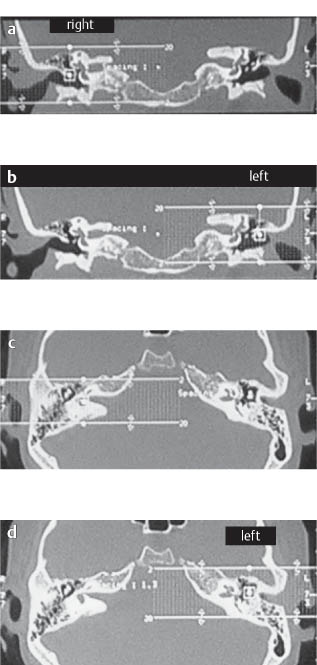
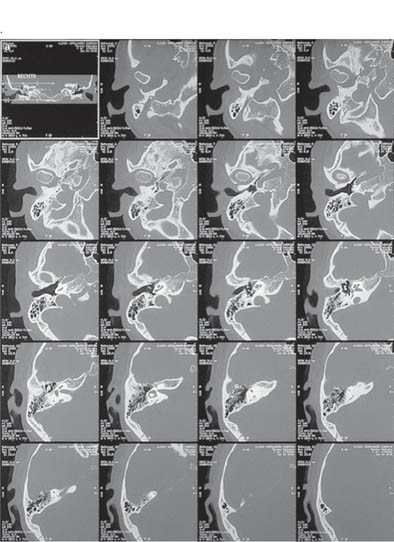
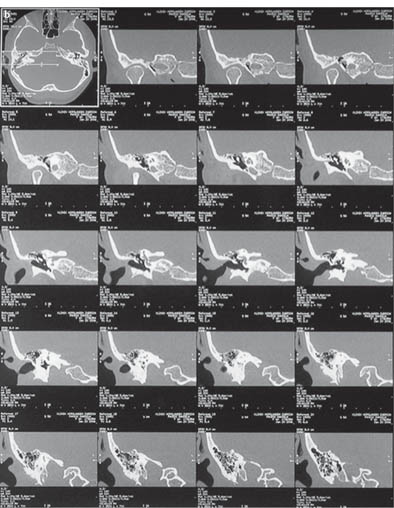
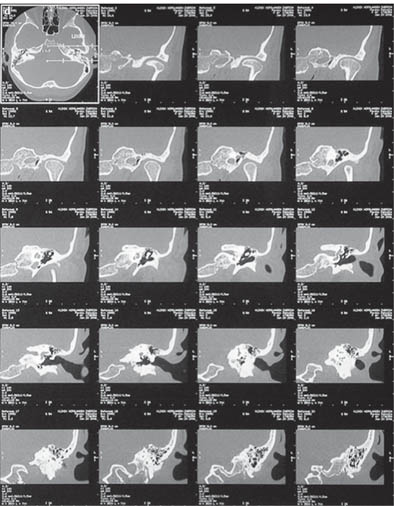
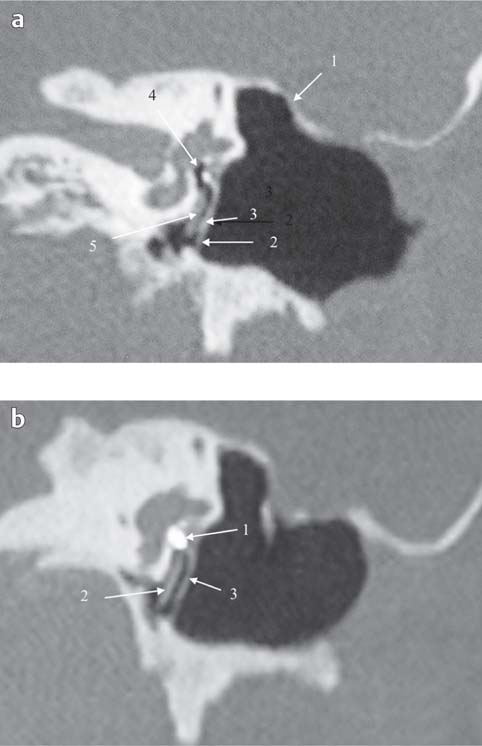
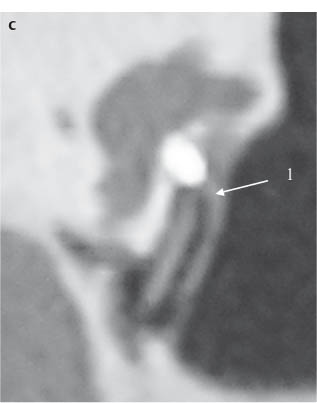
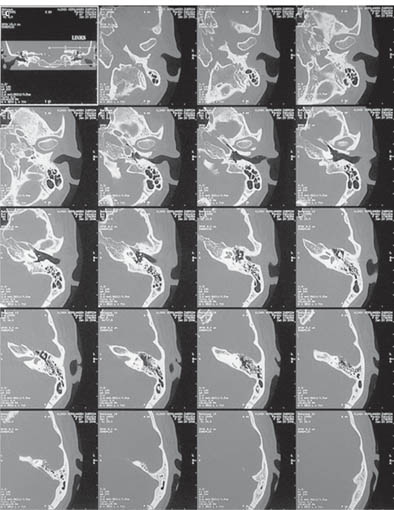
Chapter 9 Conventional and Multiplanar High-Resolution Computed Tomography of the Temporal Bone Middle ear surgery should today be referred to as temporal bone surgery. The development of otologic skull base surgery has familiarized the otologist with important structures of the temporal bone that were previously considered “untouchable” in an operative sense. A properly performed open tympanomastoidectomy (open epitympanomastoidectomy) requires the surgeon to have precise knowledge of the anatomy of the deepest structures of the temporal bone. This enables him or her to safely skeletonize the vertical semicircular canal, the labyrinthine segment of the fallopian canal, the middle cranial fossa dura, the sigmoid sinus, the jugular bulb, the vertical segment of the intrapetrous internal carotid artery (ICA), and the carotid bend. The preoperative anatomic knowledge necessary to carry out the complete exenteration and exteriorization of the retrofacial, retrolabyrinthine, supralabyrinthine, and supratubal cell tracts in the desired adequate and safe manner is best provided by pre-operative high-resolution computed tomography (HRCT). Familiarization with the anatomic variations and with the changes induced by pathology in the temporal bone is obtained by careful study of preoperative HRCT scans. The previously used lateral views give a rough estimation of the degree of pneumatization and of the position of the sigmoid sinus but are unable to provide sufficient information on the deep microscopic architecture of the temporal bone. Surprisingly, many otologists today are still proud to state that they do not need preoperative radiologic images unless the patient presents with complications. By this they mean that an experienced surgeon should be able to cope with any unforeseen intraoperative anatomic problem. This attitude is a dangerous overestimation of one’s own surgical skills because the key to safe surgery is the anticipation of possible intraoperative difficulties. This is why, even with the greatest experience, the information provided by HRCT can guide the hand of the surgeon on to the most secure and safe path. In this regard, the otologist can learn from the rhinologist, who would not dream of touching a nose without a CT scan! Why should this not hold true for otology in view of the fact that the temporal bone harbors some of our most valuable sensory organs? Many insurance companies have developed a very restrictive attitude toward preoperative HRCT in the otologic practice. It will take time and a lot of persuasive effort from the otologic front to change the situation. We are firmly convinced that the future of otology lies in superspecialization. Superspecialization connotes the accumulation of special experience needed to successfully solve intricate diagnostic, surgical, and medical problems in relation to a complicated human organ. The complexity of the ear and the temporal bone justify a special effort to preserve and restore the hearing function without injury to balance or the facial nerve. HRCT is an essential tool for understanding the pathology of the middle ear cleft. The advent of multiplanar reconstruction techniques for HRCT has opened up new possibilities for the evaluation of the preoperative and postoperative microanatomy of the ear, and a more liberal attitude toward the use of imaging techniques is required to achieve the necessary expertise for adequate management of ear diseases. A well-prepared operation carried out on the basis of solid clinical experience and with the information provided by conventional and multiplanar reconstruction HRCT scans will lead to a global reduction in surgical costs as the operative success rate will increase and the number of unnecessary surgical procedures will be reduced. In the future the otologist and radiologist will have to learn to work together. The otologist will need to be as adept as the radiologist in reading HRCT scans and for the radiologist to have as complete an understanding of the pathology of the ear as the otologist. With the advent of HRCT and multiplanar reconstructions, the understanding and quantification of preoperative changes of the mucosa, ossicles, and pneumatic cell systems within the middle ear cleft will provide a more scientific basis for surgical decisions. Classification of pathologic middle ear conditions (mucosal disease and ventilation dysfunction) based on imaging will lead to a more precise evaluation of surgical results and to a well-defined elimination of surgical attempts doomed to failure. As stated above, the global financial balance of otologic surgery will be less onerous and the outcome better in spite of the expense involved in using more precise imaging techniques. The scanner used was an MX8000 (Picker/Marconi, Cleveland, Ohio, US) with four detector rows. The examination protocol consisted of a 2.0 × 0.5-mm collimation with a high-resolution bone algorithm. The entire petrous bone was scanned from above the tegmen tympani to below the mastoid process with the patient’s head placed in a neutral position to approximate the Reid base line* (Figs. 142a–d). Fig. 142 The planes used in HRCT for the reconstruction of the temporal bone. The patient is a 40-year-old female with bilateral otosclerosis. a, b Planes used for axial scanning of the temporal bone from above the tegmen tympani to below the mastoid process. The head of the patient is in a neutral position approximating the Reid base line. c, d The planes for coronal scanning of the temporal bone are selected to contain the relevant structures of the external, middle, and inner ear. The printed films consisted of two sets of images, one film for each side with 20 images in the axial and coronal plane. The images of both planes were reconstructed from the raw data with a field of view (FOV) of 80 mm. Both planes have the same high-resolution quality due to isotropic voxel size. The images were photographed with a window width of 4000 HU and a window center of 1500 HU (Figs. 143a–d). Fig. 143 a Axial images of the right temporal bone. b Coronal images of the right temporal bone. c Axial images of the left temporal bone. d Coronal images of the left temporal bone. Many of the anatomic details of the middle and inner ear are not optimally displayed in conventional CT for several reasons: The limitations of conventional CT can only be overcome by dynamic multiplanar reconstruction at a designated workstation. Today, the otologist and radiologist are able to use PC-based programs to obtain quality multiplanar reconstructions (Dicom-3-Reader programs; e.g., eFilm for PC, Osirix for Mac users). The workstation we used was an Advantage Windows (General Electric, Fairfied, CT, US; http://www.ge.com). Generally, the otologist and radiologist work together to evaluate the HRCT images and should conventional CT not suffice for a correct diagnosis, both specialists can create supplementary slices at the workstation in order to obtain additional information about a specific problem and clearly show the pathology (Figs. 144a–c). Fig. 144 An open cavity with ossicular reconstruction (Fisch titanium total [FTT]) in the left ear of a 34-year-old male 3 years postoperative. a Conventional: coronal plane, oval window niche. Note the epitympanectomy with skeletonization of the middle cranial fossa (MCF) dura (1). The tympanic membrane (TM) (2) goes from the tympanic segment of the facial nerve to the inferior tympanic sulcus. The prosthesis head (3) is in full contact with the tympanic membrane. The prosthesis shaft cannot be seen on the stapes footplate (4). The 1-mm-thick Silastic sheeting (5) is barely visible over the promontory. b
General Considerations
Technical Aspects of High-Resolution Computed Tomography
HRCT (conventional)
 A Conventional CT
A Conventional CT
HRCT (conventional)
 B Multiplanar Reconstructions
B Multiplanar Reconstructions
 The axial and coronal planes are not always the best for all the anatomic structures. Therefore, it is very important to find the ideal plane for any desired anatomic detail using additional oblique slices.
The axial and coronal planes are not always the best for all the anatomic structures. Therefore, it is very important to find the ideal plane for any desired anatomic detail using additional oblique slices.
 In conventional CT with 20 images of the entire petrous bone there are always small gaps between the slices. Small anatomic structures are therefore not completely depicted and need an additional workup.
In conventional CT with 20 images of the entire petrous bone there are always small gaps between the slices. Small anatomic structures are therefore not completely depicted and need an additional workup.
 The standard window width and center is not ideal for very thin anatomic structures and should be handled dynamically.
The standard window width and center is not ideal for very thin anatomic structures and should be handled dynamically.
Conventional CT and multiplanar reconstruction
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


