Fig. 12.1
Radiation-induced mucositis with incipient breakdown of the buccal mucosa (Reproduced with permission of Springer Science and Business Media)
Minimizing the exposure of affected mucosa by tobacco, alcohol, or poorly fitting dentures should be considered in the management of mucositis. Optimizing the nutritional status of the patient and giving instructions for oral hygiene may aid in management. Saline and bicarbonate lavage may be used in the management of non-confluent mucositis. Topical xylocaine and other analgesics may be used to relieve oral discomfort. Treatment breaks should be avoided due to the accelerated repopulation features of the tumor.
Oral hygiene and mouth care are of utmost importance for decreasing the incidence and severity of oral complications. Patient education about the rationale for oral hygiene should be considered at the very outset. Effective oral hygiene maintenance is required throughout the treatment course to avoid complications. Frequent rinsing (four to six times daily) of the oral cavity with 0.9 % saline is common practice in many centers. Avoiding the use of drying agents such as alcohol or glycerine-based products may be beneficial. Dental brushing with toothpaste, dental flossing, sodium bicarbonate rinses, and ice chips are useful in achieving bacterial dental plaque control . Cleaning of the oral cavity after meals is important. Reduced salivary function as a result of xerostomia may cause accumulation of food and debris, which requires more frequent hygiene.
Lip care products including petroleum-based oils and waxes may be used to avoid dryness of the lips.
Instruction of patients for routine follow-up with an expert dentist is crucial. A meticulous dental assessment several weeks before radiotherapy commencement is required to allow for adequate time interval for tissue healing if invasive oral procedures such as dental extraction are indicated. The potential risk of soft tissue necrosis and osteoradionecrosis may be reduced with this timely approach [3, 4].
Oral candidiasis is a frequent infection of the oropharynx in patients receiving radiotherapy to the head and neck region. This infection may aggravate mucositis since the yeast colonize the injured mucosa. Topical antifungals such as nystatin and clotrimazole may be used in the management of oral candidiasis. Systemic antifungals such as flucanozole and ketoconazole may also be used if necessary.
Mucosal healing usually occurs rapidly after completing radiation treatment.
3 Taste Changes
Atrophy and degeneration of taste buds may result as a consequence of oral cavity irradiation. Taste buds are susceptible to irradiation, and sensations of sweet, sour, salty, or bitter may be affected. Incidence of taste changes is dependent on radiation dose. Though recovery may be observed within a few months following treatment in some patients, persistent changes may also occur.
Patients should be instructed to chew foods longer to allow for more contact of foods with taste buds. Also, smelling the foods before eating may be recommended since taste and smelling senses are interlinked.
4 Xerostomia
Reduction in salivary flow as a result of salivary gland damage is a frequent complication of head and neck radiotherapy. Saliva is required for normal execution of oral functions including swallowing, taste, and speech. So, permanent impairment of salivary function may have several clinical consequences and may substantially affect qualiy of life. As the salivary viscosity increases, lubrication of oral tissues is impaired and buffering capacity is compromised with increased risk of dental caries and progressive periodontal disease. Due to the patient’s difficulty in maintaining oral hygiene and mechanical cleansing, oral flora becomes more pathogenic and plaque levels accumulate.
Unstimulated whole salivary flow rates under 0.1 mL/min are indicators of xerostomia. Significant reduction of salivary gland within the necrosis field causes xerostomia [5]. Typical symptoms and signs include dryness, fissures at lip commissures, burning sensation of the tongue, a dorsal tongue surface atrophy, increased thirst, and difficulty in wearing dentures (Fig. 12.2).

Fig. 12.2
Radiation-induced xerostomia and dental caries secondary to radiation therapy (Reproduced with permission of Springer Science and Business Media)
Xerostomia occurs as a result of inflammatory and degenerative effects of radiation on the salivary gland parenchyma. Salivary flow decreases within the first week after radiotherapy commencement, and continual progressive decrease occurs during the course of treatment. The severity of hypofunction is dependent on the dose of radiation and volume of glandular tissue within the radiotherapy field. Severe radiotherapy-induced xerostomia with less than 25 % of the baseline salivary function may be avoided by sparing at least one parotid gland to a mean dose of <20 Gy or by sparing both parotid glands to <25 Gy [6]. Nevertheless, keeping the parotid mean doses as low as possible without compromising clinical target volume coverage is recommended since better function of the parotid glands may be achieved with lower parotid mean doses [6].
Patients with xerostomia should maintain their oral hygiene to minimize the risk of oral lesion formation. Unless preventive measures are taken, periodontal disease may deteriorate and caries may become uncontrollable. Preventive strategies include plaque removal by toothbrushing and flossing; remineralization by the use of topical and/or systemic remineralizing solutions; rinsing with antimicrobials such as chlorhexidine, povidone iodine, etc.; and using sialogogues such as pilocarpine and bethanechol.
Surgical interventions may be used in the management of xerostomia [7–9]. Complementary methods such as acupuncture have been used for xerostomia prevention [10, 11].
Amifostine (WR-2721), which is a pro-drug dephosphorylated by plasma membrane alkaline phosphatase to the active metabolite of free thiol WR-1065, exerts its radioprotective action by scavenging free radicals produced by head and neck irradiation along with its detoxification effect used in chemotherapy-induced renal toxicity reduction. It is used as a radioprotective agent to reduce xerostomia in patients with head and neck cancers who are receiving radiotherapy [12–15].
Temporarily wetting the oral mucosa by saliva substitutes or artificial saliva preparations is a palliative cytoprotective strategy to relieve discomfort of patients with xerostomia.
Pilocarpine, a parasymppathomimetic agent, is used in the management of radiotherapy-induced xerostomia [16–18]. It may have a radioprotective effect on salivary glands if used during head and neck radiotherapy. Pilocarpine typically increases salivary flow within 30 min after ingestion. Continual use is required to achieve maximal benefit. Treatment is initiated at 5 mg orally, thrice daily, and dose is then titrated to achieve optimal balance between clinical response and side effects. Allowing a week between dose increments is recommended to confirm patient tolerance. Hyperhidrosis is a common adverse effect of pilocarpine.
5 Skin Toxicity
An overwhelming majority of patients receiving radiotherapy for head and neck cancers experience varying degrees of acute skin effects. Treatment-related factors include total dose, dose per fraction, type and energy of radiation, use of beam modifiers, the size of radiotherapy fields, and the use of concomitant therapeutic agents such as chemotherapeutics, radiosensitizers , monoclonal antibodies, etc. Patient-related risk factors include impaired nutritional status, fair complexion, history of extensive sun exposure, comorbid diseases such as diabetes mellitus, and collagen vascular diseases such as scleroderma and lupus.
Skin reactions range from mild erythema or dryness to dry or moist desquamation. Symptoms are usually temporary. Typical onset of symptoms occurs approximately 2 weeks after the commencement of radiotherapy and may persist up to 4 weeks after treatment completion (Fig. 12.3).

Fig. 12.3
Typical skin reaction after head and neck radiotherapy (Reproduced with permission of Springer Science and Business Media)
Management of skin toxicity includes adhering to principles of good wound care and maintaining a clean environment. Careful cleansing of the skin is warranted. Moisturizers (Acuophor or aloe vera gels) may be applied to areas of dry desquamation. Mechanical and chemical irritation of treated skin must be prevented by avoiding tight clothes, perfumes, etc. In the presence of moist desquamation, additional measures should be taken to avoid skin infections and consequential treatment breaks.
6 Osteoradionecrosis
Direct osteocytic damage or injury to the small vasculature of the haversian systems and the periosteum by irradiation may negatively affect the bone’s capability to resist trauma and avoid infections. Pathologic fractures may occur since the compromised bone has lost its ability to repair itself. Pain, fistula, infection, and complete or partial sensational loss may occur.
Osteoradionecrosis typically involves the mandible in head and neck radiotherapy with varying incidences reported in retrospective series. The risk of osteoradionecrosis increases with trauma, oral infections, and intimate association of primary tumor with the bone. Osteoradionecrosis typically occurs within the first 3 years after diagnosis of head and neck cancer (Figs. 12.4 and 12.5).
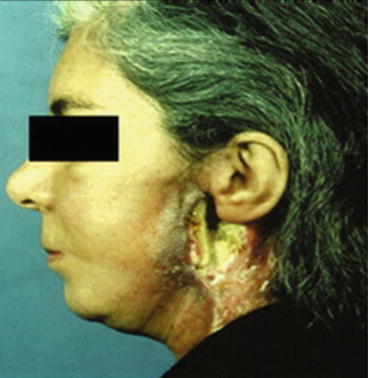
Fig. 12.4
Skin breakdown and osteoradionecrosis of the mandibular angle and ascending ramus after radiotherapy for a parotid gland tumor (Reproduced with permission of Springer Science and Business Media)
Fig. 12.5
Radiological aspects of osteoradionecrosis. Mixed radio-opaque radiolucent lesion, with the radiolucent areas representing bone destruction and axial CT of the mandible with osteoradionecrosis showing (a) small sequestra of bone (b) symphysis pathological fracture (Reproduced with permission of Springer Science and Business Media)
Management of osteoradionecrosis includes the maintenance of meticulous oral hygiene, elimination of trauma, avoidance of removable dental prostheses when the denture bearing area is within the necrosis field, maintenance of adequate nutritional intake, and discontinuation of alcohol and tobacco consumption [19]. If attempts to preserve teeth are unsuccessful, postradiotherapy dental extractions should be performed cautiously due to the risk of initiating osteonecrosis. Topical or systemic antibiotics may be used in the presence of infection. Analgesics may be indicated for pain management. Local resection of loose bony spicules may be possible. Hyperbaric oxygen treatment may be recommended if conservative treatment has failed and the patient suffers from increasing pain. It may result inconsiderable pain relief through increased oxygenation of irradiated tissue, enhanced angiogenesis, increased osteoblast repopulation , and fibroblast function.
Surgical resection of the irradiated mandible may be indicated in severe cases of osteoradionecrosis. Reconstruction of the mandible may be considered to achieve continuity for esthetics and functionality. A multidisciplinary approach is warranted in the management of these patients.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


