Cholesteatoma
Ted A. Meyer
Chester L. Strunk Jr.
Paul R. Lambert
Cholesteatomas are expansile lesions of the temporal bone lined by stratified squamous epithelium that contain desquamated keratin. Some cholesteatomas are invaginated pouches that can develop from retraction pockets, while others are completely enclosed cysts. They most frequently involve the middle ear and mastoid, but they may develop anywhere within the pneumatized portions of the temporal bone. They may be congenital (infrequently) or acquired.
The accumulation of keratin may cause infection, otorrhea, bone destruction, hearing loss, facial nerve paralysis, a labyrinthine fistula, and intracranial complications such as epidural and subdural abscesses, parenchymal brain abscesses, meningitis, and thrombophlebitis of the dural venous sinuses.
Cholesteatoma is a misnomer originally coined by Johannes Mueller in 1838 when he described “layered pearly tumor of fat, which was distinguished from other fat tumors by the biliary fat or cholesterin that is interspersed among the sheets of polyhedral cells” (1). Cholesteatomas do not contain fat, and they do not usually contain cholesterin. Nevertheless, the term remains, despite a more appropriate term suggested by Schuknecht: keratoma.
The matrix of a cholesteatoma is composed of fully differentiated squamous epithelium resting on connective tissue. The deeper layers of the epithelium of a cholesteatoma matrix show activity in the form of downgrowths into the underlying connective tissue. Cholesteatomas have a layer of granulation tissue in contact with bone. This layer of granulation tissue elaborates various enzymes such as collagenase resulting in bone destruction.
Cholesteatomas are recidivistic by nature. The conditions or processes through which they develop are often present throughout a patient’s life. Eustachian tube disease, with negative middle ear pressures, and a retracted eardrum are usually seen in patients with primary acquired cholesteatomas, and this can continue even with the complete surgical removal of a cholesteatoma. The function of the eustachian tube does not necessarily ever improve, and the patient is at risk for further cholesteatoma. If cholesteatoma is left behind surgically, either planned or unknowingly, this is considered residual disease. After being completely removed, if cholesteatoma forms again, this is considered a recurrence.
CONGENITAL CHOLESTEATOMA
Congenital cholesteatoma is defined by Derlacki and Clemis (2) as an embryonic rest of epithelial tissue in the ear without tympanic membrane perforation and without a history of ear infection. Levenson et al. (3, 4) have modified the definition of a congenital cholesteatoma to include a normal pars flaccida and pars tensa, no history of prior otorrhea, and no history of prior otologic procedures. Prior episodes of otitis media without otorrhea are not criteria for excluding congenital origin. Two-thirds of the middle ear congenital cholesteatomas are seen as a white mass in the anterior-superior quadrant (Fig. 151.1).
They may also be found within the tympanic membrane and in the petrous apex. The mean age at presentation for a congenital middle ear cholesteatoma is 4.5 years, with a male-to-female preponderance of 3:1 (4). The pathogenesis of congenital cholesteatomas is incompletely understood. In a review of the development of the epibranchial organs, Teed (5) noted an ectodermal epithelial thickening that developed in proximity of the geniculate ganglion, medial to the neck of the malleus. This mass of epithelial cells soon undergoes involution to become mature middle ear lining. Teed believed that if involution failed to take place, this formation could be the source of a congenital cholesteatoma. In pursuit of this theory, Michaels (6, 7) undertook a review of fetal human temporal bones and identified a squamous cell tuft present from 10 to 33 weeks of gestation in 37 of 68 specimens studied. He termed this structure the epidermoid formation
and noted it to be located in the anterosuperior wall of the developing middle ear cleft. Failure of the epidermoid formation to involute could be the basis for the development of cholesteatomas in the anterior mesotympanum (8, 9, 10). Other investigators implicate ectodermal migration or even metaplasia of the middle ear mucosa in the pathogenesis of congenital cholesteatomas (11, 12).
and noted it to be located in the anterosuperior wall of the developing middle ear cleft. Failure of the epidermoid formation to involute could be the basis for the development of cholesteatomas in the anterior mesotympanum (8, 9, 10). Other investigators implicate ectodermal migration or even metaplasia of the middle ear mucosa in the pathogenesis of congenital cholesteatomas (11, 12).
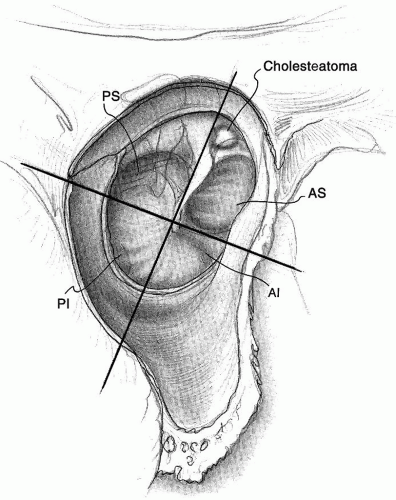 Figure 151.1 Congenital cholesteatoma of the anterior-superior quadrant. AI, anterior inferior; AS, anterior superior; PI, posterior inferior; PS, posterior superior. |
To further complicate the understanding of the development and pathogenesis of congenital cholesteatomas, they have been described as developing in or isolated to the mastoid (13, 14). Staging systems and management strategies have been developed by several groups (15, 16, 17), with staged surgical procedures recommended for the more complicated or higher-stage lesions.
ACQUIRED CHOLESTEATOMA
Acquired middle ear cholesteatomas come in two varieties: primary or retraction pocket cholesteatoma and secondary cholesteatoma. Cholesteatomas that arise from retraction pockets are known as primary acquired cholesteatomas on the basis that infection has not given rise to the cholesteatoma. Several theories have been advanced to explain the formation of primary acquired or attic retraction cholesteatomas, including invagination of the pars flaccida, basal cell hyperplasia, otitis media with effusion, and perforation of the pars flaccida membrane with epithelial ingrowth (Table 151.1). Patients with cleft palates are particularly prone to the development of primary acquired attic cholesteatomas (18, 19, 20, 21, 22).
TABLE 151.1 PATHOGENESIS OF CHOLESTEATOMAS | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
The invagination theory is supported by the observations of Aschoff in 1897 and Wittmaack in 1933 (23). They proposed that an infantile sterile otitis media neonatorum or nonbacterial otitis media develops soon after birth. Before it has had time to resorb, a permanent fibrosis and thickening of the embryonic subepithelial tympanic connective tissue occurs resulting in blockage of the attic causing a localized negative pressure with retraction of the pars flaccida. The fibrosis and thickening in the attic blocks the normal process of pneumatization of the epitympanum and antrum and decreases the pneumatization of the mastoid process and petrous portions of the temporal bone throughout the patient’s life. This small dimplelike retraction of the pars flaccida that cannot be reduced by inflation of the eustachian tube is the first stage in the development of an attic cholesteatoma.
A second method by which a small retraction pocket may develop is from long-standing otitis media with effusion (Fig. 151.2). Bluestone and Klein (18) demonstrated that in children with attic retractions, the eustachian tube constricts rather than dilates with swallowing. This results in impaired ventilation of the middle ear and mastoid air cell system and fluctuating or sustained high negative middle ear pressures. Negative middle ear pressure caused by eustachian tube dysfunction can result in retraction of the pars flaccida and collection of desquamated debris.
Like primary acquired cholesteatomas, several pathogenic mechanisms may contribute to the formation of secondary acquired cholesteatomas (Table 151.1). The implantation theory, the metaplasia theory, and the epithelial invasion theory have all been advanced as possible mechanisms involved in cholesteatoma formation. The implantation theory describes the formation of a cholesteatoma by the iatrogenic implantation of skin into the middle ear or eardrum as a result of surgery, a foreign body, trauma, or a blast injury. Cholesteatomas may develop secondary to a myringotomy for ventilating tube
placement or a tympanoplasty procedure. They occur as a result of epithelial migration or displacement through the myringotomy or from the displacement of a flap of the tympanic membrane into the middle ear at the time of a tympanoplasty. Secondary acquired cholesteatomas are also thought to arise from a perforation as a result of acute necrotic otitis media in childhood (24).
placement or a tympanoplasty procedure. They occur as a result of epithelial migration or displacement through the myringotomy or from the displacement of a flap of the tympanic membrane into the middle ear at the time of a tympanoplasty. Secondary acquired cholesteatomas are also thought to arise from a perforation as a result of acute necrotic otitis media in childhood (24).
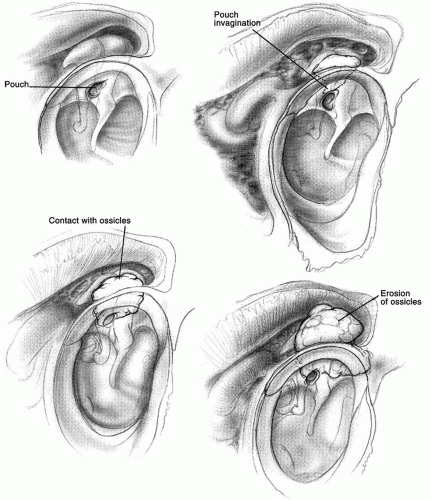 Figure 151.2 Evolution of an attic cholesteatoma. |
The metaplasia theory describes the transformation of columnar epithelium to keratinized stratified squamous epithelium secondary to chronic or recurrent otitis media. Support for this theory comes from changes that occur in the bronchi in the face of chronic irritation and infection. However, metaplasia is not thought to be a significant cause of cholesteatoma in humans (25). The epithelial invasion theory involves the invasion of the middle ear by skin from the meatal wall of the outer drum surface through a marginal perforation or an attic perforation (26). This is supported by experimental evidence demonstrating that epithelial cells migrate along a surface until they encounter another epithelial surface, at which point they stop migrating; this is known as contact inhibition. If the middle ear mucosa were destroyed by infection, then this would allow for epithelial migration from a marginal perforation. This is the generally accepted theory for the formation of secondary acquired cholesteatomas of the posterior-superior tympanic membrane.
Cholesteatoma may also arise in the external auditory canal (27, 28, 29, 30, 31) often after trauma from repeated direct manipulation. Like cholesteatoma in the middle ear, epithelial migration is disrupted in external auditory canal (EAC) cholesteatoma. Patients present with otorrhea, otalgia, bony destruction, and trapped squamous debris, and some have hearing loss. Some EAC cholesteatomas have similar characteristics as keratosis obturans, but in general, surgical removal is the treatment modality of choice for EAC cholesteatoma, where patients with keratosis obturans can usually be managed by frequent office cleanings and topical therapy (32).
A unique feature that cholesteatoma and tympanic membrane epithelium have in common is migration. No other epithelium tested, including skin, vocal cord, and oral epithelium, has shown the locomotion present with tympanic membrane epithelium and cholesteatoma (33). Once a retraction pocket develops, the epithelial migratory pattern is altered and keratin accumulates. This is the second stage in the development of a cholesteatoma. The sac slowly enlarges by accumulation of keratin and other debris until the walls of the attic are reached. Once this point is reached, bone resorption occurs. Three factors appear to be involved in the process of bony resorption: (a) mechanical, related to pressure generated by the expansion of cholesteatoma as it accumulates increasing amounts of keratin and purulent debris (34, 35, 36); (b) biochemical, due to bacterial elements (endotoxins), products of the host’s granulation tissue (collagenase, acid hydrolases), and substances related to the cholesteatoma itself (growth factors, cytokines) (37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49); and (c) cellular, predominantly induced by osteoclastic activity (50, 51, 52, 53). It is likely that bone destruction in cholesteatoma results from a combination of these factors, but clarification is needed regarding their specific roles.
Multinucleated osteoclasts within the subepithelial matrix of a cholesteatoma release acid phosphatase, collagenase, and other proteolytic enzymes that resorb the bone products. The osteoclasts may be further activated by infection, pressure, and Langerhans cells through an immune mechanism. Cholesteatoma debris is a favorite culture medium for bacteria from the external meatus, including staphylococci, Pseudomonas aeruginosa, Proteus, Enterobacter, aerobic and anaerobic nonhemolytic streptococci, diphtheroid bacilli, and Aspergillus molds. When the cholesteatoma becomes infected from water contamination, a foul-smelling discharge ensues. An active infected cholesteatoma will resorb bone at a faster rate.
The ability of cholesteatomas to erode bone is what makes them particularly dangerous (Fig. 151.3). Their expansion is dictated by space available, their migratory tendency, and their internal desquamation. Pressure alone may cause bone resorption to take place.
SURGICAL ANATOMY
Cholesteatomas are channeled along characteristic pathways by ligaments and folds. During the third to fifth fetal months, endothelial-lined sacs develop from evaginations of the first brachial pouch to form the tympanic cavity mucosal folds and ossicular suspensory ligaments. These sacs contact each other, defining the various pouches, spaces, and compartments that divide the middle ear (Fig. 151.4).
 Figure 151.3 Infected cholesteatoma of the attic eroding the scutum (arrow). |
The most common locations of origin of cholesteatomas in decreasing frequency are the posterior epitympanum, the posterior mesotympanum, and the anterior epitympanum (54). Epitympanum cholesteatomas originate in a shallow pocket that lies between the pars flaccida of the tympanic membrane and the neck of the malleus. This pouch, known as Prussak space, has as its floor the lateral process of the malleus and its associated mucosal folds lying in the horizontal plane. Cholesteatomas most commonly exit Prussak space by the posterior route: the cholesteatoma penetrates the superior incudal space lateral to the body of the incus. From there, it traverses the aditus ad antrum to enter the mastoid (Fig. 151.5). The cholesteatoma may reach the middle ear by descending through the floor of Prussak space into the posterior space of von Troeltsch, a pouch lying between the tympanic membrane and the posterior mallear fold, the inferior edge of which contains the chorda tympani nerve (Fig. 151.4). This pouch contains a medial, superior, and lateral wall but is open to the mesotympanum inferiorly toward the posterior mesotympanum. Cholesteatomas in this region may involve the stapes, round window, sinus tympani, and facial recess.
The second most common site of origin of cholesteatomas is the posterior mesotympanum (Fig. 151.6). The pars tensa retracts into the mesotympanum to form a cholesteatoma sac that passes medial to the malleus and the incus. Cholesteatomas in this region invade the sinus tympani
and facial recess. The sinus tympani lies between the facial nerve and the medial wall of the mesotympanum. The facial recess is bounded by the fossa incudis and the facial nerve posteriorly and the chorda tympani nerve anteriorly. Both areas are difficult to access surgically (Fig. 151.7) and are common sites of residual cholesteatoma.
and facial recess. The sinus tympani lies between the facial nerve and the medial wall of the mesotympanum. The facial recess is bounded by the fossa incudis and the facial nerve posteriorly and the chorda tympani nerve anteriorly. Both areas are difficult to access surgically (Fig. 151.7) and are common sites of residual cholesteatoma.
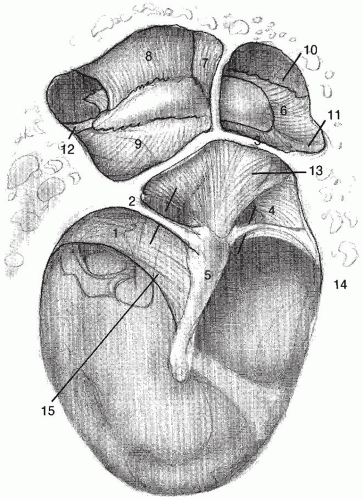 Figure 151.4 Spaces and pouches on the middle ear defined by various ligaments and folds. 1, posterior mallear fold; 2, posterior tympanic stria; 3, lateral mallear fold; 4, anterior tympanic membrane stria; 5, malleus (short process); 6, tensor fold; 7, superior mallear fold; 8, superior incudal fold; 9, lateral incudal fold; 10, anterior epitympanic space; 11, anterior mallear ligament; 12, postincudal ligament; 13
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|