Correction of auricular malformations requires a comprehensive knowledge base of the existing surgical procedures. Surgery, without the knowledge in selecting the proper technique, will cause great harm. As with any surgical operation, successful outcome depends foremost on the surgeon’s experience and meticulous attention to detail in both planning and execution. In addition, the plastic surgeon should realize that the care of the patient with an ear deformity may necessitate a team approach that includes an otologist, audiologist, radiologist, and psychiatrist. The family should be an integral part of the surgical planning at the outset. This chapter covers ear deformities ranging from simple protruding ears to major congenital deformities.
ANATOMY AND EMBRYOLOGY
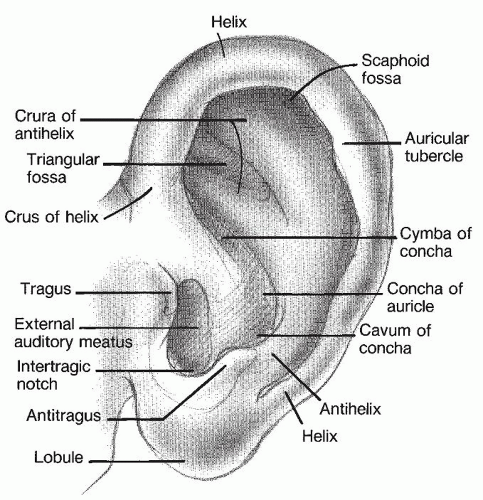
Topographic landmarks in a normal ear are shown in
Figure 191.1. Of particular importance are the helix, superior crus, inferior crus, scapha, and antihelix as well as the cymba conchae and the cavum conchae, the two structures that make up the entire conchal bowl.
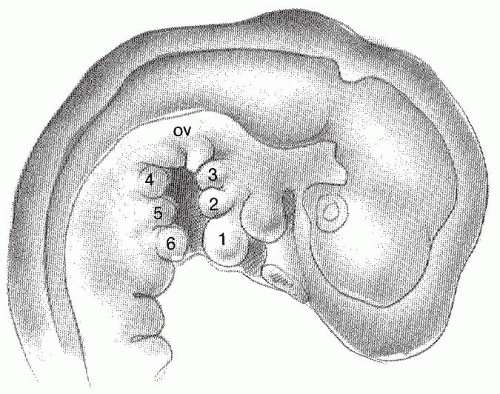
The development of the auricle is first seen in the 5-week-old embryo. The auricle begins as six mesenchymal proliferations at the dorsal ends of the first and second pharyngeal arches surrounding the first pharyngeal cleft. Initially, the external ear is located in the lower neck. As the mandible develops, the ear ascends to the side of the head at the level of the eyes. The current theory behind auricular development (
Fig. 191.2) is that the six hillocks correlate directly with the tragus, helix, cymbum, scapha, antihelix, and antitragus (
1).
The ear is made of both intrinsic and extrinsic musculature. The intrinsic muscles are the major and minor helixes, the tragus, the antitragus, the transverse, and the oblique. The extrinsic muscles include the anterior auricularis, superior auricularis, and posterior auricularis.
The auricle receives its blood supply from three arteries: the superficial temporal, the posterior auricular, and the occipital. The venous system involves the posterior auricular, external jugular, superficial temporal, and retromandibular veins. The lymphatic system of the ear drains anteriorly to the parotid lymph nodes and posteriorly to the cervical lymph nodes. Cranial nerve VII supplies the motor innervation of the auricle, with the temporal branch supplying the anterior and superior auricularis muscles and the posterior auricular branch supplying the posterior auricularis muscles. The sensory innervation is supplied primarily by the lesser occipital nerve, the mastoid branch of the lesser occipital nerve, the great auricular nerve (C2, C3), and the auriculotemporal nerve. Arnold nerve, a branch of cranial nerve X, supplies the concha.
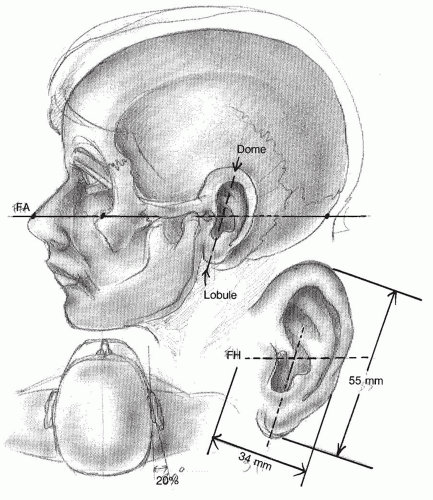
A normal auricle and its dimensions are shown in
Figure 191.3. The superior aspect of the ear is usually level with the eyebrow (
2). The vertical axis of the auricle is typically inclined approximately 20 degrees posteriorly. The vertical height is usually equal to the distance between the lateral orbital rim and the root of the helix at the level of the brow (about 6 cm), and the width is approximately 55% of the length. The helical rim protrudes 1 to 2 cm from the skull at a 21- to 30-degree angle. Traditionally, an ear is considered deformed when the dimensions deviate significantly from these general rules. However, aesthetic appeal is often both subjective and culturally specific. Meticulous preoperative planning with special attention to these factors is essential in achieving normal-appearing and aesthetically pleasing ears.
PROTRUDING EARS
Protruding or prominent ears are a fairly common defect. An extensive array of surgical options is available, and every plastic surgeon should know at least one technique that can be used to achieve reliable results. Optimal
surgical outcome depends on a combination of artistic and technical skills. Although the diagnosis of protruding ears is often made by sight, knowing the basic anatomical dimensions will ensure appropriate decisions regarding intervention. The normal angle between the ear and the head should be between 20 and 25 degrees (
3). Usually, an angle greater than 30 degrees makes the ears appear overly noticeable. Sometimes the auriculocephalic angle of the ear is less than 30 degrees, but some particular anatomic feature makes the ear offensive to the family or patient; therefore, a thorough preoperative assessment and discussion are necessary.
A prominent ear deformity is usually associated with a poorly formed antihelical fold and an overdeveloped concha. The scapha may be malformed with deficient superior and inferior crura surrounding the fossa triangularis. In addition, the helix may be abnormal in both definition and curvature.
Preoperative Evaluation
The preoperative evaluation should include good photographs. In addition to the frontal view, adequate documentation should include oblique, lateral, and rear views. Both ears should be compared and evaluated with regard to at least three basic criteria: the thickness and stiffness of the cartilage and the symmetry of one ear compared with the other. Darwinian tubercles should be noted, as should any other preauricular tags that may exist.
A checklist such as that in
Table 191.1 will ensure that no important details are missed in the preoperative evaluation. This information should be discussed fully with the patient and family to clarify any points of uncertainty. The more involved the patient is in the planning of the surgical procedure, the more likely the postoperative care will be implemented properly.
Emphasizing the importance of making ear reconstruction a family affair, Eavey (
4) counsels parents about the condition as well as techniques to correct the ear. In his study of 92 pediatric patients, Eavey (
4) observed that children with microtia and significant auricular malformation require global attention to early family guidance, including expected and unexpected hearing loss, delayed language development, associated medical conditions, and the need for both auricular and otologic reconstruction.
In 1999, Wang (
5) advocated that early prosthetic treatment is psychologically beneficial to children with congenital ear deformities. In addition, he described procedures to determine precise locations of craniofacial auricular implants by using computed tomographic (CT) scans. Although CT scan is not typically necessary for the correction of prominent ear deformities, it is a useful tool for more complex congenital deformities.
The usual goal of the operation is to achieve some reduction of the auricle angle to within 15 to 25 degrees while maintaining normal appearance and curvature of the auricular components. The helical curve should remain gentle following surgery, with no unusual breaks or pinching effects. The helical rim should be evaluated after the surgery and its height from the mastoid skin documented. The middle third of the helix should measure 14 to 16 mm and the superior third 16 to 18 mm. Reduction of the overdeveloped conchal bowl may be necessary during the surgery as well.
Otoplasty is best begun before the child starts school, between ages 5 and 6, when the child is old enough to withstand the necessary postoperative manipulations. However, Gosain (
6,
7) has demonstrated that it is safe to perform otoplasty on children as young as 9 months old without any effect on the development of the ear.
Surgical Techniques
Mustarde Technique
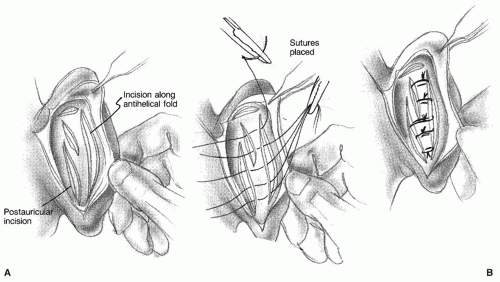
The Mustardé technique (
Fig. 191.4) involves placing several horizontal mattress sutures (usually Ethibon or Ticron) along the scapha in a curved line to create an antihelical sulcus. This technique has several advantages. A normalappearing antihelical fold can be created, and when placed correctly, the sutures hold indefinitely. Most surgeons tend to forget that a Mustardé suture also can be used to create a more than adequate superior or inferior crus.
Problems can be expected with this technique if the sutures are incorrectly placed since they could become noticeable or erode through the postauricular skin. For this reason, postauricular skin excision is usually not recommended. Furthermore, to improve the placement of the sutures, Brent (
8) recently described a hydrodissection technique where normal saline is injected on the anterolateral surface of the ear to elevate the skin away from the cartilage to allow a full-thickness bite of the perichondrium and cartilage. Should the sutures fail to maintain the proper curve of the antihelical fold, a second operation may be required. Simply using a Mustardé technique is usually not sufficient enough for most otoplasties, because work must be done in the conchal bowl area as well.
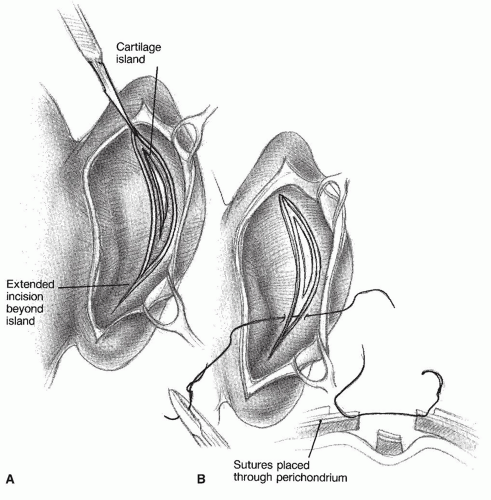
Converse Technique
The Converse technique (
Fig. 191.5) is more complicated and should be executed only by an experienced surgeon (
3). With this technique, an island of cartilage is created that sits anteriorly to the rest of the conchal cartilage. This cartilage produces a normal-appearing fold, with no sharp edges on the corrected antihelix. The advantages of this technique are that it allows more permanent retraction of the auricle and is a potentially more permanent correction of the antihelix. In addition, because the island itself is not sutured, the curvature of the newly created antihelix is gentle.
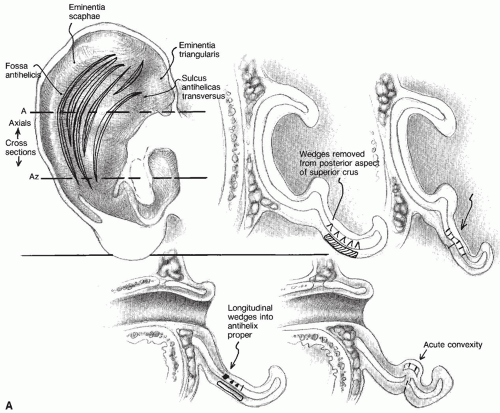
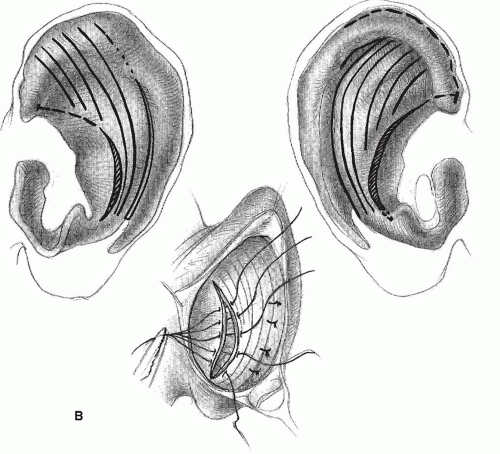
Farrior Technique
This technique (
Fig. 191.6) also requires an experienced surgeon (
9). The incisions are made through the cartilage on the conchal rim only; then longitudinal wedges are removed at the level of the superior crus and the future antihelical fold. An incision then is made through the cartilage at the level of the antihelical fold, creating an island similar to that of the Converse technique. The island widens from the inferior to the superior. This technique produces a more gentle bend of the antihelix. Recent literature has shown that there is approximately a 12% recurrence rate with this technique (
10).
Pitanguy Technique
The Pitanguy technique (
Fig. 191.7) uses a smaller island flap and a conchal setback suture (
3). It is appropriate for use with patients who have only a small amount of antihelical cartilage. Again, this technique requires an experienced surgeon and carries a recurrence rate of 4% (
11).
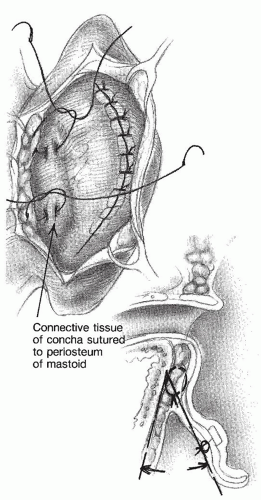
Furnas Technique
The Furnas conchalmastoid suture technique (
Fig. 191.8) is an important procedure for reducing a conchal bowl, as part of any successful otoplasty procedure. When the conchal bowl is too large, an island can be excised to narrow the dimensions of the bowl and to allow the proximal portion to lie firmly against the mastoid bone. The Furnas technique should always be used in conjunction with a conchal-reducing technique. This technique helps to retract the auricle permanently. If the suture is placed too far anteriorly on the mastoid, it can cause some forward buckling of the conchal bowl at the os of the external canal, leading to partial closure of the canal. To avoid narrowing the external auditory canal, it is important to remember to place the mastoid end of the conchalmastoid suture as far posteriorly as possible. These five otoplasty techniques are summarized in
Table 191.2.
Complications and Emergencies
Four major complications can occur following otoplasty (
Table 191.3). The most common complication is inadequate correction, and patients and their families should be alerted to this possibility prior to the operation. A secondary operation may be required within a year, even when the initial otoplasty has been performed by a well-trained surgeon.
A hematoma is probably the easiest problem to detect and is often revealed during the first postoperative examination. Simple drainage should treat this complication. Another complication is the “telephone ear” deformity, which is caused by too much flexion of the antihelix at a level equal to the midportion of the ear and inadequate flexion at the superior and inferior poles. This problem can be prevented by repeatedly checking the tension on all sutures during surgery. Reverse telephone ear can occur from overzealous tightening of the superior and inferior third of the ear.
The most feared complication of otoplasty is chondritis. Infection of the cartilage after an otoplasty can cause permanent, devastating changes in the anatomy of the auricle for which no viable solution exists. Therefore, any infection should be treated promptly and aggressively with antibiotics and possible incision and drainage.
Clinical Indicators for Plastic Repair of the External Ear
Strategy
Indicators (one of the following)
Congenital or traumatic amputation, defect, or deformity
Reconstruction following resection of benign or malignant tumor
Laboratory tests (as indicated)
Other tests (as indicated)
Type of anesthesia (as indicated)
Location of service (as indicated)
Process
Criteria for discharge
Recovery from anesthesia
No bleeding
Outcome
 DIAGNOSIS OTOPLASTY
DIAGNOSIS OTOPLASTY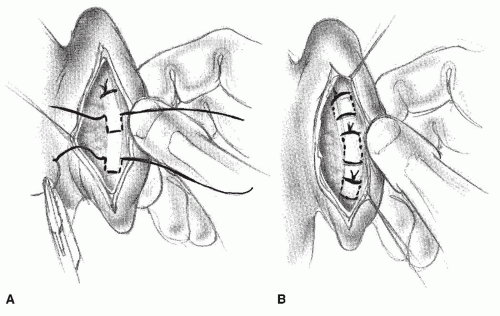
 TREATMENT OTOPLASTY
TREATMENT OTOPLASTY


