Examination |
Test Performance |
Outcome |
Interpretation of Clinical Finding |
Spontaneous nystagmus |
Static visual fixation |
Nystagmus waveform, direction, effect of fixation |
Peripheral: Horizontal-rotary jerk nystagmus, suppresses with visual fixation
Central: direction changing, horizontal, vertical, torsional, or pendular nystagmus, enhances with visual fixation |
Gaze-evoked nystagmus |
<30° eccentric gaze |
Nystagmus waveform, direction |
Peripheral: Direction-fixed nystagmus, increases while gazing in the direction of the fast phase (Alexander law)
Brainstem or cerebellum: Direction-changing nystagmus, fast-phase movement in the direction of gaze, or rebound nystagmus in neutral gaze
CPA mass: Brun nystagmus (direction-changing nystagmus caused by a combination of central GEN and vestibular nystagmus) |
Saccades |
Alternate fixation on two stationary targets |
Accuracy, conjugate movement, velocity, and initiation |
Peripheral: normal. Abnormalities indicate a central etiology |
Smooth pursuit |
Track visual target |
Smooth versus jerking eye movements |
Normal in peripheral vestibular pathology. Abnormalities (e.g., catch-up saccades) indicate a central etiology |
Fixation suppression |
Rotate examination chair ± visual fixation |
Effect of fixation on rotation-induced nystagmus |
Normal fixation suppression in peripheral pathology. Failure of fixation suppression suggests central (floccular) dysfunction |
Head impulse test (HIT) |
Rotational head thrusts while maintaining visual fixation |
Refixation saccade |
Peripheral vestibular dysfunction: Refixation saccade generated with rotational head thrusts toward the weak side |
Head heave test (HHT) |
Linear head heaves while maintaining visual fixation |
Refixation saccade |
Otolith damage: Refixation saccade generated with linear head heaves toward the damaged side |
Postheadshake nystagmus |
Headshake |
Nystagmus direction |
Asymmetric peripheral damage: nystagmus (in plane of damaged canal with fast phase toward stronger ear).
Central: cross-coupling of nystagmus |
Dynamic visual acuity (DVA) |
Visual acuity (static vs. head movement) |
Visual acuity decline |
Peripheral vestibular dysfunction: Visual acuity decline (>2 lines on Snellen chart) |
Positional testing |
Various static head positions |
Nystagmus onset, direction, duration, effect of fixation |
Peripheral: Severe vertigo, transient, and usually direction fixed. Removing visual fixationa enhances nystagmus
Central: Usually asymptomatic, persistent, direction changing, and may be disconjugate. Removing visual fixationa improves nystagmus |
Positioning testing |
Head movement to various head positions (e.g., Dix-Hallpike) |
Nystagmus latency, direction, duration, fatigability, reversal |
Peripheral: see Table 165.4 for details of posterior, horizontal, and superior semicircular canal BPPV.
Central: Immediate (no latency), persists >1 min, no reversal nystagmus, no fatigue, direction changing, no vertigo |
Limb coordination tests |
Limb coordination testsb |
Limb coordination. Arm drift with past pointing |
Peripheral (vestibulospinal): All limb coordination tests, except past pointing, are normal Past pointing: excessive arm drift toward side of peripheral lesion.
Central: abnormalities in any of the tests |
Gait |
Tandem gait, Unterberger (Fukuda) stepping test |
Gait abnormalities. Rotation with stepping |
Peripheral: Abnormal tandem gait with eyes closed, rotation to side of lesion with stepping test.
Central: Gait abnormalities (e.g., ataxia, shuffling, etc.) |
Posture |
Romberg tests |
Excessive sway and fall |
Peripheral: Fall on tandem and foam Romberg tests (eyes closed) |
Mastoid vibration |
Vibration source on mastoid |
Nystagmus direction |
Nystagmus in the plane of the affected canal toward the stronger ear |
Malleolar sign |
256-Hz tuning fork on malleolus |
Conductive hyperacusis |
Patient hears tuning fork vibration on side of superior canal dehiscence |
Pressure-evoked eye movements |
Tragal compression, pneumatic otoscopy, Valsalva maneuvers |
Eye movement, vertigo |
Perilymph fistula, otic syphilis, or semicircular canal dehiscence |
Sound-evoked eye movements |
Pure tones (≈ 100 dB) |
Eye movement, vertigo |
Perilymph fistula, otic syphilis, or semicircular canal dehiscence |
Hyperventilationinduced nystagmus |
Hyperventilate for 90 s |
Nystagmus direction |
Peripheral: excitatory nystagmus toward affected earc |
In CNS demyelinating diseases. |
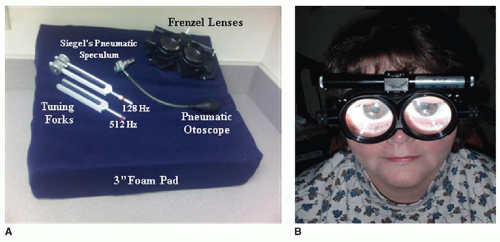
a Frenzel lenses and infrared video goggles remove visual fixation. |
b Finger-to-nose, finger-nose-finger, hand rapid alternating movement test, fine finger movements, heel-to-shin, past pointing test. |
c Hyperventilation-induced nystagmus may also occur. |
BPPV, benign paroxysmal positional vertigo; CPA, cerebellopontine angle. |