25 Complications of Sinusitis • Divided into orbital (60–75%), intracranial (15–20%), and osseous (5–10%) complications • Sinus disease accounts for: • Incidence of complications: • More common during winter months • Males > females • Antibiotics for ARS do not change the incidence of complications • Most common type of complication • Associated with ethmoid, maxillary, frontal, sphenoid in reducing frequency • Chandler classification (Fig. 25.1) • An ophthalmology review is mandatory • IV antibiotics covering aerobic and anaerobic organisms • Presence of ophthalmoplegia, loss of red–green vision/visual acuity—CT with contrast required → surgical drainage • No improvement/deterioration after 48 h IV antibiotics → surgical drainage • CT appearance: – Medial rectus oedema – Lateralization of medial rectus/periorbita – Globe displacement inferolaterally – Loss of detail of extraocular muscles/optic nerve – Possible orbital air • Surgical drainage should also include addressing the adjacent sinuses • Some evidence to suggest in small children with subperiosteal abscesses IV antibiotics sufficient if: • Spread from sinuses through diploic veins or directly through bone erosion • Often involve anaerobic or mixed aerobic/anaerobic organisms • These include: • Symptoms: • Investigations • Treatment • Venous drainage of paranasal sinuses to cavernous sinus—allows haematogenous spread of infection
25.1 Complications of Acute Sinusitis
 10% of intracranial suppuration
10% of intracranial suppuration
 10% of pre-septal orbital infection
10% of pre-septal orbital infection
 90% of post-septal orbital infection
90% of post-septal orbital infection
 2.7 to 4.3 per million (intracranial complications)
2.7 to 4.3 per million (intracranial complications)
 2.5 per million adults (all acute rhinosinusitis (ARS) complications)
2.5 per million adults (all acute rhinosinusitis (ARS) complications)
 1 per 12,000 ARS episodes (children)
1 per 12,000 ARS episodes (children)
 1 per 36,000 ARS episodes (adults)
1 per 36,000 ARS episodes (adults)
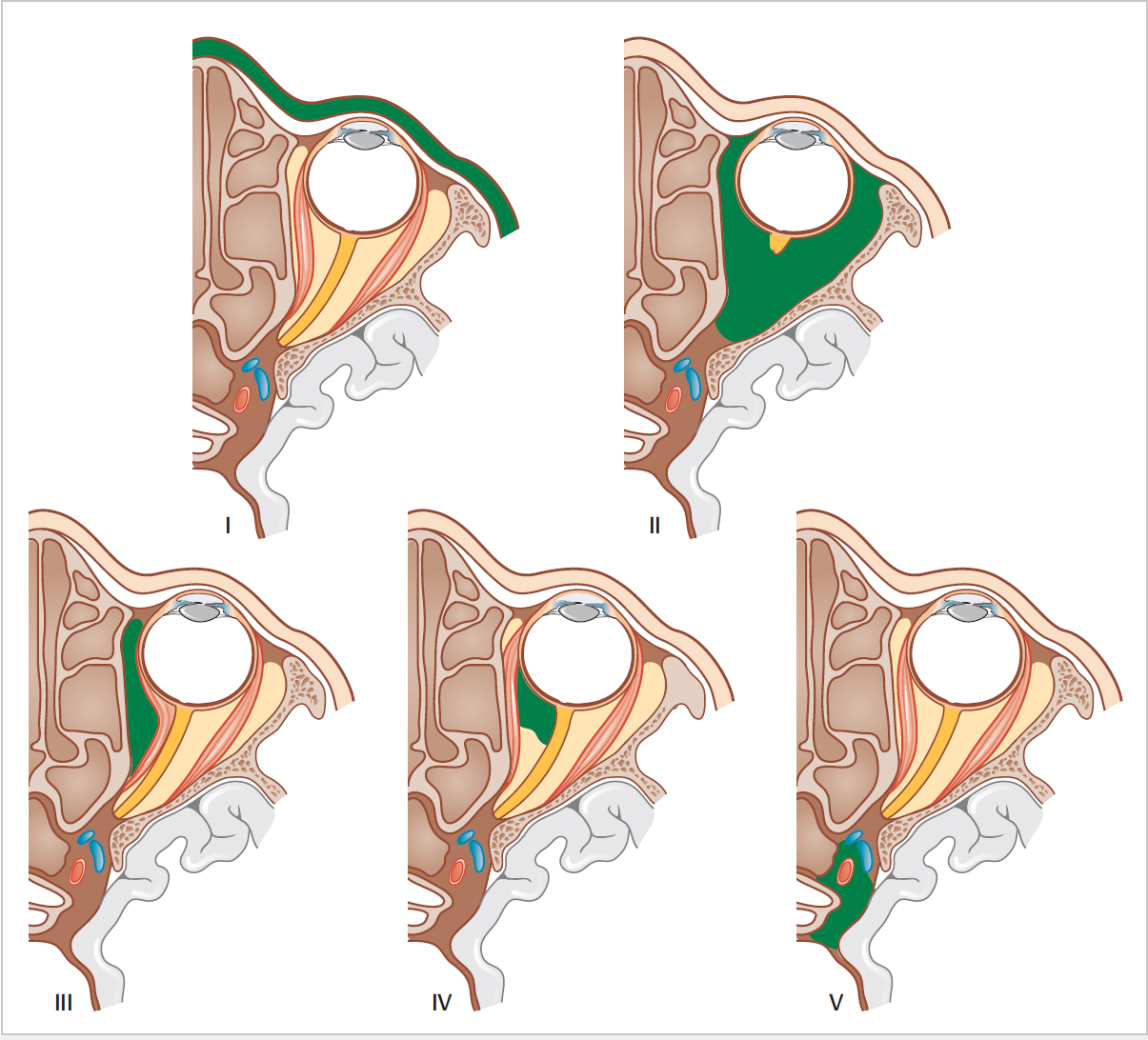
25.1.1 Orbital Complications
 I—pre-septal cellulitis (strictly speaking, outside the orbit)
I—pre-septal cellulitis (strictly speaking, outside the orbit)
 II—orbital cellulitis
II—orbital cellulitis
 III—subperiosteal abscess
III—subperiosteal abscess
 IV—orbital abscess
IV—orbital abscess
 V—cavernous sinus thrombosis (again, not “orbital,” and not necessarily the end stage of orbital infection)
V—cavernous sinus thrombosis (again, not “orbital,” and not necessarily the end stage of orbital infection)
 Subperiosteal abscess:
Subperiosteal abscess:
 Orbital abscess:
Orbital abscess:
 Improving over 48 h
Improving over 48 h
 Normal visual acuity
Normal visual acuity
 <1 mL volume, medial location
<1 mL volume, medial location
 <4 years of age
<4 years of age
 Systemically well
Systemically well
25.1.2 Intracranial Complications
 Epidural, subdural, cerebral abscesses
Epidural, subdural, cerebral abscesses
 Meningitis, encephalitis
Meningitis, encephalitis
 Superior sagittal, cavernous sinus thrombosis
Superior sagittal, cavernous sinus thrombosis
 Nausea and vomiting
Nausea and vomiting
 Neck stiffness
Neck stiffness
 Altered mental state
Altered mental state
 Focal neurological deficits
Focal neurological deficits
 Headache
Headache
 CT scan with contrast—bone erosion
CT scan with contrast—bone erosion
 MRI—soft tissue involvement, cavernous sinus thrombosis
MRI—soft tissue involvement, cavernous sinus thrombosis
 Consider lumbar puncture
Consider lumbar puncture
 Long-term, high-dose IV antibiotics
Long-term, high-dose IV antibiotics
 Craniotomy and abscess drainage
Craniotomy and abscess drainage
 Endoscopic drainage of sinuses
Endoscopic drainage of sinuses
 MC&S of pus, biopsy of abnormal tissue
MC&S of pus, biopsy of abnormal tissue
25.1.3 Cavernous Sinus Thrombosis
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


