16 Clinical Pearls in Endoscopic Pituitary Surgery: A Neurosurgeon’s Perspective
The endoscopic endonasal approach to the sellar region is an evolution of the classical microsurgical transsphenoidal technique.1 It is no longer considered a complement to microscopic surgery; rather, it has become “fully” endoscopic skull base surgery as the procedure is performed with the endoscope being the only optical device used to visualize the surgical target area.
The standard endoscopic endonasal approach to the sellar region has several benefits2,3:
• It avoids the need for the oral and the rhinoseptal submucosal nasal route; the special features of the telescopes used in this approach allow for a wider exposure of the operating field including the options of advancing toward the anatomical target area or inspecting the sphenoid sinus, sellar, supra-parasellar, and retroclival regions via a wide-angle panoramic view; the high-resolution close-up view of the anatomical structures enables a lesion arising from or involving such areas to be removed more safely, which, in turn, contributes to a reduced incidence of overall complications.
• It provides an improved postoperative course with less discomfort for the patient because there is no need to use the nasal speculum, and thus the risk of trauma to nasofacial structures is reduced. It avoids the need for postoperative nasal packing, thus minimizing breathing difficulties and discomfort for the patient.
• It reduces the duration of hospitalization and, therefore, the costs.
This approach includes the following steps, which involve a learning curve for the physician.4 Acquiring the technique requires in-depth anatomical training to become familiar with the endoscopic view of the different nasal structures; this is dependent on the acquisition of specific endoscopic skills.5 Use of specific instrumentation facilitates the readjustment process, but it takes times to achieve proficiency with the two-dimensional image provided by the endoscope. For instance, when first attempted, the restricted sensory feedback and loss of depth perception can cause slowing of surgical dexterity; a temporary difficulty in the hand-eye coordination abilities of the surgeon is usually noticeable. This temporary difficulty is overcome as the surgeon becomes increasingly confident viewing through a video monitor versus microscope oculars that are focused in the same direction as one’s own hands.
 Operating Room Setup and Patient Positioning
Operating Room Setup and Patient Positioning
In the operating room, all of the equipment needed or recommended for the endoscopic surgery, that is, the cold light source, video camera, monitor, and video recording system, are placed ergonomically behind the head of the patient and in front of the operating surgeon, who is at the right side of the patient. The anesthesiologist and equipment are positioned at the left side of the patient at the level of the head. The second surgeon is at the left side of the patient, and the scrub nurse stays at the level of the patient’s legs.
The use of image-guidance systems (IGSs), or neuronavigation, during the standard endoscopic approach is currently reserved for selected cases only, for example, patients with a conchal-type sphenoid sinus, or in certain recurrent cases previously operated transsphenoidally, or in patients with large lesions involving the para-suprasellar areas. When IGS is used, its monitor is usually put on the side of the main endoscopic monitor to allow the surgeon to see them both simultaneously.
The design of the operating room should reflect the philosophy of a team approach, and a dedicated integrated operating room helps to optimize teamwork and improve patient care.6
The patient’s neurodiagnostic studies are reviewed. Besides the standard sellar contrast-enhanced magnetic resonance imaging (MRI), a computed tomography (CT) scan with coronal reconstructions has proven to be quite useful to show the relevant nasal structures involved in the procedure—the nasal septum and turbinates. Furthermore, the neurodiagnostic studies are of the utmost importance for studying the individual anatomical configuration of the sphenoid sinus septum, because they may help the surgeon’s orientation while operating in the sphenoid sinus. Once the surgeon has gained sufficient confidence working with the endoscopic anatomy of the posterior wall of the sphenoid sinus or if the MRI scan already shows all septations inside the sinus, the preoperative CT scan of the nasal cavities may be no longer required.
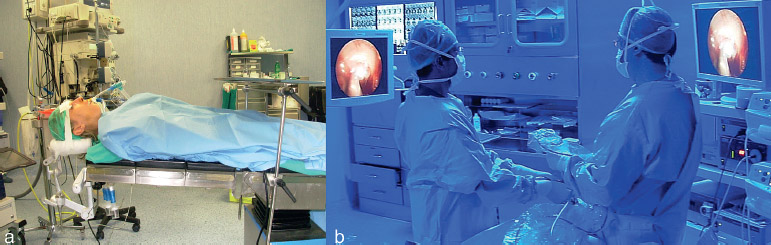
Fig. 16.1 Operating room setup. (A) Patient positioning. (B) Position of surgeons during the operation.
During the endoscopic approach to the sellar area the patient is positioned supine on the operating table with the trunk raised 10 degrees, and the head is placed in neutral position rotated 10 degrees toward the surgeon (Fig. 16.1A). The head is adequately secured in a horseshoe headrest without rigid three-pin fixation. The height of the table is adjusted so that the surgeon can work comfortably without having to hyperflex or extend the arms (Fig. 16.1B). The use of the Foley urinary catheter is not mandatory; however, it should be used if the operation is foreseen to last for more than 3 hours. The patient’s body except for the neck and the face is covered with a thermal blanket. The eyes are protected with antibiotic eye ointment and covered with adhesive bandages to minimize the risk of injuries from use of the Betadine solution during the prepping of the nose and face.
 Nasal Cavity
Nasal Cavity
The operation can be performed through a single nostril. When a bi-nostril approach is performed, two or three operating instruments, depending on the specific needs and circumstances, plus the endoscope can be inserted through both nostrils, thus providing increased working space and improved maneuverability.4
Using a small Killian-type nasal speculum, cotton pledgets soaked in 50% polyvidone-iodine are placed along the floor of the nasal cavities and in the space between the nasal septum and the turbinates. They are allowed to take effect for approximately 5 minutes. We advise not using pure polyvidone-iodine antiseptic solution because it may irritate the nasal mucosa.
Before starting the surgical procedure, each component of the endoscopic apparatus (monitor, video camera, light source, light cable, endoscope, irrigation system, recording system, etc.) should be checked to be sure it is functioning correctly; the white balance of the video camera should also be checked.
During the first part of the procedure, a 0-degree telescope, 4 mm in diameter, 18 cm in length, is used freehand. Once the scope is introduced parallel to the floor of the nasal cavity, the first structure to come into view is the inferior turbinate. The scope is advanced along the floor of the nasal cavity, passing between the posterior end of the inferior turbinate and the nasal septum, to reach the choana, which is the true anatomical landmark of this step of the procedure and where the eustachian tube opens. The middle turbinate is above and posterior to the head of the inferior turbinate. In some cases, its head may be variously pneumatized (concha bullosa). Cotton pledgets, soaked in diluted adrenaline (1/10,000, 1:20 dilution) or xylometazoline hydrochlorate, are placed in the space between the middle turbinate and the nasal septum to achieve a vasoconstriction of the nasal mucosa (Fig. 16.2). The anesthesiologist should be notified of the use of the adrenaline as it might increase the patient’s blood pressure and heart rate.
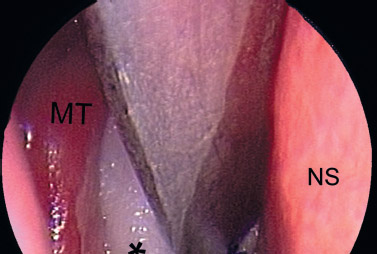
Fig. 16.2 Nasal step. Right nasal cavity. A cotton pledget soaked with diluted adrenaline protects the middle turbinate when pushing it laterally. MT, middle turbinate; NS, nasal septum; asterisk, cotton pledget.
The middle turbinate is gently lateralized to widen the space between the nasal septum and the turbinate itself. Moving the endoscope forward between the middle turbinate and nasal septum, at a 30-degree upward angle relative to the floor of the nasal cavity, the sphenoethmoid recess is reached, extending between the roof of the choana and the natural sphenoid ostium (Fig. 16.3A). Such ostium varies in size and cannot always be viewed, as it may be hidden by the tail of the superior or the supreme turbinate. At this point, it is not necessary to visualize the sphenoid ostium because access to the sphenoid cavity can be gained by proceeding from the choana slightly upward for approximately 1.5 cm along the sphenoethmoid recess.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


