Purpose
To evaluate the safety and tolerability of intraocular delivery of ciliary neurotrophic factor (CNTF) using an encapsulated cell implant for the treatment of macular telangiectasia type 2.
Design
An open-label safety trial conducted in 2 centers enrolling 7 participants with macular telangiectasia type 2.
Methods
The participant’s more severely affected eye (worse baseline visual acuity) received the high-dose implant of CNTF. Patients were followed for a period of 36 months. The primary safety outcome was a change in the parameters of the electroretinogram (ERG). Secondary efficacy outcomes were changes in visual acuity, en face measurements of the optical coherence tomography of the disruption in the ellipsoid zone, and microperimetry when compared with baseline.
Results
The ERG findings demonstrated a reduction in the amplitude of the scotopic b-wave in 4 participants 3 months after implantation (month 3). All parameters returned to baseline values by month 12 and remained so at month 36 with no clinical impact on dark adaptation. There was no change in visual acuity compared with baseline. The area of the defect as measured functionally by microperimetry and structurally by the en face OCT imaging of the ellipsoid zone loss appeared unchanged from baseline.
Conclusions
The intraocular delivery of CNTF in the encapsulated cell implant appeared to be safe and well tolerated in eyes with macular telangiectasia type 2. Further evaluation in a randomized controlled clinical trial is warranted to test for efficacy.
Idiopathic macular telangiectasia type 2 (MacTel) is a bilateral degenerative condition of unknown etiology with characteristic neurosensory atrophy and perifoveal telangiectatic vessels that leak on fluorescein angiography. Other characteristic lesions include loss of retinal transparency, crystalline deposits, a decrease or absence of macular pigment, and hyperplasia of the retinal pigment epithelium (RPE) in the macular area. The spectral-domain optical coherence tomography (OCT) assessments show disruption of the photoreceptor inner segment–outer segment junction line (IS/OS line) or ellipsoid zone (EZ) and hypo-reflective cavities in both the inner and outer retina. The natural course is a gradual progressive bilateral loss of vision, occasionally accompanied by subretinal neovascularization, leading to severe vision loss. Genetic studies have suggested a MacTel gene locus on chromosome 1.
The natural course of gradual visual acuity loss in MacTel patients is approximately 1 letter per year (Clemons TE et al. IOVS, 2012; 53:ARVO e-abstract 982); however, affected individuals have profoundly reduced visual function compared to a normal age-matched reference group. This may be owing to the presence of bilateral lesions of photoreceptor disruption that begin temporal to the fovea, resulting in bilateral nasal scotomas and consequent prefixational blindness. A study correlating these visual field defects detected by microperimetry with OCT shows that the defects are closely associated with cavitation of the outer retina, indicating that loss of vision in MacTel is associated with structural changes at the level of photoreceptors. Current evidence suggests that photoreceptor cell loss is intrinsic to the disorder rather than being consequent to the vascular changes. Photoreceptor abnormality occurs early in the disorder and progression of photoreceptor cell loss may be detected on OCT with the loss of the IS/OS layer (ellipsoid zone). Measurement of the missing ellipsoid zone, captured as “en face” images, has been proposed as a potential outcome measurement for treatment studies. These OCT abnormalities have been associated with functional changes found on microperimetry, providing a structure-function index of severity in this disorder.
To date, there is no effective treatment for MacTel, although a variety of therapies, including steroids, photodynamic therapy, and laser photocoagulation, have been evaluated. Modulation of the leakage from the telangiectatic vessels with the use of anti–vascular endothelial growth factor (anti-VEGF) agents, including bevacizumab and ranibizumab, has also been shown to be ineffective in halting visual loss.
The class of molecules called “neurotrophic factors” has been demonstrated to slow the loss of photoreceptor cells during retinal degeneration. One of these factors, ciliary neurotrophic factor (CNTF), was found to be effective in slowing vision loss from photoreceptor cell death in animal models of outer retinal degeneration. Similarly, delivery of a neurotrophic factor to the outer retina in a mouse model that shares many phenotypic MacTel characteristics showed profound functional and anatomic photoreceptor cell rescue, with no effect on the associated vascular abnormalities. In addition, there is evidence that CNTF can cause regeneration of cone outer segments in rats expressing a mutant rhodopsin transgene. The delivery of CNTF to the retina is challenging, as the blood-retinal barrier prevents penetration of a variety of agents from the plasma. To surmount such a barrier, intraocular implant (NT-501), using encapsulated cell technology, was loaded with human RPE cells that were transfected with the CNTF gene. The CNTF was targeted for secretion by fusing the genomic murine Ig signal peptide in frame to the 5′ end of the hCNTF gene to produce CNTF. The NT-501 implant (Neurotech USA, Cumberland, Rhode Island, USA) was developed specifically using encapsulated cell technology with a semipermeable membrane, which allows CNTF to diffuse into the vitreous and nutrients to diffuse into the implant but prevents the host immune system from attacking the cells within the implant, allowing a supply of CNTF over an extended period of time. The technology also limits extraocular exposure of CNTF. The implant is surgically anchored into the eye and may be explanted if necessary. Encapsulated cell delivery of CNTF has been tested in 3 human phase 2 studies of treatment for retinal dystrophies and geographic atrophy associated with age-related macular disease. The use of this device appears to be safe and there was some limited suggestion of potential benefit in these studies. Since data from the mouse model with some MacTel phenotypes and data from various animal models of retinal degeneration suggested beneficial effect of CNTF in anatomic rescue of the photoreceptor cell, the use of neurotrophic molecules may provide a therapeutic benefit for patients with MacTel, which has no proven therapy. We now report the results from a phase 1 trial that evaluated the safety and tolerability of CNTF delivered over 36-month period by encapsulated cell devices (NT-501) for the treatment of eyes with MacTel.
Materials and Methods
Study Design
This nonrandomized, uncontrolled phase 1 clinical trial, registered with ClinicalTrials.gov (NCT01327911), was conducted according to the guidelines of the Declaration of Helsinki. The protocol was approved by the Institutional Review Boards (IRBs) of the 2 participating sites, the Western IRB and the University of California Los Angeles (UCLA) IRB. Each participant provided signed informed consent. A Data and Safety Monitoring Committee (DSMC) was established to monitor participant safety. This was an open-label, nonrandomized phase 1 study conducted at 2 retinal centers: the Retina Associates of Cleveland, Inc and the Jules Stein Eye Institute, University of California Los Angeles. The EMMES Corporation (Rockville, Maryland, USA) served as the coordinating center for the study.
Primary safety outcomes
The primary outcome was ocular safety after implantation of the CNTF capsule. Safety was measured by evaluating electroretinogram (ERG) responses and visual acuity assessments. Given the typical variability in ERG measurements, a persistent reduction of 30% in any of the ERG parameters was considered a potential safety concern. Additional safety factors were the presence of inflammation in anterior segment or posterior segment (vitreous and retina) on clinical examination at the slit lamp or on dilated ophthalmoscopy. Along with the persistent 30% reduction of ERG measurements, the following adverse outcomes were specifically designated in the study protocol for the implanted eye: visual acuity decrease of 15 or more Early Treatment Diabetic Retinopahty Study (ETDRS) chart letters compared with baseline, development of subretinal neovascularization, or peri-implant fibrosis that either blocks the visual axis of the implanted eye or affects the lens or retina. Other safety measures include the rejection or extrusion of the NT-501 device, the detection of serum CNTF levels, or the presence of circulating antibodies to CNTF and/or to NTC-201 cells. All adverse events were collected regardless of severity or potential relationship to the implant, CNTF, or surgical procedure.
Secondary efficacy outcomes
Secondary outcomes were best-corrected visual acuity (BCVA) and retinal sensitivity as measured by microperimetry. A secondary structural outcome of efficacy was the assessment of the photoreceptor IS/OS layer (or ellipsoid zone) loss as measured by topographic analysis of spectral-domain OCT volume scans and OCT thickness measurements. Two of the participants also had cone photoreceptor imaging using adaptive optics scanning laser ophthalmoscopy obtained at baseline and at the month 12, 24, and 36 follow-up visits.
Participants
Participants were eligible if they had bilateral MacTel, were aged 21 years or older, and were likely to be followed up for the duration of the study. The participants must not have had a history of prior intraocular surgery. The ocular inclusion criteria included BCVA of 20/50 or better and the presence of a disruption in the photoreceptor IS/OS layer (or ellipsoid zone) on OCT. The eye with worse BCVA was designated as the study eye. If both eyes had the same BCVA, then the eye with the less overall favorable clinical characteristics (as determined by the principal investigator [PI]) was designated as the study eye. If there was no difference between eyes, the right eye was designated as the study eye.
Encapsulated Cell Technology
The CNTF encapsulated cell implants (NT-501) were manufactured by Neurotech USA. The implant was inserted through a 2.0-mm sclerotomy made 3.75 mm posterior to the limbus in the inferotemporal quadrant. At the end of surgery, subconjunctival dexamethasone and antibiotics were administered and the eye was examined with an indirect ophthalmoscope to confirm the placement of the device into the vitreous.
Clinical Follow-up
A comprehensive eye examination was performed at baseline, including BCVA testing, dilated funduscopy, intraocular pressure (IOP), ocular imaging with stereoscopic color fundus (CF) photographs, fundus autofluorescence (FAF), fluorescein angiography (FA), spectral-domain OCT images, microperimetry, and ERG testing. Following implant surgery, participants were evaluated at week 1 and months 1, 3, 6, 12, 18, 24, 30, and 36.
Imaging
CF and FA images were recorded digitally using fundus cameras. FAF imaging was performed using Heidelberg HRA2 or Spectralis scanning laser ophthalmoscopes (Heidelberg Engineering GmbH, Heidelberg, Germany). OCT scans were acquired at UCLA using Heidelberg Spectralis OCT (Heidelberg Engineering GmbH) and in Cleveland using Cirrus HD-OCT (Carl Zeiss Meditec, Inc, Dublin, California, USA) devices. On the Spectralis, volume scans 15 × 10 degrees in area with 30-μm B-scan intervals were recorded. On the Zeiss Cirrus, a standard 512 × 128 cube scan covering a retinal area 20 × 20 degrees in size was acquired. Orthogonal topographic maps (“en face” images) of the IS/OS layer (or ellipsoid zone) were generated as described earlier. In 2 participants, adaptive optics scanning laser ophthalmoscopy (AOSLO) testing was conducted at the University of Rochester and UC Berkeley at baseline and at visits at months 12, 24, and 36. These results will be presented in another report.
Functional Testing
Monocular BCVAs were determined according to a standardized protocol, using ETDRS visual acuity charts starting at a distance of 4 meters. Scoring of the test was based on the number of letters read correctly. Possible scores ranged from 0 (Snellen equivalent <20/800) to 100 (Snellen equivalent 20/12).
Fundus-correlated automated mesopic microperimetry was performed following pupil dilation with 1.0% tropicamide and 2.5% phenylephrine hydrochloride and 5 minutes of visual dark adaptation, using Nidek MP1 microperimeters (Nidek Technologies, Albignasego, Italy). The technique has been described previously. Microperimetry was also performed at each visit on MAIA perimeters (CenterVue S.p.A., Padova, Italy), using a test grid and stimulus size identical to that used on the MP1. Results were reported in decibels (dB).
ERG testing was performed according to a standard protocol developed by the International Society for Clinical Electrophysiology of Vision (ISCEV). A full-field ERG test was performed at baseline and at months 3, 6, 9, 12, 18 24, 30, and 36, including a low-luminance white flash in a dark-adapted eye (DA 0.01) and the response to a “standard flash” (DA 3.0). An additional high-luminance flash (DA 10.0) was used in 1 clinic. The standard photopic single-flash (LA 3.0) and flicker ERG (LA 30 Hz) recordings were obtained in all patients at both institutions.
Measure of Serum CNTF, CNTF-Specific Antibodies, and Antibodies to NTC-201 Cells
Blood was drawn at baseline and at months 12, 24, and 36 for measurements of serum CNTF and antibodies to CNTF or NTC-201 cells. Serum CNTF was measured using a capture ELISA (R & D Systems). By incubation of the participant’s serum on a plate coated with hCNTF (R & D Systems), the CNTF-specific antibody signal was detected by a secondary antibody of horseradish peroxidase–conjugated donkey anti-human IgG (Jackson ImmunoResearch Laboratories, Inc, West Grove, Pennsylvania, USA). Titers for serum antibodies against the NTC-201 cells were determined by ELISA by incubating participant serum on a plate coated with NTC-201 cells for 16 hours and then probing with horseradish peroxidase–conjugated donkey anti-human IgG (Jackson ImmunoResearch Laboratories).
Image and Data Analysis
Study images were assessed and graded by a central reading center (The NIHR Biomedical Research Centre for Ophthalmology, at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology). ERG data were evaluated by G.H. and N.P.
Statistical Analyses
The analyses were performed using all available data. For changes in BCVA and the ellipsoid zone as measured by OCT, within-participant and between-study/fellow eye comparisons were based on paired Student t tests. McNemar χ 2 tests were used to examine the difference in the proportion of the increase or decrease in dB as measured by microperimetry between study and fellow eyes. All analyses were carried out using commercially available statistical software (SAS version 9.2; SAS Institute, Cary, North Carolina, USA). This safety study was not powered to evaluate efficacy.
Results
A total of 7 participants were enrolled and surgery was performed between August 26, 2011, and September 16, 2011. Two participants were male and 5 female, with ages ranging from 48 to 67 years. Five were white, 1 was Asian, and 1 identified as other race. All participants completed the 36-month follow-up.
Primary Safety Outcomes
No implant was rejected or extruded, and no severe ocular inflammation occurred. One participant had a BCVA decrease of 15 or more letters immediately after surgery and returned to preimplant level at month 3. Surgical complications included 1 participant who had decreased IOP following a wound leak, while another had an elevation of IOP to 36 mm Hg postoperatively. In both cases, IOP returned to the normal range by the 1-week visit and remained normal throughout the study. There were no protocol-defined adverse outcomes. However, 5 of the 7 participants developed miosis in the implanted eye and this persisted throughout the study. One of these 5 participants with miosis experienced difficulties with dark adaptation despite ERG findings that were not changed from baseline.
Measurement of serum CNTF, CNTF-specific antibodies, and antibodies to NTC-201 cells
No CNTF or antibodies to CNTF or NTC-201 cells were detected in the serum of participants at any time point (baseline, months 12, 24, and 36).
Electroretinogram
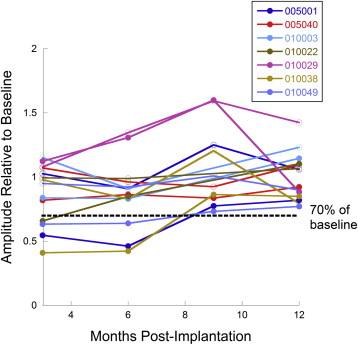
At months 3 and 6, a total of 4 participants demonstrated reduced amplitude in the ERG b-wave obtained from study eyes to a dark-adapted dim flash (DA 0.01) ( Figure 1 ). The responses of these study eyes to high-luminance flashes were preserved, as were photopic single-flash and 30-Hz flicker ERGs. Fellow eyes showed no change in ERG amplitude from baseline. At month 9, 1 of the 4 affected study eyes had returned to the normal range, and in 2 of the 4 eyes, the asymmetry between the study and fellow eyes had decreased. By month 12, none of the 4 treated eyes demonstrated a reduction in amplitude of the ERG b-wave to the dark-adapted dim flash stimulus condition. During the period of the reduction in the amplitude of the dark-adapted dim flash response, none of the 4 participants was symptomatic. However, another participant with no evidence of ERG changes complained of abnormal dark adaptation. As noted earlier, this patient had miosis.
Secondary Efficacy Outcomes
Best-corrected visual acuity
The mean ± standard deviation (SD) BCVA was 73.7 ± 8.0 letters for study eyes and 78.6 ± 8.4 letters for fellow eyes. The mean change ± standard error (SE) in BCVA from baseline to month 12 was 0.7 ± 1.9 ( P = .73) letters in the study eyes and 1.7 ± 0.8 ( P = .09) letters in the fellow eyes. The differences in mean change between study and fellow eyes did not meet statistical significance (mean ± SE difference = 1.0 ± 2.1; 95% confidence interval [CI]: −4.2 to 6.2; P = .66). The mean ± SE change in BCVA from baseline to month 26 was 1.14 ± 1.45 ( P = .46) letters in the study eyes and 3.1 ± 1.2 ( P = .04) letters in the fellow eyes. The differences between study and fellow eyes did not meet statistical significance (mean ± SE difference = 2.0 ± 1.7; 95% CI: −2.1 to 6.1; P = .28).
Optical coherence tomography
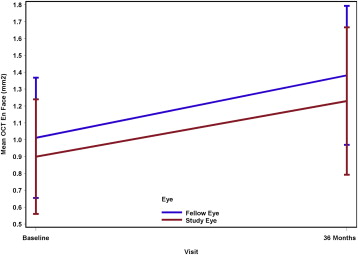
A secondary efficacy outcome was change in break area measured by OCT topographic maps of the IS/OS layer. The mean ± SD ellipsoid zone measurement at baseline was 0.90 ± 0.34 mm 2 in the study eyes and 1.01 ± 0.36 mm 2 in the fellow eyes. One participant was excluded from the analysis because no definite break in the IS/OS layer was detectable at baseline although a thinning of the ellipsoid band was present, but a break occurred at month 18. The mean ± SE change in break area at month 12 was 0.06 ± 0.04 mm 2 ( P = .15) in the study eyes and 0.12 ± 0.07 mm 2 ( P = .15) in the fellow eyes. The differences between study and fellow eyes did not meet statistical significance (mean ± SE difference = −0.06 ± 0.05; 95% CI: −0.19 to 0.07; P = .29). The mean ± SE change in break area at month 36 was 0.33 ± 0.15 mm 2 ( P = .08) in the study eyes and 0.37 ± 0.15 mm 2 ( P = .05) in the fellow eyes. Again, this difference did not meet statistical significance (mean difference = −0.04 ± 0.07; 95% CI: −0.22 to 0.16; P = .58). Figure 2 provides a graph of the means and standard errors by study and fellow eye at baseline and month 36.