2
Congenital Corneal Opacity
Bruce Schnall and Michael J. Bartiss 
The differential diagnosis for congenital corneal opacity can be remembered using the pneumonic STUMPED:
Sclerocornea
Tears in Descemet’s membrane or birth trauma
Ulcer or infection
Mucopolysaccharidosis (MPS)
Peters’ anomaly
Endothelial dystrophy, congenital hereditary (CHED)
Dermoid
SCLEROCORNEA
Etiology
 Developmental anomaly of the cornea
Developmental anomaly of the cornea
 Defective mesodermal migration during embryogenesis, resulting in tissue resembling sclera rather than clear corneal stroma
Defective mesodermal migration during embryogenesis, resulting in tissue resembling sclera rather than clear corneal stroma
 Can be autosomal dominant, recessive, or sporadic
Can be autosomal dominant, recessive, or sporadic
 Has been associated with the 22q11.2 deletion syndrome
Has been associated with the 22q11.2 deletion syndrome
Symptoms
 Opacified cornea present since birth
Opacified cornea present since birth
Signs
 Usually bilateral but can be unilateral
Usually bilateral but can be unilateral
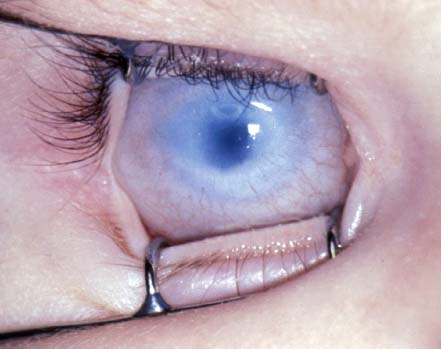
 Opacification of the cornea with the peripheral cornea more opacified than the central cornea (Fig. 2-1)
Opacification of the cornea with the peripheral cornea more opacified than the central cornea (Fig. 2-1)
 May have fine blood vessels
May have fine blood vessels
Differential Diagnosis
 Tears in Descemet’s membrane or birth trauma
Tears in Descemet’s membrane or birth trauma
 Ulcer or infection
Ulcer or infection
 MPS
MPS
 Peters’ anomaly
Peters’ anomaly
 CHED
CHED
 Dermoid
Dermoid
 Glaucoma
Glaucoma
Treatment
 Evaluation by a genetic specialist to look for associated congenital anomalies
Evaluation by a genetic specialist to look for associated congenital anomalies
 If the central cornea is clear, it can be associated with cornea plano and a high refractive error.
If the central cornea is clear, it can be associated with cornea plano and a high refractive error.
 Penetrating keratoplasty should be considered if the central visual axis is involved and the posterior segment is relatively normal.
Penetrating keratoplasty should be considered if the central visual axis is involved and the posterior segment is relatively normal.
Prognosis
 Visual outcome with or without keratoplasty depends on the presence of other ocular and systemic abnormalities.
Visual outcome with or without keratoplasty depends on the presence of other ocular and systemic abnormalities.
REFERENCES
Binenbaum G, McDonald-McGinn DM, Zackai EH, et al. Sclerocornea associated with the chromosome 22q11.2 deletion syndrome. Am J Med Genet A. 2008;146(7):904–909.
Doane JF, Sajjadi H, Richardson WP. Bilateral penetrating keratoplasty for sclerocornea in an infant with monosomy 21. Case report and review of the literature. Cornea. 1994;13(5):454–458.
Kim T, Cohen EJ, Schnall BM, et al. Ultrasound biomicroscopy and histopathology of sclerocornea. Cornea. 1998;17(4):443–445.
FIGURE 2-1. Descemet’s membrane: sclerocornea. The corneal opacification is more severe peripherally than centrally.
BIRTH TRAUMA: TEARS IN DESCEMET’S MEMBRANE
Etiology
 Trauma to the cornea during vaginal delivery resulting in tears in Descemet’s membrane
Trauma to the cornea during vaginal delivery resulting in tears in Descemet’s membrane
 May be associated with the use of forceps
May be associated with the use of forceps
Symptoms
 Corneal edema or opacification present at birth, which may resolve within the first few days of life
Corneal edema or opacification present at birth, which may resolve within the first few days of life
Signs
 Unilateral corneal edema or opacification present at birth (Fig. 2-2A)
Unilateral corneal edema or opacification present at birth (Fig. 2-2A)
 Often observed to have eyelid swelling and evidence of trauma to eyelids at birth
Often observed to have eyelid swelling and evidence of trauma to eyelids at birth
 Corneal edema often resolves within the first few days of life, revealing the Descemet’s membrane ruptures, which usually appear as vertical linear tears (Fig. 2-2B and C). Descemet’s tears associated with congenital glaucoma are usually oriented horizontally or curvilinearly (Fig. 2-3).
Corneal edema often resolves within the first few days of life, revealing the Descemet’s membrane ruptures, which usually appear as vertical linear tears (Fig. 2-2B and C). Descemet’s tears associated with congenital glaucoma are usually oriented horizontally or curvilinearly (Fig. 2-3).
 Multiple tears are often present.
Multiple tears are often present.
 Associated with high astigmatism
Associated with high astigmatism
Differential Diagnosis
 Sclerocornea
Sclerocornea
 Ulcer or infection
Ulcer or infection
 MPS
MPS
 Peters’ anomaly
Peters’ anomaly
 CHED
CHED
 Dermoid
Dermoid
 Glaucoma
Glaucoma
Treatment
 Descemet’s tears are associated with high astigmatism, which is amblyogenic. Treatment of the amblyopia includes correction of the refractive error with glasses or contacts and part-time occlusion of the fellow eye.
Descemet’s tears are associated with high astigmatism, which is amblyogenic. Treatment of the amblyopia includes correction of the refractive error with glasses or contacts and part-time occlusion of the fellow eye.
 Penetrating keratoplasty should be considered if the corneal edema does not resolve.
Penetrating keratoplasty should be considered if the corneal edema does not resolve.
Prognosis
 Visual outcome depends on the success of amblyopia treatment.
Visual outcome depends on the success of amblyopia treatment.
REFERENCE
Lambert SR, Drack AV, Hutchinson AK. Longitudinal changes in the refractive errors of children with tears in Descemet’s membrane following forceps injuries. J AAPOS. 2004;8(4):368–370.
FIGURE 2-2. A. Corneal opacification in a newborn from Descemet’s tears associated with birth trauma. B. The vertically oriented linear Descemet’s membrane ruptures can now be seen in the same infant a few days later after the corneal edema has cleared. C. The vertically oriented Descemet’s membrane breaks from birth trauma can be seen in this older child at the slit lamp with retroillumination.

FIGURE 2-3. A. Recent Descemet’s membrane ruptures associated with glaucoma. Note that the breaks are oriented horizontally. They are recent and therefore have overlying corneal edema. B. Breaks in Descemet’s membranes caused by glaucoma. The horizontally oriented breaks can be seen more clearly after resolution of the corneal edema.

ULCER OR INFECTION
Etiology
 Acquired bacterial or herpetic infection
Acquired bacterial or herpetic infection
Symptoms
 Acquired corneal opacity usually associated with conjunctival injection and eyelid swelling (Fig. 2-4)
Acquired corneal opacity usually associated with conjunctival injection and eyelid swelling (Fig. 2-4)
Signs
 Usually unilateral
Usually unilateral
 Corneal opacity with overlying epithelial defect
Corneal opacity with overlying epithelial defect
 Associated with conjunctival injection and other signs of inflammation
Associated with conjunctival injection and other signs of inflammation
 May have associated systemic infection
May have associated systemic infection
 May have associated eyelid lesions or eyelid abnormalities
May have associated eyelid lesions or eyelid abnormalities
Differential Diagnosis
 Sclerocornea
Sclerocornea
 Tears in Descemet’s membrane or birth trauma
Tears in Descemet’s membrane or birth trauma
 MPS
MPS
 Peters’ anomaly
Peters’ anomaly
 CHED
CHED
 Dermoid
Dermoid
 Glaucoma
Glaucoma
Treatment
 Depends on underlying cause or organism
Depends on underlying cause or organism
 Prompt systemic treatment may be needed
Prompt systemic treatment may be needed
Prognosis
 May result in a visually significant corneal scar
May result in a visually significant corneal scar
REFERENCE
Luchs JI, Laibson PR, Stefanyszyn MA, et al. Infantile ulcerative keratitis secondary to congenital entropion. Cornea. 1997;16:1:32–34.
FIGURE 2-4. Corneal ulcer in an infant caused by congenital entropion of the lower eyelid.

MUCOPOLYSACCHARIDOSIS
Etiology
 Inborn error of metabolism
Inborn error of metabolism
 Enzyme deficiency leads to a block in a metabolic pathway, which results in accumulation of material in the cornea.
Enzyme deficiency leads to a block in a metabolic pathway, which results in accumulation of material in the cornea.
Symptoms
 Acquired opacification of the cornea:
Acquired opacification of the cornea:
 Hurler’s syndrome, or MPS 1H, is associated with corneal clouding by 6 months of age
Hurler’s syndrome, or MPS 1H, is associated with corneal clouding by 6 months of age
 Scheie’s syndrome, or MPS 1S, is associated with corneal clouding by 12 to 24 months of age
Scheie’s syndrome, or MPS 1S, is associated with corneal clouding by 12 to 24 months of age
Signs
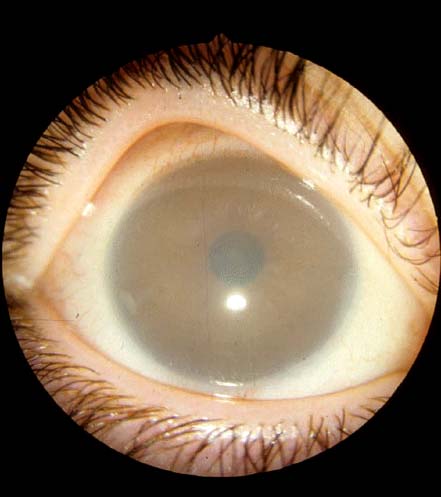
 Acquired corneal cloudiness or haze (Fig. 2-5)
Acquired corneal cloudiness or haze (Fig. 2-5)
 Associated systemic features (coarse facial features, mental retardation, poor growth, deafness)
Associated systemic features (coarse facial features, mental retardation, poor growth, deafness)
Differential Diagnosis
 Sclerocornea
Sclerocornea
 Tears in Descemet’s membrane or birth trauma
Tears in Descemet’s membrane or birth trauma
 Ulcer or infection
Ulcer or infection
 Peters’ anomaly
Peters’ anomaly
 CHED
CHED
 Dermoid
Dermoid
 Glaucoma
Glaucoma
Diagnosis
 Evaluation by a genetic specialist
Evaluation by a genetic specialist
 Urine testing for MPS
Urine testing for MPS
 Enzyme assay
Enzyme assay
 Gene testing for gene defect
Gene testing for gene defect
Treatment
 Enzyme replacement
Enzyme replacement
 Bone marrow transplant
Bone marrow transplant
Prognosis
 Depends on severity of systemic disease and success of systemic treatment
Depends on severity of systemic disease and success of systemic treatment
REFERENCE
Kenyon KR, Navon SE, Haritoglou C. In: Krachmer JH, Mannis MJ, Hollane EJ, eds. Cornea. 2nd ed. Vol 1. Philadelphia: Elsevier Mosby; 2005:749–776.
FIGURE 2-5. Hurler’s syndrome. Note the generalized corneal haze. (Courtesy of Alex Levin, MD.)
PETERS’ ANOMALY
Etiology
 Congenital
Congenital
 Can be autosomal dominant, recessive, or sporadic
Can be autosomal dominant, recessive, or sporadic
 May be associated with mutation of the PAX6 gene
May be associated with mutation of the PAX6 gene
Symptoms
 Central corneal opacity present at birth (Fig. 2-6)
Central corneal opacity present at birth (Fig. 2-6)
 80% are bilateral.
80% are bilateral.
Signs
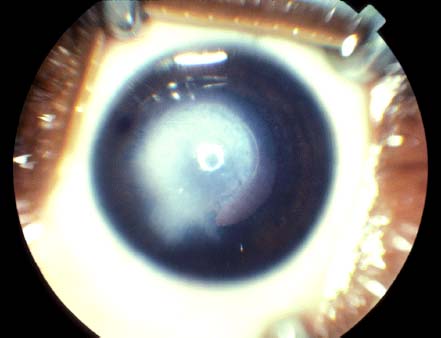
 Central corneal leukoma with adherent iris strands (Fig. 2-7)
Central corneal leukoma with adherent iris strands (Fig. 2-7)
 Adherent iris strands usually originate from the iris collarette to the posterior surface of the corneal leukoma.
Adherent iris strands usually originate from the iris collarette to the posterior surface of the corneal leukoma.
 May have associated cataract and glaucoma
May have associated cataract and glaucoma
Differential Diagnosis
 Sclerocornea
Sclerocornea
 Tears in Descemet’s membrane or birth trauma
Tears in Descemet’s membrane or birth trauma
 Ulcer or infection
Ulcer or infection
 MPS
MPS
 CHED
CHED
 Dermoid
Dermoid
 Glaucoma
Glaucoma
Diagnosis
 Examination under anesthesia may be needed to confirm diagnosis and rule out glaucoma.
Examination under anesthesia may be needed to confirm diagnosis and rule out glaucoma.
Treatment
 Evaluation by a genetic specialist to look for associated anomalies and to rule out Peters’ plus syndrome
Evaluation by a genetic specialist to look for associated anomalies and to rule out Peters’ plus syndrome
 Treat glaucoma if present.
Treat glaucoma if present.
 Penetrating keratoplasty should be considered within the first few months of life if the central visual axis is involved and posterior segment is relatively normal.
Penetrating keratoplasty should be considered within the first few months of life if the central visual axis is involved and posterior segment is relatively normal.
 If a visually significant cataract is present, cataract removal may be needed.
If a visually significant cataract is present, cataract removal may be needed.
Prognosis
 Depends on involvement of the anterior segment; prognosis is poorer if a cataract or glaucoma is present
Depends on involvement of the anterior segment; prognosis is poorer if a cataract or glaucoma is present
 Depends on success of amblyopia treatment
Depends on success of amblyopia treatment
 Early keratoplasty may reduce amblyopia.
Early keratoplasty may reduce amblyopia.
REFERENCES
Mailette De Buy Wenniger-Prick LJ, Hennekam RC. The Peters’ plus syndrome: a review. Ann Genet. 2002;45(2):97–103.
Yang LL, Lambert SR, Drews-Botsch C, et al. Long-term visual outcome of penetrating keratoplasty in infants and children with Peters anomaly. J AAPOS. 2009;13(2):175–180.
Yang LL, Lambert SR, Lynn MJ, et al. Long-term results of corneal graft survival in infants and children with Peters anomaly. Ophthalmology. 1999;106(4):833–848.
FIGURE 2-6. Peters’ anomaly. Note the central opacity and the clear corneal periphery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


