19
Complications of Otitis Media
Jerry W. Lin, Mukesh Prasad, and Samuel H. Selesnick
Acute otitis media (AOM) is one of the most prevalent illnesses in children in the United States. A 1989 prospective study by Teele et al1 demonstrated that 83% of children suffered at least one episode of AOM during their lifetime, whereas 46% of children had at least three episodes of AOM by age 3. More recent evidence by Block et al2 in 2001 suggested that the incidence and frequency of episodes of AOM are trending even higher. The use of antibiotic therapy in the treatment of AOM continues to be an active area of clinical investigation, resulting in continual modifications of the guidelines for treatment of AOM. Recent revisions in the management guidelines of AOM have focused on decreasing the use of antibiotics for initial therapy3 (see Chapter 17).
The use of antibiotics for AOM has reduced the incidence of acute suppurative mastoiditis. Conversely, Hoppe et al4 have shown that withholding initial antibiotic therapy for AOM is associated with a rising incidence of mastoiditis. A comparison of the rates of mastoiditis in children from countries with different philosophies for initial antibiotic therapy for AOM has shown that those children in countries with prescription rates of 76% or less have approximately twice the rate of mastoiditis as those in countries with prescription rates of 96% or greater.5 Although the rates of mastoiditis are quite low (4 per 100,000 children) even in those countries with lower prescription rates, the trend toward withholding initial antibiotic therapy requires the clinician to maintain an increasingly high clinical awareness of the signs and symptoms of complications of AOM.
This chapter reviews complications of both acute and chronic otitis media. Complications from otitis media can be organized into extracranial and intracranial areas of involvement, although one does not necessarily preclude the other. Extracranial complications can remain within the temporal bone or can extend beyond its confines (Table 19–1).
 Extracranial Complications
Extracranial Complications
Intratemporal Extension
Acute Mastoiditis
Acute mastoiditis is an inflammatory process of the mastoid air cells of the temporal bone. It is characterized by hyperemia of the mucosal lining of the mastoid air cells with development of fluid and pus within the air cells. Prolonged infection can lead to osteitis and subsequent destruction of the bony trabeculae that delineate the mastoid air cells. Loss of these bony trabeculae results in coalescence of the air cells, which become filled with pus. Once acute mastoiditis has progressed to the point of “coalescence,” surgical management is required.6 In the event that coalescent mastoiditis continues untreated, the process of bony erosion and abscess formation can extend to adjacent structures, resulting in myriad complications, many of which are discussed in this chapter.
As mastoid air cells are contiguous with the middle ear space via the aditus ad antrum, so must mastoiditis be considered an extension of otitis media. Patients with mastoiditis typically present with the symptoms of AOM such as fever, ear pain, and conductive hearing loss. Purulent otorrhea arises in cases of tympanic membrane perforation. Physical examination can reveal edema and erythema of the postauricular soft tissue with pain and tenderness over the mastoid process. Anterior and inferior displacement of the pinna often results in proptosis of the ear. Otoscopic examination may reveal fullness or “sagging” of the posterior-superior external canal wall, secondary to periosteal thickening near the antrum. In addition, the tympanic membrane may show evidence of AOM; if the tympanic membrane is perforated, inflamed middle ear mucosa may be seen through the perforation.
Bacterial cultures obtained from the middle ear in patients with acute mastoiditis most commonly reveal those pathogens involved in uncomplicated AOM: Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Streptococcus pyogenes and Staphylococcus aureus are frequently found in persistent acute mastoiditis. Less common organisms include Pseudomonas aeruginosa and gram-negative organisms such as Escherichia coli and Klebsiella pneumonia.7–9
The discovery of antibiotics and their application to infectious diseases in the middle of the twentieth century greatly reduced the frequency of progression of AOM to acute mastoiditis. Prior to the use of antibiotics, one quarter to one half of patients with AOM could be expected to develop acute mastoiditis.10 In a review in 2001, the incidence of acute mastoiditis in patients with AOM was 0.04 to 0.07%.11
| Extracranial |
| Intratemporal |
| Mastoiditis |
| Ossicular erosion |
| Sensorineural hearing loss |
| Facial nerve paralysis |
| Otic capsule fistula |
| Suppurative labyrinthitis |
| Petrous apicitis |
| Extratemporal |
| Subperiosteal abscess |
| Zygomatic abscess |
| Bezold’s abscess |
| Cervical/postauricular fistula |
| Extramastoid cholesteatoma |
| Intracranial |
| Meningitis |
| Brain abscess |
| Subdural empyema |
| Epidural abscess |
| Lateral sinus thrombosis |
| Otitic hydrocephalus |
| Meningoencephalocele |
A computed tomography (CT) scan of the temporal bone is the optimal imaging modality for the diagnosis of acute mastoiditis. Opacification of the mastoid air cells and the middle ear space can be observed due to mucosal edema as well as fluid or pus collection. Careful attention must be paid to the bony trabeculae defining the mastoid air cells. Haziness of these structures suggests demineralization and loss of integrity of the bony septa. This disease process may progress to complete destruction of the bone, resulting in coalescent mastoiditis and necessitating surgical intervention.
If acute mastoiditis is diagnosed prior to radiographic observation of coalescence, it may be successfully treated conservatively with myringotomy and intravenous antibiotics.12 With earlier intervention, mucosal edema in the antrum may be reduced to allow for adequate clearance of fluid or pus from the mastoid air cells into the middle ear and out the eustachian tube as well as the myringotomy site. Acute mastoiditis that persists despite conservative management requires direct drainage of the infected contents of the mastoid air cells via a cortical mastoidectomy (Fig. 19–1).12,13 Despite the powerful antibiotics available today, acute mastoiditis remains a serious otologic infection. In a recent retrospective review in 1996 of 124 patients with acute mastoiditis, Gliklich et al14 reported that 62% required surgical intervention.
Extension of the infectious process within the temporal bone can manifest as myriad functional disabilities. Spread of infection from the middle ear to the inner ear typically occurs via direct extension either through areas of bony destruction or through preformed openings in the bone, such as the round window, the oval window, or preexisting dehiscences of the temporal bone.
Ossicular Erosion
Chronic suppurative otitis media commonly results in a conductive hearing loss. Conduction of sound through the middle ear is compromised by the presence of pus in the middle ear space; however, damage to the ossicular chain may also contribute to the hearing loss. Typically, bony erosion occurs at the stapes suprastructure and the incus, whereas the malleus is less often involved. Treatment entails prosthetic reconstruction of the ossicular chain once the suppurative otitis media has been controlled.
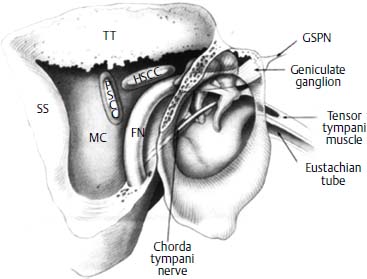
Figure 19–1 Surgical anatomy of the middle ear and mastoid after a cortical mastoidectomy includes the mastoid cavity (MC), the facial nerve (FN), the horizontal semicircular canal (HSCC), the posterior semicircular canal (PSCC), the sigmoid sinus (SS), the tegmen tympani (TT), and the greater superficial petrosal nerve (GSPN). (From Selesnick SH, Jackler RK. Facial paralysis in suppurative ear disease. Operative techniques in Otolaryngology. Head Neck Surg 1992;3:61–68. Reprinted by permission.)
Sensorineural Hearing Loss
Occasionally, sensorineural hearing loss may be found in patients with chronic otitis media. In fact, sensorineural hearing loss has been positively correlated with the duration and severity of otitis media.15 The mechanism of hearing loss is not completely understood. The most commonly proposed theory is that pathologic changes in the round window membrane can render it more permeable to bacterial toxins. Thus passage of chemical toxins from the middle ear into the inner ear via the round window may damage the cochlear apparatus.16,17 A study in 2004 has shown that introduction of fluorescencelabeled endotoxin into the middle ear can lead to accumulation of intense fluorescence in the basal turn of the cochlea.18 Consistent with this observation, another study detailing cochlear morphology in the setting of chronic otitis media described loss of outer and inner hair cells in the basal turn of the cochlea.19 Nevertheless, studies that found no cochlear pathology and described improvement of hearing following treatment of otitis have led to postulation of otitic change in middle ear resonance or change in mechanics of sound transmission as the etiology of the sensorineural hearing loss.20 Clarification of the mechanism of hearing loss remains an active area of investigation.
Facial Nerve Paralysis
Facial nerve paralysis is a rare complication of otitis media. Of all cases of peripheral facial paralysis, those secondary to otitis media comprise 6 to 8%.21 The timing of the development of facial paralysis after onset of otitis media is important to consider as it suggests the pathophysiology of the symptoms and, more importantly, has implications for the treatment of the disease. Facial palsy that occurs in the acute setting, that is, within 2 weeks of onset of otitis, likely represents injury to a dehiscent, exposed facial nerve by bacterial toxins with resultant neural edema. Inflammatory edema, as it extends to portions of the nerve that are contained within a bony canal, leads to compression of the nerve and neuropraxia secondary to ischemia.22 Treatment of acute onset of facial nerve paralysis in the setting of otitis media includes intravenous antibiotics and wide myringotomy to decompress the middle ear. Typically, complete resolution of nerve palsy is expected.23
If facial paralysis occurs after 2 weeks of otitis media, it is more likely that bony erosion has occurred to allow access of bacterial toxins to the facial nerve (Fig. 19—2). Bony erosion also can occur in the setting of cholesteatoma that has eroded through the fallopian canal and compresses the facial nerve directly. In these cases, mastoidectomy with facial nerve decompression is indicated.24 The nerve should be identified, any granulation tissue should be exenterated, and the facial nerve should be decompressed several millimeters distal and proximal to the area of involvement. In cases of cholesteatoma invasion of the fallopian canal, all cholesteatoma must be removed to relieve pressure on the facial nerve. Intraoperative facial nerve monitoring may supply meaningful information.
Otic Capsule Fistula
The endosteal bone that forms the otic capsule is subject to damage from an inflammatory process that is engendered by infection or more typically, by cholesteatoma. A fistula arises when the endosteal bone layer has been eroded, leaving only the endosteal membrane to separate the perilymphatic space from the infectious or cholesteatomatous process in the middle ear (Fig. 19–3).25 The lateral semicircular canal is more frequently involved than the superior or posterior semicircular canals; the cochlea is rarely involved. The incidence of otic capsule fistula in the setting of chronic otitis media is 3.6 to 12.9%.26–28
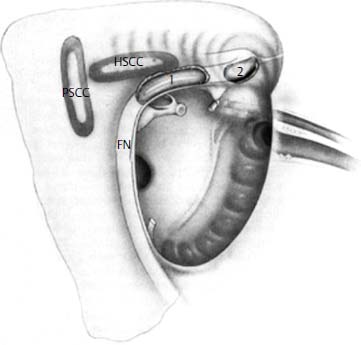
Figure 19–2 Typical sites of facial nerve (FN) erosion by cholesteatoma and otitis media. The posterior portion of the tympanic segment and the second genu (1) and the anterior portion of the tympanic segment near the first genu (2) are most commonly affected. HSCC, horizontal semicircular canal; PSCC, posterior semicircular canal. (From Selesnick SH, Jackler RK. Facial paralysis in suppurative ear disease operative techniques. Otolaryngol Head Neck Surg 1992;3:61–68. Reprinted by permission.)

Figure 19–3 Lateral semicircular canal erosion. In this coronal CT scan of the temporal bone, the endosteal bone covering the lateralmost aspect of the lateral semicircular canal (white arrow) has been eroded by an epitympanic cholesteatoma.
Patients who develop otic capsule fistulas typically present with dizziness and a chronically draining ear. Interestingly, the severity of symptoms depends on the rate of change in the size of the fistula rather than the absolute size of the fistula.29
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


