Compliant Documentation, Coding, and Billing in the Practice of Otolaryngology— Head and Neck Surgery
Stephen R. Levinson
How many physicians look forward to learning about documentation and coding? Probably as few as the number of businessmen who want to learn the details of the tax code. Yet documentation and coding are as integral to the practice of medicine as accurate bookkeeping and correctly filing taxes are to anyone operating a business. From their earliest exposure to performing history and physical examinations, medical students who have great teachers are admonished that their documented medical record for each patient encounter should be an accurate and understandable reflection of the medical care they provided and the thought process they followed. (As summarized by the great medical record innovator Dr. Lawrence Weed, “It’s not sufficient to just know what was done. It’s a very incomplete record if we don’t know why it was done” (1). What is, however, seldom appreciated and rarely taught is that the use of creatively designed medical record documentation tools can improve quality, compliance, and efficiency for recording diagnostic and surgical procedures and especially for documenting and coding evaluation and management (E/M) care. When used for documenting E/M services, effective medical record tools also increase workflow efficiency and promote physicians’ diagnostic patient care process. The benefits of effective documentation further extend to include audit compliance, medicolegal protection, communication with other physicians, and, most importantly, helping to ensure optimal patient care for both current and future visits.
While physicians almost universally understand the role that coding plays in filing claims for insurance, they must also appreciate its role in data retrieval and information processing. In the office setting, diagnostic and procedure codes are the gateway to accessing the records of patients who have undergone specific procedures or who have been diagnosed with particular illnesses. Accurate coding facilitates chart review and analysis of the success of various treatment options, as well as initiating patient recalls under appropriate circumstances. These individual practice benefits are magnified by combining related data from large numbers of physician practices, facilitating “comparative effectiveness research” (CER), which is one of the promised benefits of widespread use of electronic health records (EHRs). The requirement for coding correctly has been underscored by the proliferation of coding and health information management (HIM) professionals, who in various settings may be employed to review, assist, or even replace coding by physicians. However, even if their hospital or practice employs coding professionals, physicians need to understand coding fundamentals to achieve correct codification of patient care and to ensure receiving proper payments for their services.
SURVEYING THE CURRENT ENVIRONMENT AND SEARCHING FOR SOLUTIONS
Why do physicians so frequently complain that the tasks of creating consistently compliant (2) documentation and coding are confusing, challenging, and/or unrelated to their goals for medical practice? It is far easier to learn how to identify the precise procedure and diagnostic codes for excision of a benign neoplasm of the lateral lobe of a parotid gland with dissection and preservation of the facial nerve (CPT code 42145 and ICD-9 code 201.2) than it is to master the surgical technique required to perform that challenging operation safely and well. Similarly, with a relatively small amount of training combined with compliantly designed (and physician-friendly) medical record forms, it is far easier to perform and document the medically indicated level of care for a new patient with probable Meniere’s disease (CPT code 99204 and ICD-9 code 386.01) than it is to master the optimal evaluation and management pathways for each patient who presents with significant vertigo.
This author believes there are three factors creating barriers to logically and naturally incorporating precise documentation and accurate coding into optimal medical workflow and patient care excellence:
Lack of early training in coding principles and their integration into medical care
Lack of efficient and compliant documentation tools that can enable physicians to create documentation at the level and precision that is taught and required
Lack of teaching physician and practicing physician role models who excel in compliant documentation and coding
All three of these deficiencies could, and should, be remedied by introducing effective curricula and documentation tools at the appropriate junctures during medical education. For example, effective documentation of a comprehensive history and physical examination (the “H&P”) is traditionally taught as the first medical school course in clinical medicine, and this meaningful clinical documentation almost exactly parallels the compliant H&P required for evaluation and management (E/M) documentation and coding. This would be an optimal time to introduce sophisticated documentation tools to help young physicians provide and document the desired level of care compliantly. Use of such tools would also allow students to achieve good care far more efficiently than the “time-honored” approach of documenting with only a blank sheet of paper and a pen. As almost all physicians have experienced, performing and documenting a comprehensive H&P with such primitive technology requires between 45 and 90 minutes per patient encounter; this is the medical record equivalent of training students to examine the tympanic membrane using nothing more advanced than direct vision with an open ear speculum or to auscultate the heart by placing their ear directly against the patient’s chest.
The demands of our current medical environment require practicing physicians, academic physicians, residents, and even medical students to complete patient encounters within 10 to 20 minutes. Unfortunately, failure to provide sophisticated documentation tools that facilitate performing and documenting extensive care within this time frame has forced student physicians (and now their professional supervisors and role models) to abandon the high-quality history taking and physical examination they were taught to perform. As a consequence, most physicians currently provide and record only “problem-focused” patient care, which creates compliance problems for their evaluation and management services. The current transformation to EHRs offers a welcome window of opportunity to provide such tools, but unfortunately most current EHR data entry designs have failed to facilitate the recording of individualized (patient-specific and visit-specific) documentation that “meet all of the optimal standards that physicians should apply to introduction of any medical record technology… usability, efficiency, E/M compliance, promotion of individualized quality care, and data integrity” (3). In the optimal documentation and coding model presented here, medical students would receive medical record tools and instruction that together facilitate their ability to provide the comprehensive (and compliant) H&P taught during their early clinical training. This monitoring and mentoring of patient care and documentation should continue throughout residency training as well. In addition, it appears reasonable and logical that, at the onset of residency training, effective and compliant documentation templates should be introduced for recording diagnostic and therapeutic procedures, helping residents develop, practice,
and thereby maintain effective procedure documentation techniques from the outset.
and thereby maintain effective procedure documentation techniques from the outset.
Linking the Quality History and Physical Examination with E/M Documentation and Coding
Since the mid-1970s, probably the most commonly used reference text for teaching medical students the principles of obtaining and documenting a high-quality history and physical examination is the Bates’ “Guide to Physical Examination and History Taking” (4). Revealingly, comparing both the E/M section of the AMA publication “Current Procedural Terminology” (5) (CPT) and the American Medical Association (AMA)/Centers for Medicare and Medicaid Services (CMS) publication “Documentation Guidelines” (6) with the Bates’ Guide text of clinical practice makes it apparent that “this reference book is unquestionably the source of the E/M coding system. The descriptions of medical history and physical examination match concept for concept, paragraph for paragraph, and often almost word-for-word among the three documents. This includes not only the broad concepts, but also the details such as the various organ systems listed in the review of systems and physical examination and the specific definitions for chief complaint (CC) and history of present illness. It also includes a similar overview of formulating and documenting clinical assessments and treatment plans. Most impressively, the Bates’ Guide also presents the concept of the ‘nature of the patient’s problem.’ This component of patient assessment parallels CPT’s similarly named E/M component ‘nature of the presenting problem’ (NPP), which plays a pivotal role … in helping physicians understand how an effective E/M system promotes excellence in patient care.
In summary, the E/M coding system is actually a codification of the medical diagnostic process that all physicians learn in their training as being the most effective method for providing high-quality patient care. Making physicians aware of this relationship allows them to view compliance-based records from a fresh perspective: rather than being an added chore at the conclusion of patient care, carefully designed IMR (Intelligent Medical Record) tools can help physicians comfortably provide optimal care within a time frame that meets the limitations of the current health care environment” (7).
Finally, the beginning of residency training would also be an optimal time to introduce the fundamental concepts of coding for procedures (CPT coding) and diagnoses (ICD-9 coding, soon-to-be replaced by ICD-10 coding). These alphanumeric codes provide a shorthand “language” for recording and reporting the care physicians provide. Just as early childhood is the most successful learning time frame for introducing an individual to a new language, incorporating coding as a parallel language early in residency will enable young physicians to speak this language fluently.
Unfortunately, our medical training programs do not currently provide this idealized approach to incorporating effective documentation and coding skills and tools as an integral component of learning medical care excellence. Instead, upon completing residency training, most physicians are plunged unprepared into the chilling waters of creating documentation that must meet regulatory demands for coding and billing, performance measures, medicolegal protection, and compliance reviews. This current reality calls for an explanation of documentation and coding that can make these principles understandable and workable for practicing and academic physicians, for residents, and even for medical students.
The remainder of this chapter is devoted to presenting the basic principles of each component of coding and documentation and examining their interplay with the current payment system in the United States. This includes examples of structured documentation tools capable of incorporating these principles into the normal workflow of quality patient care, and it underscores the basic tenet that proper coding and documentation must accurately report the care provided, not distort that care to meet external regulatory demands.
DOCUMENTATION FUNDAMENTALS
Hippocrates probably documented his patient care by writing freehand on parchment with a quill pen. As his patient volume increased with his widening fame, he probably began to experience the time limitations of creating accurate records using such limited technology. Yet over the next several thousand years, the only significant technologic advances for improving medical documentation were the introduction of milled paper and the ballpoint pen. With mounting time pressures, many physicians increased their writing speed by becoming less and less legible, some even attaining a level of illegibility that left them unable to read their own notes. A significant alternative for recording care finally appeared in the 20th century in the form of dictation. This offered physicians an option that was definitely legible and could also be faster than writing an entire record in longhand. In addition, however, it added the often-significant cost of transcribing the dictated records into paper documents.
Whether created by handwriting or dictation, the final medical records were stored as paper documents, which have inherent limitations in ease of access and costs of storing, retrieving, and sharing the records, as well as mining them for data. The heralded introduction of EHRs offers solutions to these information storage and retrieval problems, but it has also introduced a broad spectrum of challenges to effective data entry. Early on, physicians adopting EHRs were required to type their medical observations into the software programs, a process that is not only usually slower than either dictation or writing but also creates barriers to good patient-physician interaction (or alternatively leads to the double effort of physicians writing notes to themselves on paper, which they then use to type their notes at the end of the day, long after seeing their patients; this is a suboptimal and perhaps noncompliant solution to the data entry challenge). Eventually, some electronic records introduced full or partial dictation alternatives, but many have also introduced a variety of automated data entry shortcuts by copying and pasting blocks of text from previous records and/or from preloaded generic descriptions. While speeding the process of documenting a patient encounter, these shortcuts severely curtail individualized documentation, introducing significant problems with compliance (8,9,10) and challenges in understanding what was actually performed (and why it was performed) during each encounter. Fortunately, effective data entry solutions are achievable, and these are also able to provide documentation that is accurate, individualized, and efficient. Physicians should therefore establish criteria that the data entry features of EHR systems must meet to ensure usability, efficiency, compliance, data integrity, and promoting quality care.
Toolkit for Designing Medical Records to Meet Physicians’ Needs
There are several medical record documentation tools that can help physicians create records that surpass the standard written or dictated format. These include
1. Choice of interface (graphic and narrative): Traditional medical record documentation required that all information be entered as free text. This approach necessitates a time commitment that is unreasonably excessive to meet today’s medical care demands.
Narrative interface: There remains a critical requirement for free-text narrative descriptions for those portions of a medical procedure or visit that call for analog (expository) documentation (e.g., an individualized history of the patient’s present illness during a visit for evaluation and management care).
Graphic interface: A preprinted list of questions or descriptions from which to select appropriate responses using check boxes or similar indicators (e.g., a survey of possible medical illnesses in the past
medical history section of the H&P screen or form). A more sophisticated variation expands this option by also allowing the entry of brief written details along with positive responses to the preentered questions.
2. Use of preloaded information (templates and macros): Criteria for proper medical record design for documentation of procedures and, particularly, of evaluation and management services must carefully distinguish between template designs that facilitate efficiently recording individualized care and macro designs that automatically enter identical clinical information in visit after visit and case after case (a process that is labeled “cloned documentation”). While these features have become pervasive in many EHRs, some physicians have incorporated templates or macros into their written or dictated paper records, where they have similar advantages and potential dangers.
Template: A preloaded graphic interface section that provides detailed structure but no substance until active documentation is entered
An effective office template should list all the elements of a comprehensive ENT physical examination with blank check boxes after each element to indicate either “normal” or “abnormal” findings. The physician checks the appropriate finding for each area examined and leaves blank those boxes for exam elements not performed during a particular patient encounter (all abnormal findings are further described with supplemental narrative detail).
In other words, until a physician documents his or her actual findings, the paper form or electronic screen shows only a blank template of information. There is NO preloaded documentation that anything has yet been performed.
Well-designed templates provide similar advantages for documentation of PFSH (past history, family history, social history) and Review of Systems obtained during initial E/M visits.
Macro: A preloaded graphic interface section that provides detailed structure plus standardized substance, because all of the check boxes have been prefilled to indicate normal findings (alternatively, in EHRs, a template form may be converted to a macro when a single electronic “click” automatically checks all of the normal boxes). In its narrative form, a macro’s preloaded information presents as one or more completed descriptive paragraphs that appear identical to a dictated normal head and neck examination (or a completely negative background history and review of systems).
In other words, before the physician even meets the patient, the macro-loaded paper form or electronic screen attest that he or she has performed a comprehensive head and neck examination and the findings were 100% normal.
Hypothetically, such macros require “documentation by exception”; that is, the physician is supposed to undocument all exam elements that were not performed and to re-document all exam elements that were found to be abnormal. If done correctly, this undocumentation and re-documentation process, though compliant, actually requires more time and effort than individually checking the blank boxes of a template. It is also subject to multiple oversights that can result in erroneous documentation. In practice, few physicians expend the effort to re-document their macros. As a result, even when physicians using macros perform a limited or focused examination, their records commonly report a comprehensive examination for every visit, almost always with all normal findings except for the one or two areas related to the patient’s presenting problem.
Unless a physician meticulously reviews each item of a macro and undocuments and redocuments each element that was not normal (or negative), the use of macros inevitably results in “cloned documentation.” (A recent analysis from the Department of Biomedical Informatics at Columbia University reported that EHRs using macros created medical records where 54% of the wording was identical on progress notes and 78% was identical on discharge notes (11).)
The use of macros in creating medical documentation will usually fail to support a physician under the scrutiny of a compliance audit, as noted below, or a medicolegal inquiry. Clinically, unless extensively modified line-by-line, macros also fail to convey meaningful patient-specific and visit-specific information needed to assist the physician in the ongoing care of his or her patients.
For E/M services, it is clear that macros should not be used for documenting any portions of the medical history or physical examination. On the other hand, the “correct use” cited above would permit macros to be used effectively and compliantly in portions of the medical decision-making E/M component, to import standard lists of diagnostic tests and/or treatment programs for specific diagnoses. However, such use still requires review for appropriateness and individualized customization during each encounter, prior to incorporating a macro into the medical record.
Similarly, it appears that macros should have only carefully controlled use in operative reports, permissible only for standard manipulations and only if there is additional individualized narrative information describing the key portions of the diagnostic or therapeutic procedures.
The Compliance Verdict on “Cloned” Medical Record Documentation
Over many years, CMS and various Medicare Carriers have released a series of critiques of “cloned” medical records, that is, records created by various macro techniques such as “copy forward” (of information from a patient’s previous visits), “copy/paste” (of preloaded generic history or examination descriptions), and/or documentation by exception. In 2007, First Coast Service Options, the Florida Medicare carrier, issued a persuasive condemnation of these documentation techniques:
“Cloned documentation does not meet medical necessity requirements for coverage of services rendered due to the lack of specific, individual information. All
documentation in the medical record must be specific to the patient and her/his situation at the time of the encounter. Cloning of documentation is considered a misrepresentation of the medical necessity requirement for coverage of services. Identification of this type of documentation will lead to denial of services for lack of medical necessity and recoupment of all overpayments made” (12).
documentation in the medical record must be specific to the patient and her/his situation at the time of the encounter. Cloning of documentation is considered a misrepresentation of the medical necessity requirement for coverage of services. Identification of this type of documentation will lead to denial of services for lack of medical necessity and recoupment of all overpayments made” (12).
The compliance (and potential financial) danger of improperly employing these data entry techniques was further underscored in a white paper issued in 2007 by the Department of Health and Human Services (HHS) and the Office of the National Coordinator for Health Information Technology (ONCHIT). Their assessment uses the term “templates” to indicate the characteristics of “macros” as described above:
“These tools include the use of defaults, templates (i.e., macros), copying, and others. These are legitimate benefits of using an automated system and can be extremely helpful if used correctly; however, the tools can also open the EHR-S up to fraud or abuse” (13).
3. Optimal use of data entry personnel: Although all documentation of the medical history and physical examination has traditionally been entered by the physician (as instructed in medical school), the 1995 and 1997 editions of the Documentation Guidelines provide two far less time-consuming alternatives for obtaining and documenting multiple subcomponents of the medical history. They instruct, “The ROS (Review of Systems) and/or PFSH (Past History, Family History, and Social History) may be recorded by ancillary staff or on a form completed by the patient” (14). This guidance is highly logical, because each physician employs his or her own standard set of questions for each of these medical history elements. Permitting patients to review and respond to these inquiries is extraordinarily efficient. It allows physicians to elicit and record a comprehensive medical history without significant time expenditure. Further, the information obtained promotes quality care by providing full background information, identifying both contributory and unrelated medical issues. These insights allow physicians to accurately determine a preliminary differential diagnosis and a preliminary assessment of the nature of the patient’s problem (“NPP”—the E/M coding system’s measure of medical necessity).
Of course, medically it is insufficient just to obtain and document this medical history information; the physician must also review the responses and further investigate all positive findings (i.e., it is not sufficient to simply record that a patient has chest pain—the physician must inquire about the details to determine whether this symptom may be medically significant, potentially health endangering, and/or require assessment). The Documentation Guidelines reflects this quality care mandate by requiring “to document that the physician reviewed the information, there must be a notation supplementing or confirming the information recorded by others” (14) (note: clearly the advice to “supplement” refers to all positive responses, while “confirm”—with an attestation by signature—is appropriate to indicate review of all the negative responses).
4. Optimal use of appropriate data entry modalities: Effective documentation requires the use of data entry tools that facilitate the efficient entry of individualized and accurate medical information. In the traditional paper environment, physicians elect to write or dictate their documentation. Prior to the introduction of EHRs, few, if any, physicians chose to record the H&P by typing, either during the care process or as an additional step following each encounter. The process would be too time-consuming and/or too intrusive into the physician-patient interaction.
Considering these drawbacks, it is remarkable that numerous EHR software systems have chosen to require the use of keyboard and mouse as the primary or only technology available for physicians to document their care. Therefore, to meet the usability, efficiency, and patient interaction requirements of all physicians, it should be required that EHRs provide at least one alternative for each data entry option
For physicians who prefer direct computer entry, use of keyboard and mouse
For physicians who prefer to dictate some or all of their records, use of (i) voice recognition software or (ii) dictation with transcription
For physicians who prefer to write (legibly) some or all of their records, use of (i) a tablet PC or (ii) a digital pen with digital paper
In addition to physicians’ personal preferences, each of these technologies offers its own particular advantages and limitations (15). Often overlooked is the potential added efficiency and usability of combining two or more of these modalities, each being employed where it is most comfortable for the physician. For example, a physician with poor handwriting might elect to use a tablet PC or mouse entry with clicks to rapidly place Xs in the check boxes of the graphic interface section of the physical examination (see Fig. 200.7) while dictating the free-text narrative required to precisely describe the details of each of the abnormal findings.
CODING AND BILLING FUNDAMENTALS
Whereas the principles and practice of physicians accurately documenting their patient care have been evolving since Hippocrates saw his first patient, the concept of “codifying” that patient care is a relatively recent phenomenon. It was not until the 1980s that Medicare and most insurers began requiring that physicians submit their claims for payment using CPT procedure codes and ICD diagnostic codes. Prior to that time, physicians submitted most insurance forms with a freetext description of the procedure performed (e.g., “tonsillectomy and adenoidectomy”) and the accompanying diagnosis (e.g., “chronic tonsillitis”). Following the transition to payments based on coding, the purpose of which “is to provide a uniform language that will accurately describe medical, surgical, and diagnostic services” (16), practices have been required to select the most appropriate CPT procedure code (e.g., 42820, for tonsillectomy and adenoidectomy, younger than age 12) and the most appropriate ICD diagnosis code (e.g., 474.02, for chronic tonsillitis and adenoiditis).
Resources for Compliant Coding and Documentation (publications are available through various medical and compliance organizations)
CPT: Current Procedural Terminology” (procedure codes, including E/M codes)
“CPT Assistant” (periodical, which publishes explanations and clarifications of CPT codes and instructions)
“International Classification of Diseases, ICD-9-CM” (diagnosis codes)
“HCPCS Level 2” (additional procedure codes)
“Documentation Guidelines for Evaluation and Management Services,” 1995 and 1997 editions (Evaluation and Management Documentation principles)
“Medicare RBRVS: The Physicians’ Guide” (Medicare RVUs and payments, global periods, assistant at surgery restrictions, cosurgeon adjustments)
“CPT Reference of Clinical Examples” (AMA scenarios for correct coding of procedures and E/M services)
“National Correct Coding Initiative (NCCI) Edits” (Medicare scenarios for correct coding of procedures)
Resources for Compliance in Otolaryngology— Head and Neck Surgery (Available through the American Academy of Otolaryngology—Head and Neck Surgery)
AAO-HNS Clinical Indicators Compendium: http://www.entnet.org/Practice/clinicalIndicators.cfm
AAO-HNS Policy Statements: http://www.entnet.org/Practice/policystatements.cfm
AAO-HNS Clinical Practice Guidelines and Clinical Consensus Statements: http://www.entnet.org/Practice/clinicalPracticeguidelines.cfm
Although physician practices and hospitals view procedure and diagnosis coding almost exclusively through the lens of its role in reporting claims for proper payment, these codes also play additional roles in improving health care. CPT advises that its procedure code functions extend to “the development of guidelines for medical care review… to medical education and outcomes, health services, and quality research by providing a useful basis for local, regional, and national utilization comparisons” (16). ICD-9-CM codes are a United States “clinical modification” of the World Health Organization’s International Classification of Disease. Its published intent is “to serve as a useful tool to classify morbidity data for indexing medical records, medical care review, and ambulatory and other medical care programs, as well as for basic health statistics” (17). These functions provide the foundation for some of the goals for system-wide use of EHRs, which are intended to facilitate the collection of coded information about symptoms and diseases, including the relative success of various procedures used to diagnose and treat them.
While these coding benefits promise to advance medical science and improve population health, the primary impact of coding on practicing U.S. physicians is accurate submission of claims to obtain correct payment in a timely manner. Reliable coding for payment depends on accurate documentation, and these demands will increase with the greater coding specificity being introduced in 2014 with the transition to ICD-10 diagnostic codes.
Integrating Coding and Billing Principles into Documentation and Patient Care
Commonly underemphasized or even overlooked in discussions of coding and billing practices, the critical factors in achieving compliant coding and documentation are specificity and medical necessity.
Specificity
Specificity is a central feature in identification of correct procedure codes, E/M codes, and diagnosis codes. CPT, the guide for procedure codes, instructs physicians to
“Select the name of tghe procedure or service that accurately identifies the service performed. Do not select a CPT code that merely approximates the service provided. If no such specific code exists, then report the service using the appropriate unlisted procedure or service code. In surgery, it may be an operation; in medicine, a diagnostic or therapeutic procedure; in radiology, a radiograph… Any service or procedure should be adequately documented in the medical record” (18).
“Select the name of tghe procedure or service that accurately identifies the service performed. Do not select a CPT code that merely approximates the service provided. If no such specific code exists, then report the service using the appropriate unlisted procedure or service code. In surgery, it may be an operation; in medicine, a diagnostic or therapeutic procedure; in radiology, a radiograph… Any service or procedure should be adequately documented in the medical record” (18).
These instructions not only underscore the need for specificity in identifying correct codes, they highlight the direct compliance link between coding and documentation. Physicians must have an appreciation and understanding of procedure codes in order to ensure that their documentation supports (i.e., verifies) that the procedure being coded was, in fact, performed. The potential hazards of nonspecific documentation and noncompliant coding are emphasized below.
Specificity is similarly a central feature in identification of correct diagnosis codes. ICD-9, the current guide for diagnosis codes, instructs physicians to
“Describe the patient’s condition using terminology that uses specific diagnoses as well as symptoms, problems or reasons for the encounter. If symptoms are present but a definitive diagnosis has not been determined, code the symptoms… Determine whether the code is at the highest level of specificity. Assign three digit codes (category codes) if there are no four-digit codes within the code category. Assign four-digit codes (subcategory codes) if there are no five-digit codes for that category. Assign five-digit codes (fifth digit subclassification codes) for those categories where they are available” (19).
Medical Necessity
Medical necessity introduces the concepts of “standards of care” and, more recently, “evidence-based medicine” (EBM) into correct billing practices. Physicians are comfortable considering the medical indications for ordering tests, diagnostic procedures, medical treatments, and therapeutic procedures. Medical necessity is the parallel terminology used as a prime determinant for appropriate payment in insurance reviews. (This concept may also carry considerable weight in evaluations of quality care or professional liability.) Physicians commonly assume that their personal decision to provide various levels of office care, perform diagnostic or therapeutic procedures, or order certain diagnostic tests automatically qualify as a certification of medical necessity. In response to concerns about some of these decisions, Medicare and private insurers elected to establish and apply their own standards of medical necessity, at times using them as a basis for denying payment for correctly coded services. The resultant conflicts, appeals, and failure to have a common understanding of this concept between physicians and insurers became one of the pivotal issues in the national class action lawsuits filed by physician organizations against health insurers in the first decade of the 21st century (20). The negotiations on this issue prompted the AMA and its affiliated specialty organizations to promulgate a definition of medical necessity that, with modifications during the negotiations, has become an established standard applied by physicians and insurers alike:
“‘Medically Necessary’ or ‘Medical Necessity’ shall mean health care services that a physician, exercising prudent clinical judgment, would provide to a patient for the purpose of preventing, evaluating, diagnosing or treating an illness, injury, disease or its symptoms, and that are: (a) in accordance with generally accepted standards of medical practice; (b) clinically appropriate, in terms of type, frequency, extent, site and duration, and considered effective for the patient’s illness, injury or disease; and (c) not primarily for the convenience of the patient, physician, or other health care provider, and not more costly than an alternative service or sequence of services at least as likely to produce equivalent therapeutic or diagnostic results as to the diagnosis or treatment of that patient’s illness, injury or disease. For these purposes, “generally accepted standards of medical practice” means standards that are based on credible scientific evidence published in peer-reviewed medical literature generally recognized by the relevant medical community, Physician Specialty Society recommendations and the views of physicians practicing in relevant clinical areas, and any other relevant factors” (21).
The introduction of the word “relevant” in multiple portions of this definition addressed concerns in broad language commonly found in insurer contracts that gave carriers wide latitude to consider any factors they chose. (Note: This definition’s compromise language concerning relative cost of alternative services raises concerns about patients’ rights to choose their care, even if more costly, under the doctrine of informed consent. While this notion could raise issues between patients and their insurers, physicians must be aware of the potential for insurers to deny payment for more costly service options; under such circumstances, it is advisable that they seek approval for payment prior to initiating such care.)
Fundamental Precepts of Billing, Coding, and Documentation
Three fundamental principles of medical record auditing provide the insight physicians need to understand correct billing and coding and to conceptualize their requirements for properly designed documentation tools needed to facilitate compliant coding while promoting optimal patient care:
Medicare stipulates, “Medical necessity of a service is the overarching criterion for payment in addition to the individual requirements of a CPT code” (22).
This statement reflects criteria in section 1862 of Social Security Law that stipulate, “no payment may be made under (Medicare) part A or part B for any expenses incurred for items or services which… are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member” (23).
Finally, in its section reviewing payment for E/M services, the Trailblazer MAC’s website further clarifies, “Federal law requires that all expenses paid by Medicare, including expenses for Evaluation and Management (E/M) services, are ‘medically reasonable and necessary’… Medicare’s determination of medical necessity is separate from its determination that the E/M service was rendered as billed… At audit, Medicare will deny or downcode E/M services that, in its judgment, exceed the patient’s documented needs” (24).
“If medical care is not documented in the medical record, it is treated as if it had not been performed.” (25)
Although this statement is no longer found in the current CMS Carriers’ Manual, it was obtained from section 7103.1(i) of an older version. Related language also appears on the Trailblazer MAC website, reporting that an error in coding occurs when “Documentation is incomplete/insufficient: (i.e.,) documentation does not support the level of service billed” (26).
“Automation is not documentation” (27).
Preloaded generic clinical information that is copied and inserted from previous encounters (copy forward), from preloaded macros (copy/paste) or created by filling in multiple check boxes with a single click (documentation by exception) fail to record individualized clinical information related to each patient and each encounter. Although the use of automated data entry is most frequently found in suboptimal designs for EHRs, similar functionality has found its way into dictated operative reports and E/M records with distressingly increasing frequency.
Reviewing records created with automated documentation reveals that physicians using this approach almost always undocument and redocument only the clinical information that is relevant to their patient’s presenting illness. Because of the automated defaults to “normal findings,” all other aspects of the patient’s health almost always appear in the completed H&P as normal—a circumstance that is not compatible with the reality of most patients’ health status. In other words, such “cloned records” attempt to give the impression that the physician performed comprehensive care, when in fact the repetitive “normal” findings in history and examination related to other organ systems attest to the fact that the physician performed and accurately documented only problem-focused care.
As noted above in the box reporting a “final verdict” on cloned documentation, automated documentation consistently fails to provide both of the critical factors needed for compliant coding and documentation: it is insufficient to record the specificity required for individualized clinical information, and it is therefore “considered a misrepresentation of the medical necessity requirement for coverage of services” (28).
Fortunately, these three auditing principles can be transformed into three powerful core documentation principles that physicians can employ to ensure compliant documentation, coding, and billing:
When (patient-specific and visit-specific) care is documented, it was done.
When care is medically necessary, and that necessity is documented in the medical record, payment must be made.
Nonautomated (i.e., individually documented) records promote compliance and can also enhance quality of care.
DESIGNING MEDICAL RECORDS TO MEET PHYSICIANS’ NEEDS
These three documentation principles can be used as cornerstones for medical record designs that meet all of physicians’ requirements for effective documentation and coding tools:
Usability: Ease of data entry with options to use multiple data entry modalities—dictation, legible handwriting, and/or keyboard and mousec
Efficiency: Completing care and individualized documentation in a reasonable time frame without sacrificing compliance or data integrity
Compliance: For both procedure and E/M records, the documentation should verify specific details of what was performed and the medical necessity of performing that care.
Data integrity: The documented record should clearly and easily convey all the care performed and the reasons why it was performed (to another physician, to a reviewer, and most importantly to the physician himself/herself during subsequent visits).
Promoting quality patient care: During E/M services, compliance-based documentation tools follow the diagnostic paradigm taught to physicians from the Bates’ Guide; this facilitates providing levels of care warranted by the NPPs during each encounter.
Appropriate productivity: Care, documentation, coding, and billing are all achieved at medically indicated levels, which the physician determines and sets based on his or her assessment of medical necessity.
Compliant Designs for Documenting Operative Procedures
While surgeons have been dictating operative reports for many years, the traditional approach commonly includes only demographic information, preoperative and postoperative diagnoses, the name(s) of the operation(s) performed, and a free-text narrative of the procedure. However, the operative note frequently fails to provide an explanation of the medical indications (i.e., the medical necessity) for performing the procedure. More recently, some physicians have also sought to save time in creating their operative reports by instructing their transcriptionists to insert generic macros to describe the procedure performed, in lieu of individualized dictation. This effort to save dictation time and costs illustrates the danger of replacing documentation with automation: every operation for every patient reads almost exactly the same, thereby sacrificing specificity.
These deficits can be remedied. Medical necessity should be documented by adding a section for “indications” near the beginning of the report. Here the physician dictates a narrative description of the clinical rationale warranting the performance of the surgical procedure. Specificity for the significant observations made during the course of the operation should be documented by dictating individualized narrative descriptions of the steps in the procedure and insertion of an additional section labeled “Operative Findings.” This section conveys the nuances of the operation and significant anatomic findings and challenges. For example, when dictating a tonsillectomy, the surgeon can document whether significant scar tissue or aberrant blood vessels were found in the dissection plane of each of the two tonsils, as well as the approximate amount of bleeding and how readily it was controlled. Figure 200.1 illustrates a sample template for operative procedures, including sections to document indications and operative findings.
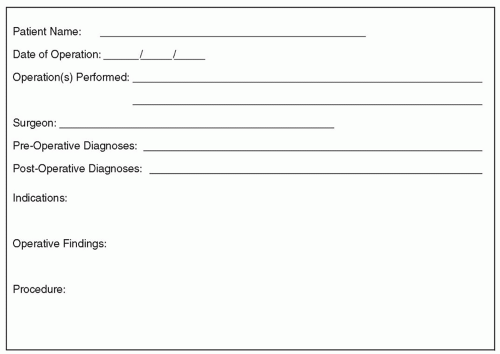 Figure 200.1 Sample operative report for operating room procedures. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


