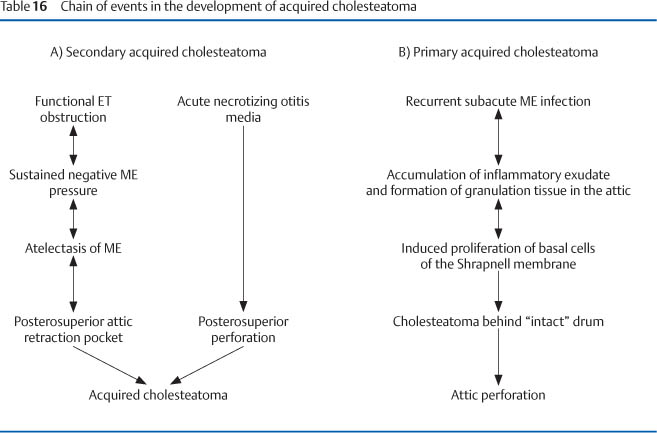
Chapter 5 Mastoidectomy and Epitympanectomy Disease involving the middle ear can extend to the mastoid and require surgical procedures involving this bone. Surgery limited to the mastoid is defined as cortical or simple mastoidectomy. A cortical mastoidectomy is mainly carried out in acute mastoiditis to drain infected mastoid air cells in association with myringotomy and introduction of a ventilating tube. Acute viral mastoiditis with inner ear involvement (vertigo and sensorineural hearing loss) requires mastoidectomy combined with epitympanotomy and posterior tympanotomy. This is necessary to achieve adequate drainage of the round and oval window niche, preventing permanent inner ear damage. In this chapter, mastoidectomy is mainly discussed in association with the treatment of middle ear disease (tympanomastoidectomy). The term intact canal wall or closed cavity tympanomastoidectomy is used when the posterosuperior canal wall is preserved. The term canal wall down or open mastoido-epitympanectomy implies removal of the posterosuperior canal wall and the complete exenteration and exteriorization of both mastoid and epitympanum. The most common indication for an open mastoido-epitympanectomy is chronic otitis media complicated by a cholesteatoma. Cholesteatoma is defined as the presence of keratinizing squamous epithelium within the middle ear or in other pneumatized areas of the temporal bone. The cholesteatoma may be classified as Congenital cholesteatoma is a developmental defect consisting of a cystic epidermoid growth arising from rests of keratinizing squamous epithelium present before birth. The patients have no history of ear disease and a normally pneumatized mastoid. For management of congenital cholesteatoma see Fisch and Mattox (1988, 2-R). Acquired cholesteatoma occurs after birth and is caused by invasion of the middle ear cleft by keratinizing squamous epithelium originating from the lining of the external auditory canal (EAC) or from the tympanic membrane (see Table 16). Patients with acquired cholesteatoma usually present with a history of recurrent ear disease and with a reduced pneumatization of the mastoid. According to the condition of the tympanic membrane, acquired cholesteatoma can be divided into primary and secondary. Primary acquired cholesteatomas develop behind an intact tympanic membrane. Secondary acquired cholesteatomas grow in the middle ear through a mostly marginal perforation of the tympanic membrane. Acquired cholesteatomas most commonly originate from a large posterosuperior perforation or from a small superior attic perforation. According to a study performed under F.R. Nager in the ENT Department, University Hospital, Zürich, Switzerland, before the antibiotic era, intracranial complications occurred in only 1.7% of cholesteatomas with extensive posterosuperior drum defects and in 6% of the cases with small attic perforations. Out of 763 cases of cholesteatomatous otitis media reviewed in 1934 by Nager, 631 cases presented with a large posterosuperior perforation. The middle ear suppuration started as a necrotizing otitis media of infancy in 35% of the cases. This arose in the course of scarlet fever, measles, diphtheria, tuberculosis, or influenza. In the remaining 65% of cholesteatomas with large perforations, no such history could be obtained. Since the middle ear infection dated from early childhood in the majority of cases, it was assumed that cholesteatomas with large perforations also begin in infancy as a necrotizing otitis media of unknown etiology. Only 20% of the 132 cases with a small attic perforation presented with a history of otitis media in early childhood. The ENT specialist did not observe in any of these cases the appearance of a small upper marginal perforation in the course of the acute otitis media. At the onset, the disease was usually symptomless and without an obvious association of a middle ear infection. A small perforation was often discovered accidentally in the course of a routine examination. There is no doubt today that in the presence of large posterosuperior perforations, as first described by Habermann in 1889 (Fig. 74), meatal epithelium grows inward through the perforation and, once in the middle ear, stimulates the production of a cholesteatoma (immigration theory). On the other hand, controversy still exists concerning the pathogenesis of the attic cholesteatomas. In 1957–1959 L. Rüedi (22–24-R) carried out an extensive histological and experimental study on the pathogenesis of cholesteatoma. He has shown that the pathogenesis of primary and secondary acquired attic cholesteatomas can best be explained on the basis of the immigration theory. Lange first put forward the opinion that a prolonged inflammatory stimulus may induce the proliferation of the basal cells in the epidermis of the Shrapnell membrane (Fig. 74). Rüedi opened the aural bulla in guinea pigs and introduced a mixture of talc and fibrin underneath the internal surface of the intact tympanic membrane. This caused a mild foreign body reaction, and in several animals granulation tissue developed between the drum and internal wall of the middle ear. Active ingrowth of the epidermis from the intact tympanic membrane into the newly formed granulation tissue was found to occur after 15 to 20 days. Invading colonies of basal cells divided into branches, and the desquamated stratified squamous epithelium formed typical cholesteatomatous masses. The clinical and histologic study of normal and pathologic animal experiments led Rüedi to the conclusion that, as a rule, all types of cholesteatoma of the middle ear develop by immigration of stratified squamous epithelium from the epidermis of the external auditory meatus or the tympanic membrane. Within the middle ear cavities, the active growth of the matrix is enhanced by submucous connective tissue filling the incompletely pneumatized attic and epitympanic cells. A search for evidence of embryonic cell rests or areas of metaplasia in the mucosa of the middle ear proved fruitless in 124 temporal bones obtained from patients with cholesteatoma, acute otitis media, and from normal young children examined histologically by serial section. While the occurrence of such cell rests or metaplasia is possible (Fig. 74), it is at best very rare; however, cholesteatomas are commonly encountered. Secondary acquired cholesteatomas are divided according to their origin into the following types. — Immigration cholesteatoma a) through a marginal perforation in chronic suppurative otitis media, b) after long standing and sufficiently drained retraction poclet of the drum in chronic serious otitis media or c) through papillary proliferation of basal cells after rupture of the limiting membrane of the epithelium of the Shrapnell’s membrane in chronic attic inflammation (see Figs. 74, 75) — Iatrogenic (keratinizing epithelium introduced in the middle ear cavity by a surgical procedure). — Residual (rests of keratinizing epithelium after incomplete surgical removal). — Recurrent (new secondary acquired cholesteatoma appearing following complete removal of a previous one). — Retention cholesteatoma (accumulation of keratin in an insufficiently exteriorized cavity). This latter type of cholesteatoma is not strictly confined to the middle ear (mucosal lined cavity) but can also develop within the insufficiently enlarged EAC. Fig. 74 Fig. 75 A primary acquired cholesteatoma may occur under an apparently intact tympanic membrane when the limiting membrane of the epithelium of the Shrapnell’s membrane is injured by a chronic infection with granulation tissue in the attic. The proliferating basal cells of the Shrapnell’s membrane penetrate into the granulation tissue through a hole in the limiting membrane without visible external perforation. The primary cholesteatoma differs from the congenital cholesteatoma because it is accompanied by a history of middle ear infection in a (mostly) sclerotic mastoid. Fig. 76 Secondary acquired cholesteatomas originate from a posterosuperior defect of the pars tensa or through a perforation in the Shrapnell’s membrane (see also Chapter 10, p. 332. They invade the attic, remaining lateral or medial to the malleus and incus. The medial route (broken line) leads through a triangular space situated between the chorda tympani, malleus neck, and long process of the incus. The lateral route (solid line) follows the lateral surface of the incus and malleus. In extensive lesions, lateral and medial routes of invasion are combined. — Eradication of disease. — Prevention of recurrent and retention cholesteatomas. — Formation of a dry and self-cleansing cavity. — Restoration of tympanic aeration. — Reconstruction of a sound-transformer mechanism. a) Closed (Intact Canal Wall) Tympanomastoidectomy The principle of the intact canal wall tympanomastoidectomy is to completely remove the cholesteatoma matrix with preservation of the external bony canal. The combined transcanal and transmastoid approach permits removal of cholesteatoma invading the facial recess. Cholesteatoma in the sinus tympani and eustachian tube may be difficult to extirpate because of the limited visibility in this areas. Fig. 77 The insert shows squamous epithelium (solid line) invading the middle ear cavity through a marginal perforation. Only a small remnant of mucosa (broken line) has remained under the anterior drum. The principle of a closed cavity (intact canal wall) mastoidectomy is to remove the matrix from the tympanic cavity and mastoid, working on both sides of the preserved bony canal wall (see also Chapter 10, p. 308). b) Open (Canal Wall Down) Mastoido-Epitympanectomy The principle of an open mastoido-epitympanectomy is to create a large cavity in which no retention of keratinizing epithelium is possible. The drawback of a classic radical mastoidectomy (open cavity without tympanoplasty) is the recurrent infection of the middle ear cavity through the perforated drum. Closure of the middle ear space by means of a tympanoplasty (modified radical mastoidectomy) eliminates the possible postoperative drainage from the middle ear, but insufficient attention is paid to elimination of disease from the attic. The open cavity surgical technique presented on the following pages is characterized by the radical exenteration and exteriorization of both mastoid and epitympanum (attic). The advantages of this technique, called open mastoido-epitympanectomy with tympanoplasty (OMET), are the elimination of recurrent and residual disease as well as the formation of a dry self-cleansing cavity. Fig. 78 The principle of a classic radical mastoidectomy is to include the external canal in a large open cavity. No tympanoplasty is performed (see also Chapter 10, p. 332). c) Temporary Resection of the Canal Wall Temporary resection of the canal wall allows additional exposure of the tympanomastoid space. The drawback is, however, the insufficient exteriorization and possible recurrence of disease (including cholesteatoma) in the presence of persisting eustachian tube dysfunction. The technique of temporary resection of the canal wall may also be called “open–closed” mastoidectomy. Fig. 79 a The broken line shows the planes of resection of the posterosuperior canal wall. The oblique margin adds stability when replacing the bone. b Removal of the posterosuperior canal wall lateral to the chorda tympani. c The reconstructed canal wall may be stabilized with bone removed from the temporal squama (see Figs. 55A–F), bone paste (bone dust and fibrin glue), as well as a drop of Histoacryl glue. The choice between open and closed tympanomastoidectomy depends on: — The function of the eustachian tube. — The extent of the disease. The pneumatization of the temporal bone (as determined by high-resolution computed tomography [HRCT], see Part 4, Chapter 10, pp. 299–300, 308, 332) is a good measure of the function of the eustachian tube. A sclerotic mastoid is generally the result of poor eustachian tube function (ventilation) during childhood. The criteria for the choice of the approach in mastoid surgery are: 1. Limited disease with good pneumatization: closed cavity. 2. Sclerotic mastoid with extensive disease: open cavity. 3. Disease, particularly cholesteatoma matrix, cannot be radically removed beyond doubt: open cavity. The consistent application of these rules has significantly reduced the number of intact canal wall procedures performed in our department from 73% (1970–1976) to 11% (1994–2000) (Table 17).
General Considerations
 Definitions
Definitions
 Cholesteatoma
Cholesteatoma
 Classification of Cholesteatoma
Classification of Cholesteatoma
 Congenital.
Congenital.
 Primary acquired.
Primary acquired.
 Secondary acquired.
Secondary acquired.
a) Congenital Cholesteatoma
b) Acquired Cholesteatoma
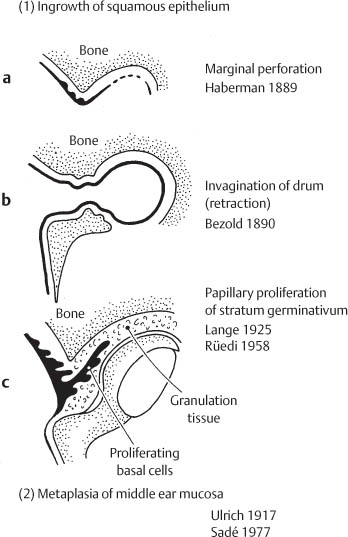
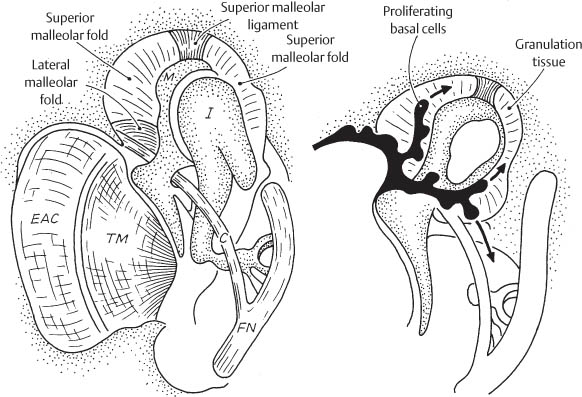
Pathogenesis of acquired cholesteatoma
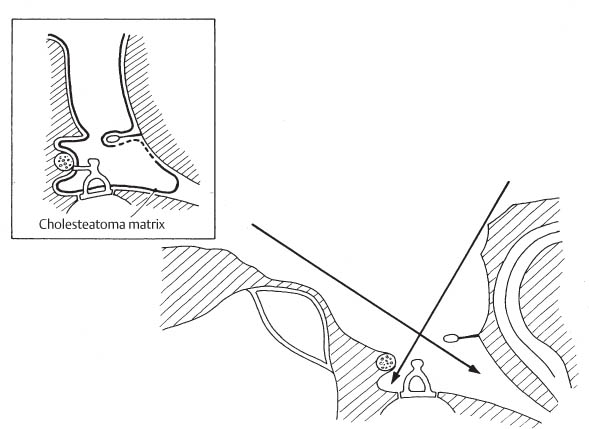
Routes of invasion of primary acquired cholesteatoma of the attic
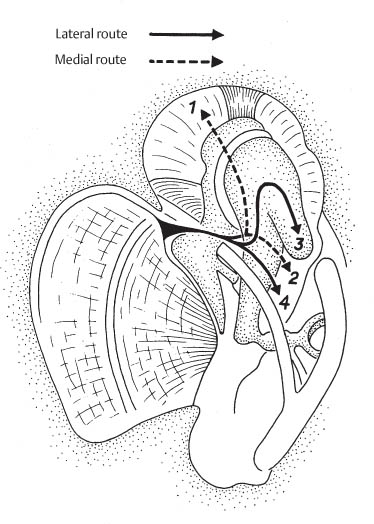
Routes of invasion of secondary acquired cholesteatoma of the attic
 Surgical Treatment of Acquired Cholesteatoma
Surgical Treatment of Acquired Cholesteatoma
Aims
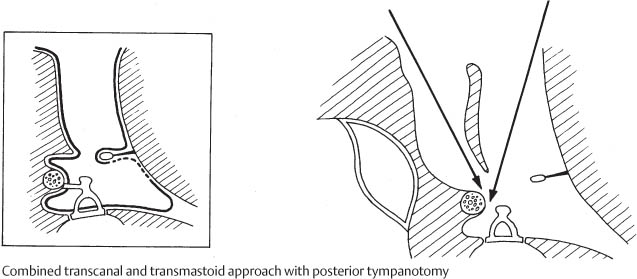
Surgical Concepts
Principle of closed (intact canal wall) tympanomastoidectomy
Principle of open cavity
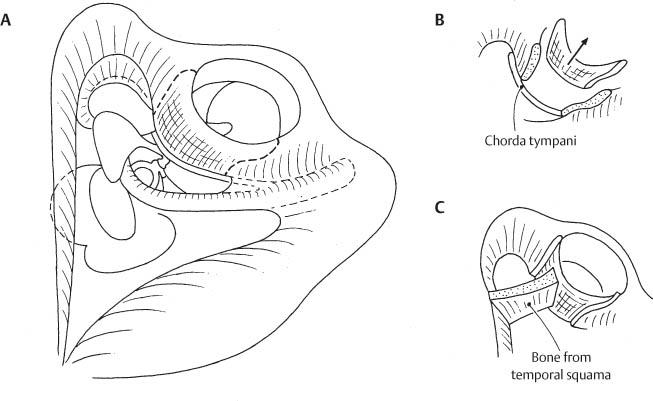
Temporary resection of the canal wall
| n | % |
Closed cavity | 225 | 73.0 |
Intact canal wall | 210 | 68.0 |
Temporary resection of canal wall | 15 | 5.0 |
Open cavity | 84 | 27.0 |
Modified radical mastoidectomy | 80 | 26.0 |
Radical mastoidectomy | 4 | 1.3 |
Specific Surgical Techniques for Cholesteatoma Removal
 Closed Mastoido-Epitympanotomy with Tympanoplasty
Closed Mastoido-Epitympanotomy with Tympanoplasty
Surgical Technique
The closed mastoido-epitympanotomy with tympanoplasty is a tympanomastoidectomy in which particular emphasis is applied to the work in the attic. A closed mastoido-epitympanotomy with tympanoplasty includes mastoidectomy, epitympanotomy, posterior tympanotomy, and tympanoplasty.
Surgical Highlights |
|
 General anesthesia
General anesthesia Retroauricular skin incision
Retroauricular skin incision Meatal skin flap
Meatal skin flap Canalplasty
Canalplasty Middle ear inspection
Middle ear inspection Mastoidectomy
Mastoidectomy Epitympanotomy
Epitympanotomy Posterior tympanotomy
Posterior tympanotomy Complete removal of cholesteatoma matrix
Complete removal of cholesteatoma matrix Tympanoplasty (ossiculoplasty, myringoplasty)
Tympanoplasty (ossiculoplasty, myringoplasty)Surgical Steps
The first surgical steps of intact canal mastoido-epitympanotomy with tympanoplasty are similar to those of retroauricular tympanoplasty:
— Retroauricular skin incision (Fig. 9A, p. 17).
— Raising of periosteal flap (Fig. 9B, p. 17).
— Canal incisions (Figs. 9C and D, pp. 17–18).
— Exposure of EAC and mastoid (Figs. 9E and F, p. 18).
— Elevation of meatal skin flap (Figs. 9G–N, pp. 19–22).
— Canalplasty (Figs. 9R–V, pp. 24–25).
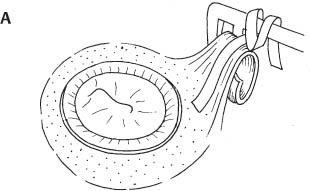
Fig. 80A
Surgical site after canalplasty
All bony overhang has been eliminated. The shape of the canal is that of an inverted truncated cone. A correct canalplasty facilitates tympanic membrane grafting, speeds up healing, ensures the self-cleansing property of the external canal, and makes it easier to carry out second-stage tympanoplasty (ossiculoplasty).
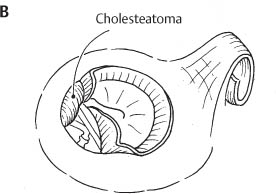
Fig. 80B
Middle ear inspection
The tympanomeatal flap is raised and the extent of cholesteatoma invasion of the middle ear assessed. The decision to perform a closed cavity is made on the basis of: (1) no evidence of eustachian tube dysfunction, (2) good pneumatization of the tympanomastoid cleft, and (3) limited extension of cholesteatoma.
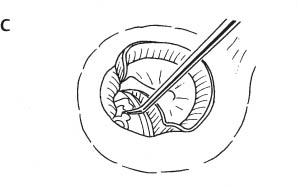
Fig. 80C
Division of the incudostapedial joint
This step is necessary to avoid inducing a sensorineural hearing loss when working along the incus and malleus in the attic. In most instances, the long process of the incus is already eroded by the cholesteatoma so that division of the incudostapedial joint is superfluous.
Mastoidectomy
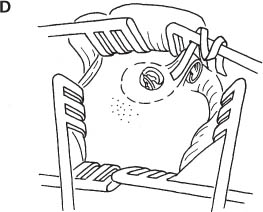
Fig. 80D
Mastoidectomy: exposure of the mastoid plane
The mastoid plane is exposed with two articulated re-tractors (3-I) supplemented by a third rigid retractor (2-I) placed between the temporal muscle and mastoid tip.
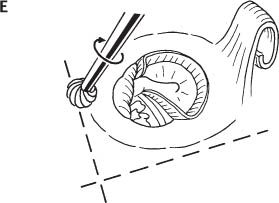
Fig. 80E
Mastoidectomy: identification of the antrum
The antrum is identified at the intersection of two grooves formed by removing bone along the superior and posterior canal wall. The entrance of the bony external canal should not be lowered when drilled for the antrum (see Fig. 80F). This is why the canalplasty should be completed before looking for the antrum. The middle fossa dura and sigmoid sinus are skeletonized at this stage when working in a sclerotic mastoid.
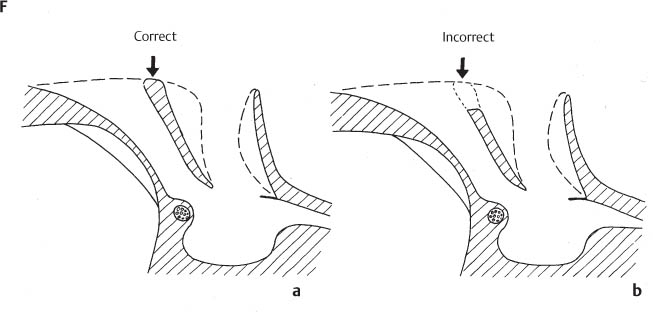
Fig. 80F
Mastoidectomy: correct bone removal
a The posterior canal wall should not be lowered during canalplasty and mastoidectomy.
b Lowering the posterior entrance of the canal carries the risk of squamous epithelium ingrowth from the external canal into the mastoid (meatomastoid fistula).
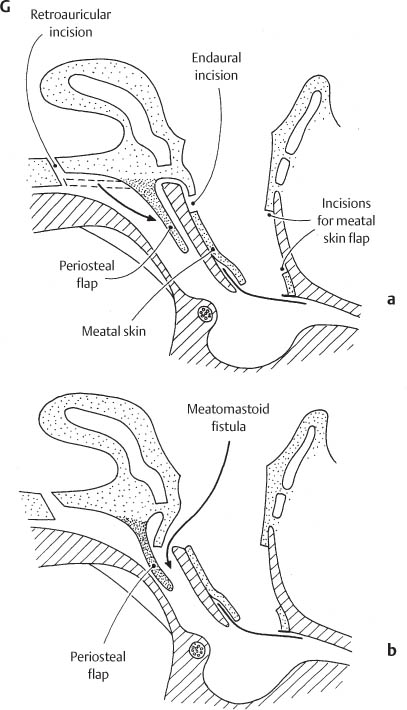
Fig. 80G
Mastoidectomy (cont.): danger of incorrect bone removal
Schematic cross section through the ear showing the correct (a) and incorrect (b) shaping of the posterior canal wall. Note that the posterior limb of the endaural incision must be made lower than the lateral entrance of the external canal and how the mastoid periosteal flap is rotated against the posterior canal wall to prevent atrophy of the bone and a meatomastoid fistula.
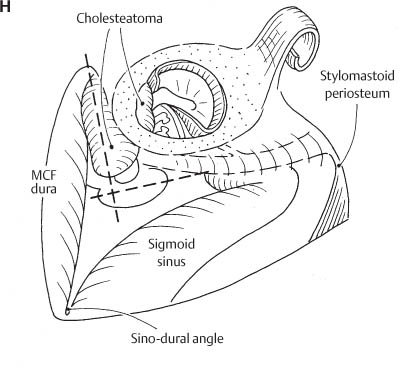
Fig. 80H
Surgical site after mastoidectomy
The broken lines show the position of the antrum. The digastric ridge and the stylomastoid periosteum are exposed to identify the stylomastoid foramen. The course of the mastoid segment of the fallopian canal is identified through the bone using the monitoring of the EMG of facial muscles (NIM-2). The retrofacial cells are exenterated. The lateral and posterior semicircular canals are identified and the retrolabyrinthine cells exenterated. The sigmoid sinus and the middle cranial fossa dura are skeletonized.
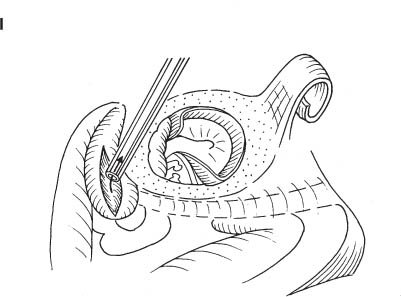
Fig. 80I
Epitympanectomy: exposure of the attic
The lateral wall of the attic is removed with a diamond burr. The cholesteatoma fills the epitympanum. The matrix is opened with small tympanoplasty microscissors (52-I), and the contents of the cholesteatoma sac are evacuated by suction. The size of the cholesteatoma is reduced to allow easier separation of the matrix from the surrounding bone. Opening of the cholesteatoma sac permits evaluation of the condition of the lateral semicircular canal through the medial wall of the matrix. Changes in color (dark blue) indicate the presence of a fistula.
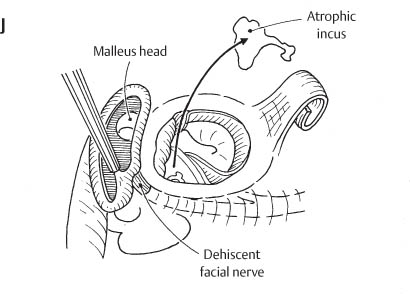
Fig. 80J
Epitympanectomy: identification of the tympanic facial nerve
The atrophic incus is removed. The cholesteatoma matrix is elevated from the lateral semicircular canal if no fistula is suspected. The tympanic facial nerve is identified along the inferior margin of the lateral semicircular canal. Only on rare occasions does an extremely large cholesteatoma prevent adequate identification of the facial nerve along the lateral semicircular canal. In such a situation, it is best to follow the mastoid facial nerve from the stylomastoid foramen into the area where the anatomy has been distorted by the lesion. EMG monitoring of facial function (NIM-2) is essential in such a situation (see Fig. 2).
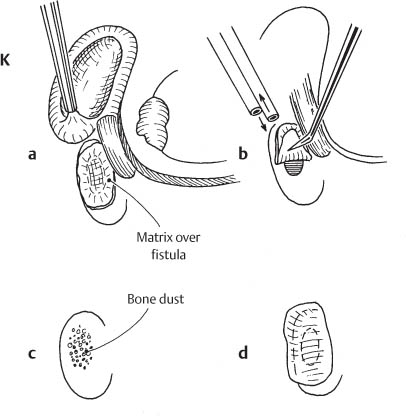
Fig. 80K
Management of semicircular canal fistula
a Always expect a fistula when elevating the cholesteatoma matrix from the lateral semicircular canal. Look for a fistula before removing the medial wall of the cholesteatoma sac. A fistula is suspected when a circumscribed dark color is seen along the semicircular canals. In the presence of a fistula, leave the covering skin until the end of the operation to avoid damaging the inner ear.
b Remove the skin over the fistula when the bone work and the removal of the remaining matrix is completed. Use constant irrigation. The matrix covering the fistula is only removed if the endosteum is intact. This is usually possible in fistulas up to 2 mm in diameter. If the perilymphatic space is open, the skin covering the fistula is replaced in its original position (see also Figs. 178, 179).
c If the matrix has been removed, the intact endosteum of the fistula is covered with bone dust (obtained by drilling) mixed with fibrin glue (bone paste).
d The fistula is finally covered with fresh temporal fascia placed over the bone paste.
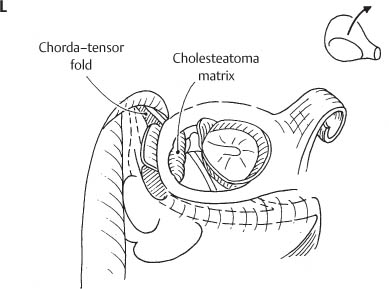
Fig. 80L
Epitympanectomy (cont.): exenteration of the attic
The malleus neck is divided and the head of the malleus removed. The cholesteatoma matrix is carefully detached from the walls of the epitympanum, and the size of the cholesteatoma sac is successively reduced by cutting away excess matrix. The completely closed chorda–tensor fold is removed. The matrix lying lateral to the tympanic segment of the facial nerve is removed from the supralabyrinthine and supratubal recess. The position of the geniculum, petrosal nerve, and labyrinthine segment of the facial nerve should be known to avoid injury of a dehiscent nerve. A spontaneous dehiscence of the facial nerve may exist proximal to the geniculum. EMG monitoring of the facial muscles with the NIM-2 is very helpful in this phase of surgery to avoid causing a lesion of the facial nerve.
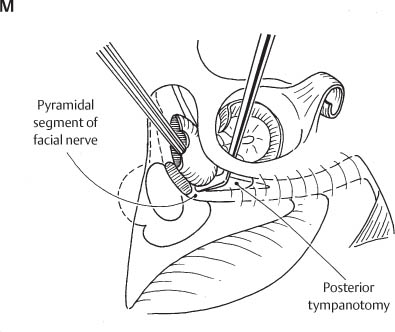
Fig. 80M
Posterior tympanotomy
The bone situated between the pyramidal facial nerve and the chorda tympani is drilled away along the tympanic segment of the fallopian canal. The resulting opening to the middle ear is the posterior tympanotomy. A lesion of the facial nerve should not occur because the posterior tympanotomy is carried out after the mastoid segment of the fallopian canal has been skeletonized. This is done in a retrograde fashion beginning from the stylomastoid foramen (see Fig. 80H). The posterior tympanotomy is performed under direct visual control of the nerve and with EMG monitoring of the facial muscles (NIM-2). The size of the tympanotomy depends on the extent of the cholesteatoma in the facial recess and sinus tympani. A wide exposure of the sinus tympani requires sacrifice of the chorda. If the cholesteatoma is limited to the superior half of the oval window niche (above the stapes arch), complete removal of the matrix can be accomplished at this stage, working from both sides of the intact canal wall (combined approach).
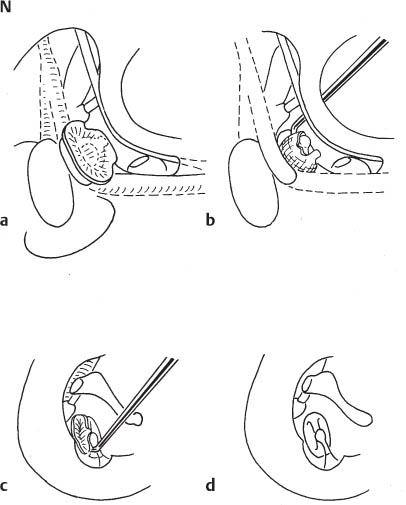
Fig. 80N
Posterior tympanotomy: removal of cholesteatoma from the oval window
Matrix covering the stapes and oval window is removed after completion of all bone work because uncontrolled suction irrigation might damage the exposed inner ear.
a The last portion of cholesteatoma invading the oval window niche between the stapes arch and facial nerve is exposed.
b Removal of the matrix from the oval window begins anteriorly where the footplate (or membrane covering the oval window) is best identified. For the elevation of matrix from the oval window, the same precautions should be taken as when working over a fistula of the lateral semicircular canal (see Fig. 80K, p. 165).
c The posterior matrix is best removed through the transcanal approach. Drilling a small notch in the posterior canal wall may be necessary to visualize the posterior foot-plate. Removal of the matrix from the stapes is performed in a posteroanterior direction, taking advantage of the stability offered by the stapedial tendon.
d The matrix has been completely removed from the oval window niche and stapes. The notch in the posterior canal wall will be reconstructed later on with tragal cartilage. Cutting the stapes arch with crurotomy scissors (54-I, 55-I) to remove matrix surrounding the stapes arch is rarely necessary. Manipulations around the stapes arch require caution to avoid luxation of the foot-plate.
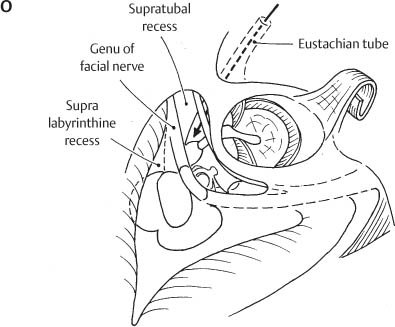
Fig. 80O
Surgical site following completion of closed tympanomastoidectomy
The supralabyrinthine and supratubal recesses are exenterated. Good knowledge of the anatomy of the tympanic and labyrinthine segment of the facial nerve is necessary for this purpose. Keep in mind the acute angle formed by the tympanic and labyrinthine facial nerve and that the proximal labyrinthine segment of the fallopian canal is nearly covered by the lateral tympanic segment. Note that the chorda–tensor fold was removed to provide adequate ventilation of the anterior attic (arrow).
Fig. 80P
Tympanoplasty (ossiculoplasty)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


