The management and selection of an appropriate surgical procedure for a patient with chronic otitis media requires that the clinician identify the proper subclassification of the disease process, to have prioritized the objectives of surgery, and, finally, to be aware of the histopathological limitations imposed on reconstruction by the disease process. Failure of surgery for chronic otitis media, because of either residual or recurrent disease, can be ascribed to improper selection of a surgical procedure as much as to failure of the surgical technique itself. Likewise, much of the current controversy concerning the surgical method of choice and the differences in results is due to comparison of disparate types of chronic otitis media. Assignment of a particular patient in the subclassification presented in
Table 17.1 will help guide the otologic surgeon in the selection of surgical procedure and the timing of surgery (
1).
Chronic active otitis media implies an active and hence potentially progressive process. Chronic active otitis media includes cases with cholesteatoma, with or without otorrhea, and cases without cholesteatoma but with chronic otorrhea. Except for medically unstable patients, the diagnosis of cholesteatoma almost always implies the need for surgical treatment. On the other hand, the diagnosis of chronic active otitis media without cholesteatoma should engender a trial of medical management in an attempt to arrest the otorrhea and convert the process to chronic inactive otitis media. Medical management includes culture of the suppuration, parenteral and topical antibiotics as indicated by culture and sensitivity tests, and frequent cleaning of the ear canal and removal of exuberant granulation if present. Failure of medical management in chronic active otitis media without cholesteatoma constitutes an indication for surgical treatment.
The presence of a complication of chronic otitis media, such as labyrinthine fistula or facial nerve paralysis, generally implies the need for urgent surgical management, with or without the presence of cholesteatoma (
Chapter 18).
Chronic inactive otitis media implies stable, nonprogressive pathology of the tympanic membrane, middle ear, and mastoid cavity caused by previous suppuration and/or eustachian tube dysfunction. In most cases, chronic inactive otitis media represents a relative indication for elective surgery generally directed toward reconstructive procedures for the tympanic membrane and ossicular chain.
Chronic inactive otitis media with frequent reactivation refers to an ear without cholesteatoma, but with a perforated tympanic membrane and a history of episodic mucopurulent drainage. In this condition, although the drainage may cease with oral and/or topical antibiotics, it recurs without an obvious inciting event such as exposure to water. The significance of this diagnosis is that attempts to repair the perforated tympanic membrane without exploration of the mastoid, antrum, and epitympanum to eliminate active infection, granulation, or obstruction of the aditus ad antrum (“attic block”) will often result in graft failure and recurrent suppuration. Therefore, before recommending simple tympanoplasty or ossiculoplasty as an elective procedure in a case of chronic otitis media that has only recently been rendered inactive by medical management, a waiting period is advisable to minimize the risk of spontaneous reactivation.
CLASSIFICATION OF RECURRENT CHRONIC OTITIS MEDIA FOLLOWING TYMPANOMASTOIDECTOMY
The classification outlined in
Table 17.1 can be used either for primary disease or for recurrent disease following mastoid tympanoplasty. Thus recurrent cholesteatoma with or without otorrhea or recurrent chronic otorrhea can easily be subclassified as chronic active otitis media (recurrent). Occasionally, both with canal wall-up and with canal wall-down procedures, intermittent suppuration may occur and therefore fall under the category of chronic inactive otitis media with frequent reactivation (postoperative). Following canal wall-down procedures, this may take the form of an unstable epithelium. On an intermittent basis, granulation tissue may appear commonly in the sinodural angle or tegmental area but responds to local hygiene and topical antibiotics. On the other hand, a canal wall-down “mastoid bowl” with continuous otorrhea but without cholesteatoma,
in which the otorrhea does not respond to local hygiene and topical antibiotics, should be classified as chronic active otitis media (recurrent) and usually implies residual or recurrent disease in remaining pneumatized spaces of the temporal bone.
ROLE OF RADIOGRAPHIC STUDIES IN THE SUBCLASSIFICATION OF CHRONIC OTITIS
The classification presented in
Table 17.1 is based on clinical observation, either immediate or over time, and generally does not require radiographic studies for classification. However, there are special cases in which computed tomography (CT) of the temporal bone will aid in the subclassification. For example, in a case with an attic retraction pocket, if the superior and posterior limits of the pocket are not visible, CT may indicate an epitympanic soft tissue mass consistent with an attic cholesteatoma, thus allowing subclassification of chronic active otitis media with cholesteatoma. Study of the temporal bone plays a much larger role in the selection of a surgical technique in the evaluation of complications of chronic otitis media and in the evaluation of patients with recurrent chronic active otitis media following mastoid tympanoplasty.
OBJECTIVES AND PRIORITIZATION IN SURGERY FOR CHRONIC OTITIS MEDIA
In addition to appropriate subclassification of the disease process, the selection of an appropriate surgical procedure also requires the surgeon to have adopted specific objectives and priorities in the treatment of chronic ear disease. With few exceptions, the major objectives, in order of priority, are (i) elimination of suppuration and other manifestations of chronic active otitis media, (ii) alteration of the anatomy of the ear and mastoid in an attempt to prevent recurrent disease and to optimize subsequent cleaning and otologic monitoring of the ear, and (iii) reconstruction of the tympanic membrane and ossicular system in order to achieve serviceable and stable postoperative hearing.
It is generally recognized that failure to achieve the first objective will become manifest by residual disease and require revision surgery. However, it should be pointed out that failure to achieve the second objective is also a common cause for revision surgery for recurrent disease. Therefore, paradoxically, a surgical attempt to restore the eardrum and canal to a normal anatomic condition in an inappropriately selected patient may predispose to recurrence of the disease process.
For example, in cases with attic cholesteatoma managed either by anterior atticotomy or by canal wall-up tympanomastoidectomy, substitution of the removed bony scutum by a fascial graft may result in recurrent attic retraction and cholesteatoma formation. However, the placement of free cartilage grafts in the epitympanum following such a procedure is effective in preventing such reretraction.
CLINICAL FACTORS INFLUENCING THE SELECTION OF SURGICAL APPROACH
Several factors, including the clinical history, otologic findings, and hearing, both in the diseased and contralateral ear, are important considerations in surgical decision making. For example, a limited attic cholesteatoma with no suppuration may be adequately treated by anterior atticotomy. Extensive disease, as indicated by the presence of complications, radiographic evidence of significant bone destruction, profuse purulent drainage, and otologic history consistent with progression over many years, usually is best handled by a postauricular mastoidectomy.
Table 17.2 presents relative indications for various surgical approaches. Surgery for chronic otitis media should be individualized depending upon the clinical circumstances. It should be emphasized, however, that these indications are relative ones and must be modified by the experience of the particular operating surgeon. Also playing significant roles in the choice of the surgical procedure are such factors as the reliability of the patient in conforming to the otologic follow-up necessitated by a given surgical procedure, age of the patient, presence of usable hearing in the operated on and contralateral ears, evidence for poor eustachian tube function such as the presence of bilateral chronic otitis media, uncontrolled allergic rhinosinusitis, and a history of cranial base anomalies. In general, the surgeon should strive to eliminate the disease process, as well as perform a reconstructive procedure in one surgical procedure unless there is strong indication that staging and multiple procedures will offer a significant benefit to the patient. Although the surgeon should have a specific, planned procedure in mind preoperatively, including the elements of the surgical procedure outlined in
Table 17.2, he or she should prepare the patient and allow time for intraoperative revision of the surgical plan.
RECURRENT CHRONIC ACTIVE OTITIS MEDIA: CAUSES, EVALUATION, AND MANAGEMENT
The estimated incidence of recurrent chronic active otitis media when no residual disease was left at the time of the first surgery ranges from 3% to 18% of all surgical procedures
for chronic otitis media (
2,
3,
4,
5). The causes of failure of mastoidectomy include residual or recurrent cholesteatoma and residual or recurrent suppuration of the middle ear and mastoid compartments.
Residual Disease
Residual cholesteatoma with or without suppuration or residual chronic infection without cholesteatoma may be attributed to inadequate exposure during the previous surgical procedure, failure to recognize the extent of primary disease, or failure to exenterate disease during the previous procedures. Common examples of this include cholesteatoma in the sinus tympani or oval window or round window niches, which are notoriously difficult to access; failure to exenterate obstructed and infected air cells, principally along the tegmen, sinodural angle, facial recess, and mastoid tip (
6); and failure to recognize significant disease in the hypotympanum and infralabyrinthine cells (
7).
Recurrent Disease
Mastoid tympanoplasty may also fail because of recurrence rather than residual disease. The causes of failure due to recurrent disease are somewhat different following canal wall-up versus canal wall-down tympanomastoidectomy. The most common cause of failure in canal wall-up procedures is failure to alter the anatomy of the ear and mastoid and to make recurrence less likely. Common examples of this include recurrent attic retraction and cholesteatoma due to failure to insert stiff grafts such as free cartilage to prevent reretraction, postoperative sequestration of the mastoid from the middle ear space due to attic block, and failure to maintain an adequate communication between the mastoid and middle ear via the facial recess. In contrast, in canal wall-down tympanomastoidectomy the most common causes of recurrent chronic suppuration are postoperative obstruction, sequestration, and reinfection of residual air cells of the tegmen, sinodural angle, facial recess, or mastoid tip; or inadequate meatoplasty or inadequate removal of the bone over the facial ridge, resulting in a mastoid bowl in which it is difficult or impossible to provide local hygiene. It is important to recognize that in this sense the objectives of canal wall-up surgery differ from that of canal wall-down procedures. Thus in a canal wall-up procedure the objective is clearly to remove all disease, both granulation tissue and cholesteatoma, but to allow remucosalization of the pneumatized space of the mastoid in the postoperative period. In contrast, remucosalization of the mastoid not only is not the objective in canal wall-down procedures but in fact commonly results in recurrent disease due to obstruction, sequestration, and reinfection. This principle is best illustrated by the example of the fenestration cavity. The fenestration procedure in which a canal wall-down mastoidectomy was performed for the purpose of hearing improvement in otosclerosis commonly resulted in a chronic draining mastoid bowl (
8). Thus in an ear in which there was originally no suppuration whatsoever, the development of a draining mastoid bowl must be attributed to the surgical procedure itself. It is important to remove most or all residual pneumatized cells principally in the sinodural angle tegmen and facial recess, particularly in the canal wall-down technique, because such residual cells may become easily obstructed and then reinfected.
EVALUATION OF RESIDUAL RECURRENT DISEASE FOLLOWING FAILURE OF PREVIOUS MASTOID SURGERY
The evaluation and management of cases in which there is either a residual or recurrent cholesteatoma or persistent or recurrent suppuration requires careful clinical and radiographic evaluation. In failed canal wall-up technique, CT of the temporal bone will help to reveal the extent of recurrent
cholesteatoma or the location of obstructed and infected residual air cells.
The clinical situation of recurrent suppuration without cholesteatoma following previous canal wall-down technique requires special consideration. Skin grafts placed over bone rather than a thick, subcutaneous soft tissue layer are relatively unstable and are prone to ulceration and suppuration, even in the absence of deep-seated recurrent disease. In such cases, local hygiene, debridement, and delayed split-thickness skin grafts (
Chapter 10) may result in a dry mastoid bowl. The bacteriology of chronic suppurative otitis media, particularly following canal wall-down procedures, includes a high prevalence of anaerobic pathogens (
9,
10,
11). In this regard it is important to recognize that commonly used topical otologic antibiotics have poor anaerobic coverage. Failure of delayed skin grafting and topical or parenteral antibiotics based on culture and sensitivity implies more deep-seated sequestrated disease and should engender a radiographic study. Despite the localization implied by the term
chronic otitis media, insufficient clinical attention has been paid to the role of the hypotympanum in chronic active otitis media (
6,
7).
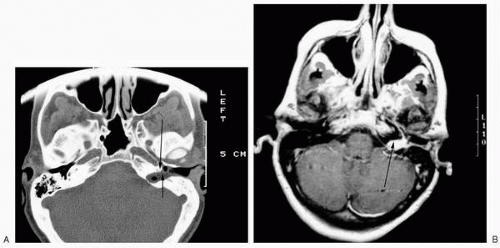
CT and magnetic resonance imaging (MRI) may demonstrate significant disease in the hypotympanum (
Fig. 17.1A, B). Imaging may also demonstrate that unsuspected residual or recurrent disease is no longer contiguous with the previous surgical site (
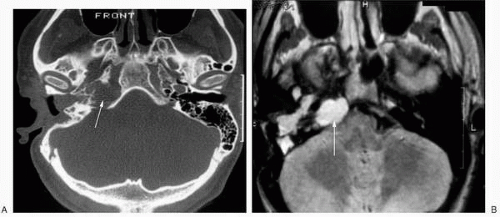
Fig. 17.2) or unsuspected contiguous disease in the petrous apex (
Fig. 17.3A,B) (
12).