsy eye controls over a wide range of ages. Thickening of Descemet’s membrane and the presence of guttae are diagnostic features often seen in Fuchs’ corneal dystrophy (discussed below).
Posterior embryotoxon is a nodular prominence at the termination of Descemet’s membrane (thickening of Schwalbe’s line) (Fig. 2.11), but a fortuitous section is necessary to identify it in histological specimens.
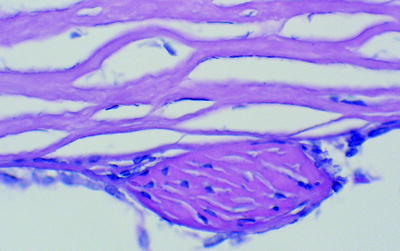
Fig. 2.11
Posterior corneal stroma showing a nodular prominence known as posterior embryotoxon. These are identified with fortuitous sections of the peripheral cornea. They represent the demarcation of the termination of Descemet’s membrane (Schwalbe’s line)< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

