Clinical Applications of Topical Ophthalmic Antibiotics-A Comprehensive Review Including Mechanisms of Action and Adverse Effects of New and Long-Standing Pharmaceuticals
Renée Solomon
Eric Donnenfeld
BACTERIAL CONJUNCTIVITIS
Bacterial conjunctivitis is common, generally mild to moderate in severity, and usually self-limiting.1 Treatment with topical ophthalmic antibiotics speeds resolution of the disease, decreases morbidity, prevents recurrence and spread of the disease to social contacts, decreases the incidence of permanent conjunctival changes, decreases the risk of corneal or intraocular infection when surgery is anticipated, and prevents the development of chronic conjunctivitis with its greater treatment challenges and risk of progression to corneal damage or disease.2, 3 and 4 The most frequently isolated pathogens in acute bacterial conjunctivitis are Streptococcus pneumoniae and Haemophilus influenzae in pediatric patients and Staphylococcus epidermidis in adult patients.5, 6
Chronic conjunctivitis is defined as any case of conjunctivitis that lasts longer than 2 weeks. The most common pathogens associated with this condition are Staphylococcus aureus and S. epidermidis, the most common organisms found in normal lid and conjunctival flora. These pathogens produce toxins that can damage the conjunctiva and cornea, producing the superficial punctate keratopathy that is commonly seen. The punctate keratopathy characteristically involves the inferior cornea and conjunctiva. These organisms also commonly spread to other ocular structures, such as the meibomian orifices, lash follicles, and the lacrimal canaliculi, and may even breach the corneal epithelium.2, 3
Other, more serious types of infectious conjunctivitis include hyperacute bacterial conjunctivitis, usually caused by Neisseria gonorrhoeae and S. pneumoniae. N. gonorrhoeae is often associated with oropharyngeal infections and requires systemic and topical therapy.2, 3
In the treatment of acute bacterial conjunctivitis, most physicians do not perform cultures, and therefore prescribe broad-spectrum antibiotic agents. Because bacterial conjunctivitis is usually self-limiting, agents associated with a higher incidence of ocular toxicity or hypersensitivity reactions are best avoided. Combination products with gram-positive and gram-negative coverage are popular for their broad spectrum of activity, but some contain agents that can be irritating or cause allergic reactions. Patient compliance is a common treatment challenge, particularly in pediatric patients, because they are reluctant to let anyone instill anything into their eyes and are sensitive to irritating agents.
BACTERIAL KERATITIS
Bacterial keratitis is an ophthalmic emergency that has the potential to cause significant vision loss secondary to corneal scarring and perforation. Rapid diagnosis and immediate treatment with appropriate antimicrobial therapy are necessary to limit the extent of tissue damage and to improve the visual prognosis.3, 4, 5, 6 and 7 Approximately 30,000 cases of microbial keratitis are diagnosed each year in the United States.8 The most likely causative organisms depend on geographic location, preexisting corneal disease, urban or rural environment, history of contact lens wear, and climate.9, 10, 11, 12 and 13
Approximately 87% of all cases of bacterial keratitis in the United States result from infection by one of the following organisms: gram-positive infections are most commonly secondary to streptococci or staphylococci, whereas the gram-negative organisms include Pseudomonas sp. or Enterobacteriaceae (especially Serratia marcescens but also Citrobacter, Klebsiella, Enterobacter, and Proteus sp.).14, 15 and 16 Currently, the most common causes of microbial keratitis are Staphylococcus aureus in the northern United States and Pseudomonas and Streptococcus sp. in the southern United States.3, 11, 17 Streptococcus pneumoniae is the most common pathogen in many developing countries. Staphylococcus sp. are the most common organism associated with photorefractive keratectomy or LASIK.18 Pseudomonas sp. are frequently associated with overnight contact lens wear, but may also be seen with daily-wear contact lenses.19, 20, 21, 22, 23, 24, 25, 26 and 27 In fact, Pseudomonas sp. have become a more common cause of bacterial keratitis in the southern United States than Staphylococcus aureus.28, 29 In children younger than 3 years, Pseudomonas sp. have been identified as the most common bacterial cause of keratitis.30, 31
Many ophthalmologists diagnose and treat bacterial keratitis on the basis of their empirical observations and only perform a microbial analysis on particularly severe ulcers (e.g., those encroaching on or involving the visual axis). Most physicians choose what they think to be a broad-spectrum antibiotic and begin treatment immediately,3, 32, 33 but the choice of agent may also be influenced by which pathogen is suggested by the disease presentation and the physician’s knowledge of pathogen prevalence in the local environment and patient population.28, 34, 35 and 36 Care must be taken in the choice of a broad-spectrum antibiotic because certain commercially available agents may have significant gaps in the spectra of their antimicrobial efficacy, may poorly penetrate the cornea, or may be bacteriostatic rather than bactericidal. Any of these characteristics would make them unsuitable for the treatment of bacterial keratitis.
For approximately 25 years, the mainstay for the treatment of these infections has been dual therapy using topically administered fortified antibiotics.37 These antibiotics are not commercially available and are specially formulated by hospital pharmacies or physicians when needed. Traditionally, one antibiotic provided coverage against gram-negative pathogens (an aminoglycoside such as tobramycin or gentamicin [13.6 mg per mL]), and the second antibiotic covered the spectrum of gram-positive bacteria (vancomycin [25 mg per mL], cefazolin [50 mg per mL], or bacitracin [10,000 U per mL]). Together, they provided an initial empirical regimen for the treatment of bacterial keratitis. During the past several years, the fluoroquinolone family of antibiotics has offered an alternative to fortified antibiotics as the mainstay of treatment for bacterial ulcerations. Two double-masked, controlled, clinical trials have supported the clinical efficacy of using the commercially available fluoroquinolones (ofloxacin 0.3% or ciprofloxacin 0.3%) as compared with fortified tobramycin and cefazolin.38, 39
There are various routes for administering antibiotics in the treatment of ocular infections and they include topical, subconjunctival, oral, intravenous, and intramuscular. Topical application of antibiotics is the preferred route of administration for bacterial conjunctivitis and keratitis because the drops provide therapeutically effective concentrations; the drops wash away bacteria and bacterial antigens; adverse systemic effects of the drugs are decreased or eliminated; and in reliable patients, they can be administered on an outpatient basis.40, 41, 42 and 43 The factors that contribute to achieving effective therapeutic concentrations of the drug in the cornea include the frequency of administration, the concentration of the drug, the lipophilic nature of the drug where the epithelium is intact, the length of contact time of the drug with the cornea, and the lack of an intact corneal epithelium.44, 45 The next section deals with the individual characteristics of the various topical ophthalmic antibiotics used to treat bacterial conjunctivitis and keratitis.
PROPERTIES OF TOPICAL OPHTHALMIC ANTIBACTERIAL AGENTS
Fluoroquinolones
Chemistry, Ophthalmic Preparation, and Pharmacologic Action
The fluoroquinolones, the newest class of agents to be developed, are based on the prototype nalidixic acid (1,8-naphthyridine), which was synthesized in 1962.46
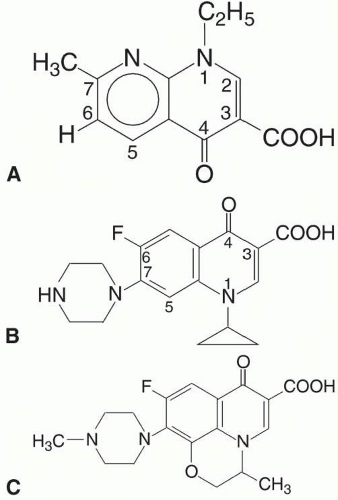 FIG. 39.1 Chemical structure of the nalidixic acid (A) from which the fluoroquinolones, including ciprofloxacin (B) and ofloxacin (C), were derived. |
In the 1980s, the fluoroquinolones were created from nalidixic acid by adding a fluorine atom to position 6 of the molecule (Fig. 39.1). This addition widened the antibacterial spectrum of activity and resulted in decreased development of resistant organisms. The newer fluoroquinolones available for ophthalmic use include gatifloxacin ophthalmic solution 0.5% (Zymaxid, Allergan, Inc., Irvine, California), gatifloxacin 0.3% (Zymar, Allergan, Inc.), moxifloxacin HC1 ophthalmic solution 0.5% (Moxeza, Alcon Laboratories, Inc., Fort Worth, Texas), moxifloxacin 0.5% (Vigamox, Alcon Laboratories, Inc.), besifloxacin ophthalmic suspension 0.6% (Besivance, Bausch and Lomb, Rochester, New York), levofloxacin ophthalmic solution 1.5% (Iquix, Vistakon Pharmaceuticals, LLC, Jacksonville, Florida), and levofloxacin ophthalmic solution 0.5% (Quixin, Vistakon Pharmaceuticals, LLC). In addition to the fluoroquinolone eyedrops, there is a fluoroquinolone ophthalmic ointment, ciprofloxacin (Ciloxan, Alcon Laboratories, Inc.), and generic formulations available of the prior-generation fluoroquinolones, ofloxacin and ciprofloxacin. The previous-generation fluoroquinolones predominantly either inhibit topoisomerase II (DNA Gyrase) or topoisomerase IV and, therefore, only require one genetic mutation for bacteria to develop resistance.47 Fourth-generation fluoroquinolones are equally effective against bacterial topoisomerases II and IV, which significantly expands their spectrum of action against gram-positive agents and atypical mycobacteria and Nocardia.48, 49 This duality of action of the fourth-generation fluoroquinolones requires that for bacteria to become resistant to these agents, the bacteria must undergo two genetic mutations resulting in a significantly decreased chance of an organism developing resistance.50 The fluoroquinolones are bactericidal by interfering with bacterial DNA replication, transcription, repair, and recombination.
Gatifloxacin differs from the prior-generation ciprofloxacin in two positions, but the enhanced activity of the molecule compared with ciprofloxacin is due to a methoxy group at the 8-position of the fluoroquinolone structure. Moxifloxacin has the same group at the 8-position, but differs from gatifloxacin at the 7-position of the molecule. The 8-methoxy substitution yields a better coverage against gram-positive organisms, including resistant strains, while preserving the similar coverage against gram-negative organisms seen in prior generations of fluoroquinolones.51
Clinical Experience and Ophthalmic Uses for the Individual Ophthalmic Preparations of the Fluoroquinolones
The ophthalmic fluoroquinolones are indicated for the treatment of conjunctivitis. However, because of their broad-spectrum antibacterial activity, they are also used to minimize the risk of postoperative endophthalmitis after cataract surgery, postoperative keratitis after keratorefractive procedures, and to treat bacterial keratitis.52 Minimum inhibitory concentrations determined in vitro suggest that fourth-generation fluoroquinolones are more effective than second- and third-generation fluoroquinolones against gram-positive bacteria, including Staphylococcus sp. found in endophthalmitis and bacterial keratitis cultures.50, 53 When selecting a fourth-generation fluoroquinolone, it is important to consider potency, ocular penetration, efficacy, and safety. In addition, the acute management of bacterial corneal ulcers requires rapid access to therapy. The cost and toxicity of antibiotic therapy must also be considered. Fortified antibiotics are not commercially available and must be prepared on request. The fluoroquinolones are superior with respect to accessibility, cost, and low toxicity. The fluoroquinolones perform at least as well as, and often better than, the aminoglycosides in the treatment of gram-negative corneal ulcers. Prompt, appropriate treatment decreases the length of time to eradication of the infection, minimizes the risk of sequelae, helps prevent the spread of infection, and reduces the time away from daily activities.
Since there are two ophthalmic formulations of gatifloxacin and moxifloxacin, and no current generic formulations, brand names will be used in this section. The commercial ophthalmic formulations of gatifloxacin, Zymar and Zymaxid, and the commercial formulation of besifloxacin contain the preservative benzalkonium chloride (BAK) 0.005%, whereas the commercial ophthalmic formulations of moxifloxacin 0.5%, Vigamox and Moxeza, contain no BAK. As noted, Zymaxid contains a higher concentration (0.5%) of the antibacterial agent gatifloxacin found in Zymar (0.3%). In addition, Iquix is also a preservative-free formulation.
Gatifloxacin Ophthalmic Solution
The addition of the methoxy group at the 8-position of the ring structure increased the potency against gram-positive bacteria by 4-fold from ciprofloxacin to gatifloxacin, resulting in a lower minimal inhibitory concentration (MIC). In comparing gatifloxacin with moxifloxacin, gatifloxacin was shown to be significantly more active against ocular isolates of P. aeruginosa with an MIC90 of 1.28 versus 2.60 mg/mL for moxifloxacin.54 In addition, gatifloxacin was demonstrated to have slightly better activity than moxifloxacin against some gram-negative pathogens. As noted, Zymar and Zymaxid are formulated with the preservative BAK. The preservative is frequently included to prevent contamination of the bottle that could be picked up by skin flora if the bottle comes in contact with the skin during instillation. In addition, the antibiotic formulation is not antifungal, but the Zymar and Zymaxid formulations are resistant to contamination by fungi. It has been reported that BAK in the Zymar and Zymaxid formulations may enhance their antibacterial activity as shown by more rapid killing and lower MICs.52
Moxifloxacin Ophthalmic Solution
Moxeza55 is a reformulation Vigamox with a new vehicle, xanthan gum, which supports BID labeling because the new formulation allows the antibiotic to remain on the eye longer and increases penetration into the ocular tissues. Moxeza is dosed two times per day for 7 days and is indicated for patients 4 months of age and older.
A multicenter, vehicle-controlled, randomized, doublemasked, parallel group study was conducted on Moxeza to evaluate in vivo safety and efficacy.55 The study group included clinically diagnosed bacterial conjunctivitis in 1,180 patients aged greater than 28 days (range 30 days to 92 years). Moxeza or its vehicle was dosed one drop twice daily for 3 days. Microbiologic specimens were obtained from affected eyes on day 1, prior to the initial dose, and on day 4 after 3 days of dosing. All recovered bacteria were identified to the species level. The microbiologic success rate for patients treated with Moxeza twice daily for 3 days was 74.5%, compared with 56.0% of patients treated with its vehicle control (P < .0001). Moxeza was also statistically more effective than vehicle in eradicating the three principle conjunctivitis pathogens, H. influenzae (98.5% vs. 59.6%, respectively), Streptococcus pneumoniae (86.4% vs. 50.0%, respectively), and Staphylococcus aureus (94.1% vs. 80.0%, respectively) (P < .001). This clinical study demonstrated that the use of Moxeza resulted in effective eradication of the three principal causative pathogens of bacterial conjunctivitis across all age groups when dosed twice daily for 3 days.55
As indicated by Tauber et al., the majority of topical ophthalmic antibiotic products approved in the United States for the treatment of bacterial conjunctivitis have a 7- to 10-day treatment regimen, totaling a minimum of 21 to 42 or more drops over a course of therapy. A full course of therapy with Moxeza is 14 drops over 7 days. Results from this Tauber’s demonstrate that Moxeza, when dosed topically twice daily for 3 days (total six drops per eye), was statistically superior to its vehicle in the percentage of patients classified as microbiologic successes after 3 days of treatment (75% vs. 56%, P < .0001). Moxeza was also significantly more effective than its vehicle in eradicating the three principle conjunctivitis pathogens. The eradication rate of H. influenzae was 98.5% for Moxeza versus 59.6% for its vehicle; Streptococcus pneumoniae was 86.4% for Moxeza compared with 50.0% for vehicle, and Staphylococcus aureus was 94.1% for Moxeza compared with 80.0% for vehicle.55 BAK alone has significant in vitro cytotoxicity to cultured ocular epithelial cells. As Moxeza is preservative-free, there is no risk of corneal toxicity that may occur secondary to the BAK preservative. With respect to the issue of the potential of enhanced potency of Zymar due to BAK, some have argued that the BAK does not enhance potency because it is rapidly diluted in the tear film, weakening its ability to enhance potency when it reaches the ocular surface. In addition, it has been pointed out that the less-concentrated ophthalmic formulation of moxifloxacin, Vigamox, does not need a preservative because of the intrinsic antibacterial and antifungal activities of its formulation.
Vigamox
Studies have demonstrated that moxifloxacin has enhanced ocular penetration. In vivo studies have demonstrated that the conjunctival concentration of one drop of moxifloxacin 20 minutes prior to a conjunctival biopsy was greater than one drop of gatifloxacin, levofloxacin, ciprofloxacin, and ofloxacin.56 In addition, the corneal concentration of moxifloxacin in the epithelium, stroma, and endothelium in a patient undergoing penetrating
keratoplasty was demonstrated to be higher than the concentration of gatifloxacin. A prospective, randomized, parallel, double-masked study of 50 patients undergoing cataract extraction were dosed preoperatively with Zymar or Vigamox every 10 minutes for four doses, beginning 1 hour prior to surgery. Mean concentrations measured in aqueous demonstrated that Vigamox achieved concentrations in aqueous humor 3.8 times greater than Zymar. The concentrations were 1.80 (±1.21) µg per mL for Vigamox and 0.48 (±0.34) µg per mL for Zymar. Furthermore, microbiologic dilution analyses of aqueous humor samples demonstrated that moxifloxacin was 4.9 times more microbiologically active against S. epidermidis (2.1 mg per mL) compared with gatifloxacin (0.4 mg per mL). The structure of moxifloxacin ophthalmic solution 0.5% may account for its enhanced penetration. Moxifloxacin is highly lipophilic and has high aqueous solubility at physiologic pH 9, or the enhanced penetration may be as a result of the higher concentration of moxifloxacin than the concentration of other agents with which it was compared.57
keratoplasty was demonstrated to be higher than the concentration of gatifloxacin. A prospective, randomized, parallel, double-masked study of 50 patients undergoing cataract extraction were dosed preoperatively with Zymar or Vigamox every 10 minutes for four doses, beginning 1 hour prior to surgery. Mean concentrations measured in aqueous demonstrated that Vigamox achieved concentrations in aqueous humor 3.8 times greater than Zymar. The concentrations were 1.80 (±1.21) µg per mL for Vigamox and 0.48 (±0.34) µg per mL for Zymar. Furthermore, microbiologic dilution analyses of aqueous humor samples demonstrated that moxifloxacin was 4.9 times more microbiologically active against S. epidermidis (2.1 mg per mL) compared with gatifloxacin (0.4 mg per mL). The structure of moxifloxacin ophthalmic solution 0.5% may account for its enhanced penetration. Moxifloxacin is highly lipophilic and has high aqueous solubility at physiologic pH 9, or the enhanced penetration may be as a result of the higher concentration of moxifloxacin than the concentration of other agents with which it was compared.57
Besifloxacin
Besifloxacin ophthalmic suspension 0.6% is a chlorofluoroquinolone formulation, which is also indicated for the treatment of bacterial conjunctivitis.58, 59 and 60 Besifloxacin was developed solely for ophthalmic use, eliminating the contribution to resistance development from the selective pressure of systemic use. It has potent broad-spectrum bactericidal activity, especially against multidrug-resistant isolates.61, 62 and 63 The ophthalmic formulations for besifloxacin and azithromycin contain DuraSite (polycarbophil, edetate disodium dihydrate, and sodium chloride) (InSite Vision, Alameda, California), a mucoadhesive polymer designed to prolong the drug’s residence time on the ocular surface.64 Besivance also contains 0.01% BAK as a preservative, a compound that has been shown to have bacteriostatic and bactericidal activities of its own.65, 66
Besifloxacin has been found to have good ocular penetration in monkeys, with rapid absorption and sustained concentrations in anterior ocular tissues through 24 hours after a single administration.67 In a study to determine the concentrations of besifloxacin, moxifloxacin, and gatifloxacin in human aqueous humor after topical instillation of commercially available besifloxacin ophthalmic suspension 0.6%, moxifloxacin ophthalmic solution 0.5%, and gatifloxacin ophthalmic solution 0.3%, it was determined none of fluoroquinolones tested would likely be therapeutically effective in the aqueous humor against the most frequently identified drug-resistant staphylococcal isolates from recent cases of postoperative endophthalmitis.68
Levofloxacin
Levofloxacin is the L-enantiomer of its racemate ofloxacin. It was developed to address the increasing bacterial resistance to ofloxacin. Iquix is indicated for the treatment of corneal ulcers by susceptible strains. Iquix has the highest concentration available for any ophthalmic antibiotic. Therefore, it would not be surprising that studies have shown that in the cornea, concentrations of levofloxacin were greater than those of gatifloxacin and moxifloxacin. Iquix has the highest aqueous solubility of the topically administered fluoroquinolones.69
Adverse Effects
The fluoroquinolones have low rates of adverse effects.70 The most frequently reported adverse events of Zymaxid were worsening of the conjunctivitis, eye irritation, dysgeusia, and eye pain. For Zymar, the most frequently reported adverse reactions occurring in 5% to 10% of patients were conjunctival irritation, increased lacrimation, keratitis, and papillary conjunctivitis. Less frequently reported reactions found in 1% to 4% of patients were chemosis, conjunctival hemorrhage, dry eye, eye discharge, eye irritation, eye pain, eyelid edema, headache, red eye, reduced visual acuity, and taste disturbance.
The most common side effects of Moxeza are eye irritation, fever, and conjunctivitis. The most frequently reported ocular adverse events secondary to the use of Vigamox found in 1% to 6% of patients were conjunctivitis, decreased visual acuity, keratitis, ocular discomfort, ocular hyperemia, ocular pain, ocular pruritus, subconjunctival hemorrhage, and tearing.
The ocular adverse events occurring from use of Iquix in 1% to 2% of patients included decreased/blurred vision, instillation site irritation/discomfort, ocular infection, and ocular pain/discomfort. The nonocular adverse events occurring in approximately 8% to 10% of patients were headache and taste disturbance. The most frequently reported adverse events, which occurred in 1% to 3% of patients, were transient decreased vision, fever, foreign body sensation, headache, transient ocular burning, ocular pain or discomfort, pharyngitis, and photophobia. Other reactions that were reported in less than 1% of patients included allergic reactions, lid edema, ocular dryness, and ocular itching.
With respect to Besivance, the most common adverse events in clinical trials were conjunctival redness, blurred vision, eye pain, eye irritation, eye pruritus, and headache, reported in approximately 1% to 2% of patients 1 year and older.71
In a randomized, masked, placebo-controlled animal study evaluating the anterior chamber toxicity of the two
topical ophthalmic formulations containing DuraSite (Besivance and Azithromycin), it has been determined that these two formulations are toxic to the anterior chamber. When injected into the anterior chamber, the following side effects were noticed: conjunctival injection, moderate limbal vascularity, and severe, diffuse corneal edema, corneal ectasia, and bullous keratopathy.72 Because of the corneal edema, the anterior chamber could not be viewed, but vital staining and histopathologic evaluation revealed glaucomatous and toxic damage in eyes given DuraSitebased medications, whereas the groups without the DuraSite polymer showed minimal changes. Two mechanisms of damage were identified in the eyes injected with Besivance or AzaSite: acute glaucoma and direct toxic reaction. The authors noted that besifloxacin and azithromycin are completely different classes of drugs, and that the concentrations of BAK are radically different in these two drugs, so they believe that it is reasonable to conclude that DuraSite is most likely responsible for the toxicity results. While further studies are warranted to determine whether these problems are of clinical importance, the authors concluded that DuraSite blocks the trabecular meshwork and may be additionally toxic when introduced as a large bolus. The authors recommended that until the safety of these medications is established with further studies using smaller injected volumes, there should be placement of a suture over a clear corneal wound if DuraSite-based medications are used.72
topical ophthalmic formulations containing DuraSite (Besivance and Azithromycin), it has been determined that these two formulations are toxic to the anterior chamber. When injected into the anterior chamber, the following side effects were noticed: conjunctival injection, moderate limbal vascularity, and severe, diffuse corneal edema, corneal ectasia, and bullous keratopathy.72 Because of the corneal edema, the anterior chamber could not be viewed, but vital staining and histopathologic evaluation revealed glaucomatous and toxic damage in eyes given DuraSitebased medications, whereas the groups without the DuraSite polymer showed minimal changes. Two mechanisms of damage were identified in the eyes injected with Besivance or AzaSite: acute glaucoma and direct toxic reaction. The authors noted that besifloxacin and azithromycin are completely different classes of drugs, and that the concentrations of BAK are radically different in these two drugs, so they believe that it is reasonable to conclude that DuraSite is most likely responsible for the toxicity results. While further studies are warranted to determine whether these problems are of clinical importance, the authors concluded that DuraSite blocks the trabecular meshwork and may be additionally toxic when introduced as a large bolus. The authors recommended that until the safety of these medications is established with further studies using smaller injected volumes, there should be placement of a suture over a clear corneal wound if DuraSite-based medications are used.72
The most commonly reported adverse effect from topical ciprofloxacin treatment is the formation of a white crystalline precipitate in approximately 17% of treated eyes.73, 74 and 75 This results from precipitation of the drug (formulated at pH 4.5), which is poorly soluble at the nearneutral pH of the tear film. The relationship between this precipitate and antibacterial efficacy is unknown. The precipitate resolves spontaneously without sequelae after cessation of the medication. Like the 0.3% solution, the ciprofloxacin ointment has also been shown to cause a white precipitate that resolves spontaneously without sequelae after discontinuing it. Other adverse effects from the ointment include burning, punctate epitheliopathy, blurred vision, and tearing.76
Extemporaneously Compounded Fortified Antibiotics
Extemporaneously compounded fortified antibiotic eyedrop preparations contain high concentrations that are usually prepared from products formulated for intravenous use. A typical treatment regimen might consist of a combination of a cephalosporin (e.g., 50 mg per mL cefazolin) for gram-positive bacteria coverage and an aminoglycoside (e.g., 13 mg per mL tobramycin, or gentamicin) for gram-negative bacteria coverage. However, these agents are not compatible when combined in the same solution and must be formulated separately and administered from different bottles. Another common extemporaneously fortified antibiotic is vancomycin 50 mg per mL.77 Most need to be refrigerated after dispensing to the patient, because, being derived from intravenous products, they do not contain a preservative. Instillation of the two agents must be separated by intervals of several minutes or more (e.g., 15 minutes might be ideal) to prevent washout of the first agent by the second. The high concentrations used in these preparations exacerbate their epithelial toxic potential. This is a special concern for the aminoglycosides.
In the treatment of bacterial keratitis, fortified cefazolin-aminoglycoside preparations are as effective as the fluoroquinolones ofloxacin and ciprofloxacin, but are more difficult to obtain and use. Not all pharmacies are equipped to formulate extemporaneously compounded agents, and not all pharmacists are familiar with the procedures.
There has been some debate in the literature as to the efficacy of using a collagen shield as a vehicle to absorb and deliver drugs. Advocates argue that collagen shields soak up antibiotics and continuously deliver them to the cornea for several hours, enabling higher concentrations to be delivered for longer periods of time. However, some studies have found that collagen shields are not more efficacious than using fortified antibiotics alone.78, 79 According to several other studies, collagen shields are labor intensive yet as effective in treating bacterial keratitis as frequent dosages of drops.80, 81, 82, 83 and 84
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


