Fig. 4.1
This is an image of the OcuLight SLx, the most commonly used ophthalmic diode laser in the United States (Image courtesy of Iridex, Mountain View, CA)

Fig. 4.2
This is a magnified image of the G-probe, with an excellent view of the curved footplate and the protruding tip (Image courtesy of Iridex, Mountain View, CA)
Most surgeons apply six to eight laser spots per quadrant for 360°, with the applications spaced one half probe tip width apart. This strategy produces confluent burns on the ciliary processes in human autopsy eyes [91]. It is highly recommended to avoid the 3 and 9 o’clock meridians so as to minimize trauma to the long posterior ciliary arteries and nerves [89]. It is also advisable to avoid perilimbal regions with excessive scleral or conjunctival pigmentation. Since the shorter wavelength of the diode laser is preferentially absorbed by pigment, laser uptake within pigmented anterior segment tissues can result in partial- or full-thickness ocular surface burns. Applying laser treatment to these highly pigmented regions also reduces energy transmission to the ciliary body, thus reducing efficacy [92].
The efficacy of transscleral diode CPC is directly related to the extent of ciliary body and ciliary process destruction. While the G-probe performs admirably at positioning the laser over the ciliary body in standard eyes, its performance in patients with atypical morphology or axial length (i.e., extreme myopia, congenital glaucoma, or microphthalmos) is deficient. For this reason, many surgeons routinely employ ocular transillumination to facilitate identification of the ciliary body for optimal laser probe placement. This procedure is performed by placing a bright focal light source against the posterior globe, while aiming the light anteriorly. When this is performed in a dark environment, the darker ciliary body will be highlighted against the backdrop of a brighter ruby-colored glow [93, 94].
Historically, the use of transscleral diode CPC in the United States has been relegated to eyes with severe, refractory glaucoma. Its status as a treatment of last resort is due to concerns regarding phthisis, chronic uveitis, pain, and loss of vision. The official recommendations of the American Academy of Ophthalmology Ophthalmic Assessment committee are based on Level III evidence and include [93]:
1.
Patients with refractory glaucoma who have failed trabeculectomy or tube shunt procedures
2.
Patients with elevated IOP and poor vision
3.
Patients with minimal or no visual potential who have eye pain thought to be secondary to the elevated IOP
4.
Patients whose ocular surface precludes incisional surgery (i.e., profoundly scarred conjunctiva, ocular cicatricial pemphigoid, thin sclera, history of scleritis)
5.
Patients who refuse incisional surgery
6.
Patients who are in emergent situations (i.e., neovascular glaucoma)
While this list serves as a useful guideline, the position of transscleral diode CPC in the treatment algorithm is surgeon specific. Ultimately, this decision is based on a careful consideration of the potential risks (i.e., visual loss, hypotony), the potential benefits (i.e., noninvasive procedure), and individualized patient characteristics (i.e., candidate for anesthesia).
Diode CPC has been shown to have both theoretical and practical benefits compared with older forms of cyclodestruction, but widespread adoption required strong clinical data establishing efficacy. The first item that required clarification was comparative efficacy with the other comparable cyclodestructive technique, Nd:YAG CPC. In a prospective, randomized study by Youn et al., they directly compared the IOP-lowering efficacy of Nd:YAG and diode transscleral CPC in patients with refractory glaucoma. At the 12-month follow-up, 83 % of the patients in the Nd:YAG group (mean 14.45 mmHg) and 71 % of the patients in the diode group (mean 15.22 mmHg) have an intraocular pressure between 5 and 20 mmHg. There was no significant difference between the two groups in the percentage of patients who achieved target IOP or in the final mean IOP. Similarly, there was no statistically significant difference in the postoperative visual acuity or change in visual acuity between groups at the final follow-up [95]. A retrospective study by Oguri et al. also compared the safety and efficacy of transscleral CPC using the Nd:YAG and diode lasers in patients with neovascular glaucoma. In this study, the probability of successful IOP control (≤23 mmHg) at 3 years was 47.2 % in the diode group, 13.3 % in the free-running mode Nd:YAG, and 8.8 % for the continuous wave Nd:YAG group. While there was no significant difference in efficacy between the diode laser and the free-running Nd:YAG laser, the diode laser was significantly more effective compared with the Nd:YAG in continuous wave mode. In the Oguri study, there was a significantly high rate of visual loss in all three groups (24 % for the diode group, 56 % for the free-running Nd:YAG, and 44 % for the continuous wave Nd:YAG) [96]. While the rates of visual loss were high, they are similar to other CPC studies that studied patients with neovascular glaucoma [63].
Establishing comparative efficacy was necessary to consider the diode laser as a viable alternative to the Nd:YAG laser for use in transscleral CPC. The next step in validating the diode laser involves documenting long-term IOP control. Kosoko and associates led the way in this endeavor when they designed a prospective, non-comparative study that specifically looked at the long-term efficacy of diode CPC in patients with refractory glaucoma, naïve to previous ciliary ablation. This study followed 27 eyes from 27 patients for 6–28 months, with a mean follow-up of 19 months. These patients were treated with 17–19 applications over 270°, for a total energy of 63.3 J. In this publication, failure was defined as an IOP drop of less than 20 % from baseline and an IOP above 22 mmHg. Based on this definition, the cumulative probability of success in this cohort of patients was 52 % at 2 years [97].
In 2006, Vernon et al. published their own efficacy results that spanned a longer duration of postoperative observation. In this retrospective study, the authors reviewed the results of 42 eyes from 39 patients who underwent diode laser transscleral CPC. These patients were followed for 36–84 months, with a mean duration of 65.7 months. The treatment consisted of 14 burns that were distributed around 270° of the limbus overlying the ciliary body. Each treatment session delivered 56 J of energy. In this study, the mean IOP decreased from a pretreatment level of 31.4 ± 8.8 mmHg to a final value of 15.6 ± 6.3 mmHg. This represents a 50.3 % decrease in the IOP compared with baseline. Treatment failure was defined as an IOP ≥ 22mmHg and a <30% reduction in IOP compared to baseline levels. Considering this criteria, 37 of the 42 eyes (88.1 %) achieved an IOP <22 mmHg, 35 of the 42 eyes (83.3 %) achieved an IOP reduction ≥30 %, and 31 out of the 42 (73.8 %) patients had a ≥30 % reduction in IOP and a final IOP <22 mmHg. The mean number of glaucoma drops decreased from 2.55 ± 0.83 to 1.71 ± 1.44, which was found to be statistically significant. This study also reinforced the finding that it often takes multiple treatments to achieve optimal success since 59.6 % of eyes required more than one treatment (mean 2.17 sessions) to achieve the desired outcome [98].
While the previous studies focused on efficacy in adults, a study by Autrata and associates considers the long-term IOP-lowering ability of diode CPC in the pediatric glaucoma population. This retrospective study reviewed 69 eyes in 53 children, with a mean age of 6.14 ± 1.29 (range 0.9–15) years. A majority of these patients have already undergone some form of eye surgery, with the average patient having undergone 1.6 previous surgeries. The mean follow-up for these patients was 5.6 ± 2.8 (range 2.2–9.5) years. In this particular study, success was defined as a postoperative IOP of ≤21 mmHg, with or without glaucoma medications. In patients who underwent a single treatment session, only 46 % of these patients had an IOP ≤21 mmHg at 12 months. With repeat laser procedures, the success rate increased to 79 % at 1 year, 63 % at 2 years, and 48 % at 5 years. The mean final post laser IOP was 20.81 ± 6.38 mmHg after a mean of 2.13 ± 1.47 laser treatment sessions [99]. Pediatric glaucoma patients seem to respond with the same degree of IOP lowering that you would see in an adult glaucoma patient, but the effect has a shorter duration of action. This limitation must be considered in light of its more favorable side effect profile. In pediatric glaucoma patients, diode CPC seems to be particularly useful for patients who are not good candidates for incisional surgery, as a temporizing measure before performing more invasive procedures and as an adjunct to previous tube shunt surgery [100, 101].
The results with diode laser CPC have been good enough that some have considered using it in lieu of a glaucoma drainage device in patients with refractory and neovascular glaucoma. In a study by Malik and associates, they retrospectively compared the use of a double plate Molteno tube shunt to diode CPC in glaucoma patients who failed previous surgery. Twenty-eight eyes in the diode group and 26 eyes in the glaucoma drainage implant group were followed for a mean of 150 (range 21–322) weeks. While the number of patients who achieved an intraocular pressure between 5 and 21 mmHg without adjunctive glaucoma medications strongly favored the Molteno tube shunt group (46 % in the Molteno group to 11 % in the diode laser group), the success rate was comparable in the patients who required postoperative glaucoma medications (81 % in the tube eyes and 64 % in the diode laser eyes) [102]. Yildirim and associates prospectively treated neovascular glaucoma patients with either diode CPC or an Ahmed Glaucoma Valve to compare the long-term safety and efficacy. Of the fifty-eight patients who completed the study, all had at least 2 years of follow-up. The Kaplan-Meier survival analysis demonstrated a 2-year probability of success of 61.18 and 59.26 % for the diode and Ahmed groups, respectively. The two groups also shared a similar rate of postoperative vision loss, with 24 % of the patients in the diode group experiencing a decrease in vision compared with a 27 % rate of vision loss in the Ahmed group [103].
Like all surgical procedures, diode transscleral CPC has its share of potential complications. The most common postoperative issues include visual loss, chronic uveitis, pain, hypotony, and treatment failure [87]. The prevalence of visual loss after diode transscleral CPC has been documented to be 7–31 %, which is lower than that seen in patients following Nd:YAG CPC (30–47 %) and cyclocryotherapy (5–69 %) [49, 57, 86, 87, 89, 97, 104–107]. Similarly, posttreatment discomfort is less pronounced following diode CPC as compared to Nd:YAG CPC and cyclocryotherapy [87, 108]. Other reported complications include phthisis bulbi, malignant glaucoma, anterior segment ischemia, sympathetic ophthalmia, lens subluxation, choroidal effusions, necrotizing scleritis, staphylomas, epiretinal membrane formation, intraocular pressure spikes, and corneal edema [87, 109–115].
Future Considerations
New Indications
Historically, cyclodestructive procedures have been reserved for patients with poor vision and refractory glaucoma. This is due to concerns about the high rates of visual loss and phthisis in the cyclocryotherapy literature [116]. A more detailed review of the literature highlights the fact that a majority of the early studies on cyclodestructive procedures targeted patients with refractory glaucomatous conditions, particularly neovascular glaucoma. In fact, a study by Sidoti and associates that evaluated the success rate of Baerveldt tube shunt placement in patients with neovascular glaucoma documented a high complication rate, including a 31 % incidence of complete visual loss (no light perception) and an 11 % incidence of phthisis [117]. This finding highlights the fact that refractory glaucoma conditions are difficult to treat and susceptible to poor outcomes, regardless of the intervention.
The evolution of cilioablative therapy has ushered in the much more refined diode laser procedure. When directly compared against cyclocryotherapy, diode laser cyclophotocoagulation was found to be equally effective at IOP reduction, with a significantly lower rate of profound vision loss (cyclocryotherapy 15.7 %, diode CPC 6.3 %) and phthisis (cyclocryotherapy 5.2 %, diode CPC 3.1 %) [118]. Moreover, as previously discussed, the study by Yildirim and associates documented the equivalent IOP-lowering efficacy of diode CPC and the Ahmed Glaucoma Valve in treating patients with neovascular glaucoma. Similarly, the rate of vision loss was statistically equivalent between the two groups (27 % in the Ahmed valve-treated patients and 24 % in the diode CPC patients). One particularly interesting finding was that this study reported a greater incidence of phthisis bulbi for the Ahmed Glaucoma Valve (6 %) patients as compared to those patients who received diode CPC (0 %) treatment [103].
The excellent results described above have encouraged surgeons to employ diode CPC in early stages of glaucoma and in patients with better vision [119, 120]. In 2001, Egbert and colleagues performed a prospective study of diode laser CPC as the primary surgical treatment in patients with primary open-angle glaucoma. In this study, one eye was treated with diode laser CPC while the fellow eye was treated with glaucoma drops. The IOP decreased in 67 % of the patients, with 48 % achieving a >20 % reduction in IOP compared with baseline eye pressure. There were no reports of phthisis bulbi, hypotony, or sympathetic ophthalmia in patients who were treated with laser. Regarding vision, 76 % (60/79) of the patients had the same or improved visual acuity as compared to baseline. Moreover, the incidence of visual loss was 23 % in both the diode CPC-treated eyes (18/79) and in the medically treated eyes (10/47) [121].
Another study looked at diode CPC as the primary surgical therapy in patients with primary open-angle glaucoma, chronic angle-closure glaucoma, and neovascular glaucoma. The patients in all three groups experienced significant drops in the IOP compared with baseline levels. Specifically, the patients with neovascular glaucoma experienced a 47 % decrease in IOP, the primary open-angle glaucoma patients achieved a 39 % drop in IOP, and the patients with chronic angle-closure glaucoma were found to have a 29.9 % reduction in eye pressure. There were no patients in any subgroup that experienced phthisis bulbi, prolonged hypotony, or vitreous hemorrhage. Importantly, the mean pre-laser visual acuity did not deteriorate following treatment in the primary open-angle glaucoma or chronic angle-closure glaucoma subgroups with good baseline vision [122].
With mounting evidence supporting the safety and efficacy of diode CPC as a primary treatment, an increasing number of surgeons are considering this procedure earlier in the course of the disease and in patients with better vision. In fact, the United Kingdom National Cyclodiode Laser survey reported that only 12.3 % of the respondents reserved diode CPC for patients with poor (≤6/60) vision [123]. It is likely that increasing familiarity and comfort with diode CPC will lead more surgeons to consider this intervention earlier in the course of the glaucoma treatment paradigm.
Endoscopic Cyclophotocoagulation
While it is difficult to classify endoscopic cyclophotocoagulation (ECP) as a new technology since it was first described in 1985 and then released as a commercially available unit in the early 1990s, it is reasonable to state that its greater acceptance and position in the therapeutic paradigm are still in evolution [15, 124]. ECP is a cilioablative technique that allows direct photocoagulation of the ciliary processes with endoscopic assistance. The E2 Microprobe Laser and Endoscopy Systems (Endo Optiks, Little Silver, NJ) incorporates a diode laser that emits pulsed continuous wave energy at 810 nm with a 175-W xenon light source, a helium-neon laser aiming beam, and a recordable video camera. The image guide, the light guide, and the laser guide are transmitted via fiber-optic technology to an 18- or 20-gauge probe. The 20-gauge endoscope provides a 70° field of view with a depth of focus from 0.5 to 15 mm. The 18-gauge endoscope affords a larger (110°) field of view with a depth of focus from 1 to 30 mm. While the 20G probe has a smaller diameter and can focus close to the target, the larger probe provides improved resolution and a more panoramic view [125].
Endoscopic cyclophotocoagulation can be performed through limbal, clear cornea, and pars plana approaches. A pars plana entry is favored by vitreoretinal surgeons, who often use this technology in combination with a pars plana vitrectomy. The clear corneal and limbal approaches are preferred by anterior segment surgeons, who can perform this procedure without the need for a vitrectomy.
In a clear cornea/limbal approach, viscoelastic is used to stabilize the anterior chamber and then expand the posterior chamber. This technique facilitates endoprobe access to the ciliary processes. Yu and associates reported that 2 mm was the ideal distance between the probe and target tissue to preserve the intended laser energy settings [126]. The initial power is 0.25–0.3 W, which is titratable up to 1.2 W. The laser should be set on continuous mode so that the surgeon is “painting” the laser across the target tissue (Video 4.2). Successful treatment is manifested as a whitening and contraction of the ciliary processes. Utilization of a curved probe allows treatment for up to 270° from a single incision. Kahook and colleagues found that a two-site treatment allowed for 360° of treatment, which resulted in significantly lower intraocular pressure and less dependence on glaucoma medication compared with a one-site approach [127]. At the end of the case, complete removal of viscoelastic is highly recommended since retained viscoelastic is one of the most common causes of post-ECP IOP elevation [128].
Given that ECP is still in its relative infancy, the specific indications are still evolving. Currently, the most common use of ECP is in combination with phacoemulsification for the treatment of early to moderate glaucoma. Other documented indications for ECP include the following: (1) the treatment of plateau iris syndrome, (2) for patients with refractory glaucoma, (3) to augment the effects of a glaucoma drainage implant, and (4) in patients who are not good candidates for filtration surgery or glaucoma drainage implants.
At the 2006 American Glaucoma Society annual meeting, Berke and associates presented the long-term data for the use of combined cataract surgery with ECP (Phaco/ECP) in the setting of medically controlled glaucoma. With a mean follow-up of 3.2 years (range 5 months–5.5 years), the mean IOP decreased 3.4 mmHg in the Phaco/ECP group as compared to a 0.7 mmHg increase in IOP following the straight cataract extraction. The Phaco/ECP group also experienced a >50 % reduction in medication burden, while there was no significant change in medication load for the patients who underwent cataract surgery alone [129].
Chen and associates evaluated the IOP-lowering efficacy of ECP in a large series of patients with refractory glaucoma of various diagnoses. The eyes in this study received 180–360° of laser treatment to the ciliary processes. The mean baseline IOP was 27.7 mmHg preoperatively, which decreased to 17.0 mmHg at the last follow-up. With the definition of success being an IOP ≤21 mmHg, 94 % of the treatments were successful at year one and 82 % were considered a success after 2 years. There was a mean reduction of one glaucoma medication over the course of the study. No significant complications were noted in this report and <10 % of the patients experienced a ≥ 2 line decrease in Snellen visual acuity [130].
Another compelling question is how ECP compares with traditional glaucoma surgeries (trabeculectomy and glaucoma drainage device) in the treatment of elevated IOP. Gayton and colleagues conducted a randomized prospective study that compared Phaco/ECP with combined phacoemulsification and trabeculectomy. Success was defined as a posttreatment IOP <19 mmHg with no deterioration of the visual field and no increase in optic nerve head cupping. Based upon this criterion, 30 % of the Phaco/ECP eyes achieved the target IOP range without medications and 65 % were successful with adjunctive medications. In the phacoemulsification/trabeculectomy group, 40 % of the patients achieved IOP control without medications, while 52 % of these patients reached the desired IOP range with additional glaucoma medications [131]. Lima et al. prospectively compared patients with refractory glaucoma who were randomized to receive either ECP or an Ahmed drainage implant. All of the patients were pseudophakic, status post at least one previous trabeculectomy with adjunctive antimetabolite, possessed vision better than light perception, and had an IOP ≥35 mmHg (mean 41 mmHg in both groups) on maximal tolerated medical therapy. At 24 months of follow-up, the mean postoperative IOP was 14.73 mmHg in the Ahmed group and 14.07 mmHg among ECP-treated patients. Based on a Kaplan-Meier analysis, this represents a 2-year success rate of 70.6 % for the Ahmed patients and 73.5 % for the ECP patients. Noteworthy, the Ahmed glaucoma implant-treated patients had a significantly higher rate of complications compared with those patients treated with ECP [132].
Neely and Plager published two studies detailing their experience with ECP in the pediatric population. In the first study, they retrospectively evaluated 6 years of data from 36 eyes of 29 patients with refractory glaucoma who underwent ECP. The mean baseline IOP was 35.06 mmHg and the mean IOP at the final visit was 23.63 mmHg, representing a 30 % decrease in IOP. The cumulative success rate for ECP in pediatric glaucoma patients was 43 %, with 25 % of all patients requiring more than one treatment to achieve the desired efficacy. Aphakic patients had a higher rate of complications, which included 2 retinal detachments, 1 episode of chronic hypotony, and 1 case of profound visual loss [133]. In another related study, Carter et al. performed a retrospective review of 34 eyes from 24 children and young adolescents who were followed for a mean of 44 months after being treated with ECP. The mean IOP decreased from 32.6 to 22.9 mmHg during the follow-up period. In this study, treatment failure was defined as a (1) postoperative IOP >24 mmHg and <15 % IOP lowering, despite the addition of adjunctive medications, or (2) the occurrence of a visually significant complication. Based on these qualifiers, the overall success rate was found to be 53 % [134].
One distinct advantage of ECP is that the treatment is performed with direct visualization of the target tissue. This is particularly useful in situations where the patient has abnormal anatomy (i.e., congenital glaucoma) or media opacities (i.e., corneal opacities). As it relates to the former, Barkana and associates reported successfully treating a congenital glaucoma patient with ECP in the setting of a failed transscleral diode CPC. Endoscopic visualization revealed several misplaced laser burns, representing the ill-fated attempt at transscleral CPC [135]. A study by Al-Haddad and colleagues documented a low incidence of successful IOP reduction (17 %) using ECP in patients with corneal opacities but acknowledged that the procedure still played a limited role in this challenging patient population. They also reported significant benefit of endoscopy alone in the intraocular placement of tube shunts when media opacities precluded good visualization. This study was limited by a low sample size, patients with abnormal anatomy and aqueous dynamics, and difficulty measuring the IOP accurately due to the opacified corneas [136].
While ECP has a favorable side effect profile compared to transscleral CPC, several complications have been reported. The largest series of Phaco/ECP patients reported the following complications: IOP elevation (14 %), fibrinous uveitis (7 %), cystoid macular edema (4 %), and transient hypotony (2 %) [137]. Another large case series that included patients with more advanced glaucoma reported fibrinous exudates (24 %), hyphema (12 %), cystoid macular edema (10 %), ≥2 line visual loss (6 %), and choroidal detachment (4 %) [130]. There are several theoretical, albeit currently unsubstantiated, risks such as endophthalmitis and suprachoroidal hemorrhage that are an inherent to any intraocular procedure. There was one reported case of post-ECP phthisis bulbi that occurred 5 months after treatment [138].
Micropulse Transscleral Diode Laser Cyclophotocoagulation
A new form of transscleral diode laser CPC has been developed that utilizes micropulse technology to denature the target tissue while minimizing collateral tissue damage. The diode laser emits a series of short (microsecond), repetitive bursts of energy. This active phase of the treatment algorithm is referred to as “on” time and confines the thermal effect to the absorbing tissue, with minimal diffusion of heat to the adjacent structures. The cooling period (“off” time) is proportionately longer than the pulse time, thus allowing the thermal relaxation of tissue and a return to baseline temperature [139, 140] (Fig. 4.3).
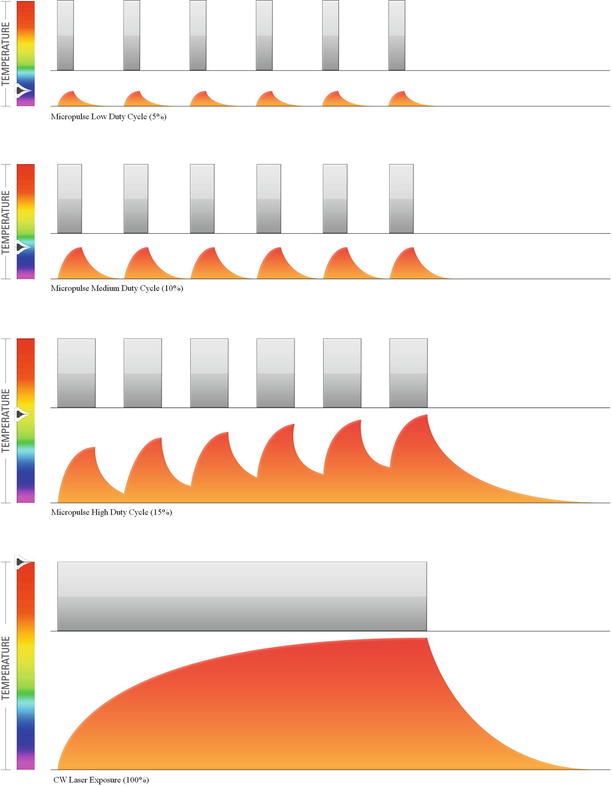
Fig. 4.3
This is an artistic rendering of micropulse laser delivery. These images demonstrate how continuous wave energy is separated into a series of repetitive microsecond pulses. The pictures provides a graphical representation of the fact that the duration of the laser pulse (“ON”) time can be adjusted to deliver adequate energy to the target tissue while minimizing thermal spread (Image courtesy of Iridex, Mountain View, CA)
Micropulse diode laser technology has been successfully used for the treatment of several retinal diseases, including diabetic retinopathy and maculopathy. This same technology is now being evaluated for safety and efficacy as a method for CPC. Based on its mechanism of action, the expectation is that micropulse diode laser CPC will achieve IOP-lowering efficacy that rivals traditional diode CPC, without the associated pain and inflammation.
In 2002, the results of a pilot study were published that documented a mean baseline IOP of 44 mmHg that decreased to 28 mmHg at week 1 and 36 mmHg at week 3. At the end of the first week, 75 % of the patients achieved ≥20 % decrease in IOP, while 63 % of the patients experienced a ≥30 % drop in IOP compared to baseline. These results demonstrate a significant short-term reduction in IOP that tends to regress over time [141]. In 2010, Tan and associates published the results from a prospective interventional case series that evaluated 40 eyes from 38 consecutive patients with refractory glaucoma who were treated with micropulse diode CPC using a redesigned G-probe. The mean baseline IOP was 40.1 mmHg and the patients were followed for an average of 17.3 (range 12–118) months. The mean IOP dropped to 24.6 mmHg at the final follow-up, with 35 % (14/40) requiring a second laser treatment. The mean number of glaucoma medications was reduced from 2.1 before treatment to 1.3 at the final visit. Importantly, only 31.6 % reported any pain during the procedure and none of the patients described the discomfort as moderate or severe. Regarding complications, all of the patients experienced mild inflammation and hyperemia. Fortunately, there were no reports of hypotony and no patients experienced a loss in visual acuity [142].
Indeed, the micropulse diode transscleral CPC appears to be a promising new technology that provides stellar IOP control with a favorable side effect profile. Further testing with longer follow-up is required to have a better sense of where this fits in our treatment algorithm.
Ultrasound-Mediated Cyclomodification
While effective, traditional cyclodestructive procedures are nonspecific interventions that coagulate the surrounding tissue along with the ciliary body and ciliary processes. This indiscriminate tissue damage results in the feared complications, including hypotony, phthisis, and pain.
These issues have prompted research into other tissue-specific and less destructive alternatives. This effort culminated in the introduction of high-intensity focused ultrasound (HIFU) for the treatment of glaucoma. In 1991, Silverman and colleagues published the results from a multicenter clinical trial, where 880 eyes of patients with refractory glaucoma were treated with HIFU. In this study, successful treatment was defined as an IOP between 6 and 22 mmHg. Given this qualifier, the authors reported a 6-month success rate of 48.7 % with one treatment and 79.3 % when re-treatment was allowed. The common complications in this study included mild iritis, scleral thinning, and phthisis (1.1 %) [143]. Unfortunately, the commercial unit was obtrusive and the process was cumbersome, thus leading to the demise of this device (Fig. 4.4) [144].
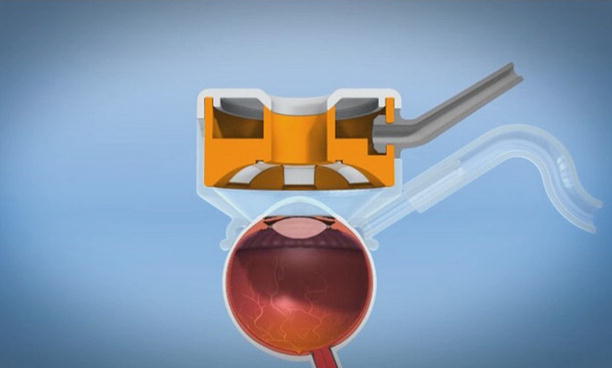
Fig. 4.4
This is a representation of the HIFU handpiece as it sits on the human eye (Image courtesy of EyeTechCare, Rillieux-la-Pape, France)
Improved technology (particularly miniaturized annual transducers) has facilitated the redesign of the HIFU unit into a compact, user-friendly device. The first commercially available HIFU unit is called EyeOP1 (EyeTechCare, Rillieux-la-Pape, France) and consists of a command module and a disposable circular therapy probe. The command module is a computerized system with a touch screen that allows input and adjustment of the setting parameters. The computer controls the two essential components of the system: (1) the generator that delivers the necessary power to the piezoelectric transducers and (2) the pressure reduction system, which modulates the amount of suction applied by the probe. The therapeutic device also consists of two vital parts: (1) the positioning cone, which centers the device on the eye and fixates it in proper position, and (2) the treatment probe, which actually creates the ultrasonic beam [144].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


