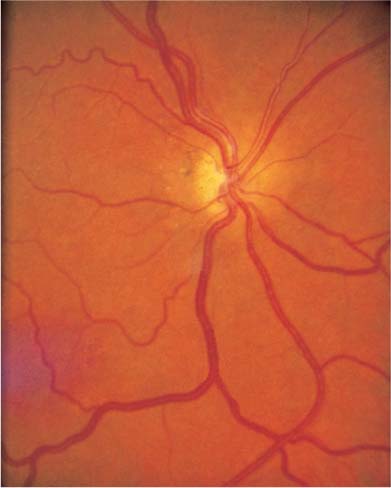
Chapter 23 Congenital optic nerve anomalies are associated with variable visual system function; affected individuals may be asymptomatic throughout life or develop signs of severe visual deficiency in infancy. Thus, anomalies may be discovered incidentally, during evaluation for poor vision and nystagmus in infants, or in adults with recent visual loss. They may be associated with both central nervous system and systemic abnormalities. Clinically, it is useful to characterize the anomalies by the appearance of the optic disc and peripapillary retina and to separate them into three general categories: (1) abnormalities of disc size, (2) abnormalities of disc conformation, and (3) presence of abnormal tissue at the disc. Optic nerve aplasia is an extremely rare, nonhereditary syndrome of unknown etiology, characterized by complete lack of development of the optic nerve, disc, retinal nerve fiber layer, ganglion cells, and retinal vasculature. Optic nerve aplasia does not require urgent evaluation. No visual function is present in the affected eye (s). Ocular The eye is microphthalmic or small. Optic nerve aplasia is usually associated with cataract, anterior chamber angle malformation, retinal dysplasia, anterior coloboma, iris hypoplasia, or persistent primary vitreous. Systemic Although unilaterally affected individuals are usually otherwise healthy, bilaterally affected individuals typically have severe central nervous system malformations and die shortly after birth. None Children at risk for amblyopia should be seen within 1 or 2 weeks. Optic nerve hypoplasia is the most commonly encountered congenital optic disc anomaly. It is usually bilateral. Optic nerve hypoplasia has been associated with several environmental factors including maternal insulin-dependent diabetes mellitus, fetal alcohol syndrome, maternal ingestion of quinine, anticonvulsants, and illicit drugs. Visual function can range from normal to absent in the affected eye (s). Visual Function Visual function can vary from 20/20 to no light perception and is nonprogressive. Presumably, the variability is directly related to the number of axons present. Disc The hypoplastic disc is small in diameter (histopathology shows subnormal numbers of axons), often pale, and surrounded by a yellowish halo bordered by a ring of pigmentation (double-ring sign) (Fig. 23–1). The yellowish halo may be mistaken for optic nerve pallor, resulting in misdiagnosis of optic atrophy. Major retinal blood vessels may be tortuous and have anomalous branching patterns. Rarely, variants of optic nerve hypoplasia occur where the disc is not diffusely small. Superior segmental disc hypoplasia can occur in children of insulin-dependent diabetic mothers. These discs have superior entrance of the central retinal artery, superior disc pallor, superior peripapillary halo, and inferior visual field loss. In utero damage to the afferent visual system can result in segmental optic disc hypoplasia corresponding to the portion of optic nerve affected. In utero retrogeniculate lesions can produce disc changes (homonymous hemioptic hypoplasia), presumably by transsynaptic degeneration. Other Ocular Optic nerve hypoplasia may occur without other ocular abnormalities, although astigmatism is commonly associated. There may be superimposed amblyopia; an occlusion trial should be instituted if it is suspected. Systemic Optic nerve hypoplasia is frequently associated with a variety of central nervous system and endocrine abnormalities. Septo-optic dysplasia (de Morsier syndrome) consists of absence of the septum pellucidum, agenesis of the corpus callosum, and optic nerve hypoplasia. These patients may have deficiencies of anterior pituitary hormones leading to dwarfism, hypothyroidism, diabetes insipidus, hypocortisolemia, and hyperprolactinemia. Hormonal insufficiency may progress over time, and repeat evaluation is necessary. Other common central nervous system structural abnormalities, including hemispheric migration anomalies, encephalomalacia, and posterior pituitary ectopia, may have prognostic implications. Brodsky and Glaser1 found that posterior pituitary ectopia predicts anterior pituitary hormone deficiency in patients with optic nerve hypoplasia. They also reported a correlation between the presence of cerebral hemispheric abnormalities and neurodevelopmental deficits. FIGURE 23–1 Optic nerve hypoplasia. Magnetic resonance imaging (MRI) should be obtained to evaluate structural abnormalities. Occlusion therapy to prevent amblyopia, when necessary. Children found to have optic nerve hypoplasia need careful refraction, MRI, and endocrine evaluation. Megalopapilla does not require urgent evaluation. Patients are asymptomatic. Visual Function Optic nerve function is normal. Disc Megalopapilla is present when the disc is greater than 2.1 mm in diameter and is otherwise normal in configuration except for an increased cup-to-disc ratio. The cupping is symmetric horizontally and vertically without focal notching of the rim. It is usually bilateral, and cilioretinal arteries are often present. No treatment is necessary. Megalopapilla probably represents a physiologic variant of normal, but patients with the anomaly are occasionally inappropriately diagnosed with glaucoma and treated. Rarely anterior encephalocele, and midline facial anomalies may be associated, but in the absence of optic nerve dysfunction or these findings, no further evaluation is necessary. Tilted discs do not require urgent evaluation unless there are symptoms of peripheral field loss, progressive visual field changes, or strict respect of the vertical midline (see below). Patients with tilted discs are usually asymptomatic, though superior bitemporal visual field defects may be present. Visual Fields Superior bitemporal visual field abnormalities are due to refractive scotomas produced by the regional myopia from the inferonasal retina. They do not respect the vertical midline. Fundus The tilted disc syndrome is characterized by elevation of the superotemporal disc, posterior displacement of the inferonasal disc, situs inversus of the retinal vessels, inferonasal conus, and thinning of the inferonasal retinal pigmented epithelium and choroid (Fig. 23–2). These findings are bilateral in 80%. In some cases, the optic discs are focally hypoplastic, with corresponding visual defects that do not respect the midline. MRI should be performed if atypical (see Red Flags, above). None See Red Flags, above. Within several weeks, because amblyopia may occur and may be treatable in milder cases. Morning glory discs are usually unilateral, occur more commonly in females, and are rare in African Americans.
CONGENITAL OPTIC NERVE ANOMALIES
ANOMALIES CHARACTERIZED BY ABNORMALITY OF OPTIC DISC SIZE
OPTIC NERVE APLASIA
Urgency of Evaluation
Diagnosis
Symptoms
Signs
Treatment
OPTIC NERVE HYPOPLASIA
Urgency of Evaluation
Diagnosis
Demographics
Symptoms
Signs
Ancillary Tests
Treatment
Follow-up and Referral
MEGALOPAPILLA
Urgency of Evaluation
Diagnosis
Symptoms
Signs
Treatment
Follow-up and Referral
ANOMALIES CHARACTERIZED BY ABNORMALITIES OF OPTIC DISC CONFORMATION
TILTED DISCS
Urgency of Evaluation
Diagnosis
Symptoms
Signs
Red Flag
 True bitemporal visual field defects due to suprasellar lesions have been reported in patients with tilted discs. Thus, in a patient with the tilted disc syndrome, not all field defects should be ascribed to the congenital disc anomaly; symptoms of peripheral field loss, progressive visual field changes, or strict respect of the vertical midline should prompt neuroimaging.
True bitemporal visual field defects due to suprasellar lesions have been reported in patients with tilted discs. Thus, in a patient with the tilted disc syndrome, not all field defects should be ascribed to the congenital disc anomaly; symptoms of peripheral field loss, progressive visual field changes, or strict respect of the vertical midline should prompt neuroimaging.
Ancillary Tests
Treatment
Follow-up and Referral
MORNING GLORY DISC
Urgency of Evaluation
Diagnosis
Demographics
Symptoms
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


