Chin Augmentation
Jonathan M. Sykes
Christina K. Magill
The chin prominence is not present in any four-legged mammal (1). During evolution, with the adoption of an upright posture and with verticalization of the face, the chin became an important facial feature. The events contributing to the evolutionary development of the chin in humans are open to speculation; however, the importance of the chin in the overall appearance of the face cannot be overstated (2).
Facial beauty arises from symmetry and balanced proportion of all facial features. Although standards of facial beauty are often determined by social media and are time-adjusted, certain elegant features are not affected by time trends. A strong and well-projected chin is one of those features. For this reason, it is not surprising that no United States president has ever had a weak chin. A strong chin helps support the soft tissues of the lower face, and a well-projected chin improves the cervical skin and contributes to a well-defined cervicomental angle (3).
It is important to analyze the chin in three dimensions in order to determine if the deformity is horizontal, vertical, or related to transverse discrepancy or asymmetry (4). Surgical correction of aesthetic deformities of the chin can be performed either by chin augmentation with an implant or by osteotomy and advancement (or reduction) of the bony mentum (5). Simple horizontal deficiencies are often easily corrected with alloplasts. More complex problems of the mentum, such as transverse asymmetry or significant vertical dysmorphia, usually require bony osteotomy of the mentum (genioplasty) with repositioning of the chin into a more ideal three-dimensional position. This chapter outlines the pertinent anatomy and classification of chin deformities and describes an algorithm for correction of these problems.
PATIENT EVALUATION
Careful analysis of the face and chin is important in order to choose and execute the correct procedure. Specifically, the chin should be evaluated as it relates to other skeletal and soft tissue structures, including the lips, teeth, nose, and soft tissues of the neck. A detailed history of past trauma, orthodontic treatment, or prior oral surgery is essential. This is important because many patients with dental malocclusion and underlying facial skeletal abnormalities are treated with orthodontics. Orthodontic therapy may correct the malocclusion, but does not address the underlying facial skeletal deformity (Fig. 192.1). It is also important to identify any past dental extractions, as these can impact future surgical decisions. Lastly, it is important to identify and discuss any temporomandibular joint dysfunction (TMD). Although chin surgery does not directly affect the occlusion, any significant TMD can alter the decision to perform mentoplasty.
Physical examination of the chin should include inspection and palpation of the chin itself and of the adjacent structures such as the lips, teeth, and nose (6). The entire face should be observed at rest and during animation to evaluate the mentalis soft tissue mound and its support. In many patients with either horizontal or vertical microgenia, the mentalis muscle hypertrophies in an effort to create lip competence (7). Overworking of the mentalis muscle causes dimpling of the chin and is referred to as “mentalis strain” (Fig. 192.2). This condition is often associated with open bite deformities and/or microgenia.
Evaluation of patients being considered for chin surgery should include three-dimensional analysis of the chin: (a) vertical (superior-inferior), (b) horizontal (anterior-posterior), and (c) transverse. Analysis should consist of systematic inspection, clinical photographs, and possible radiographic examination (8).
The evaluation of all patients for possible chin surgery should include consistent and reproducible clinical photographs in three views: AP (frontal), lateral (profile), and oblique. These photographs allow analysis of the contour and projection of the chin as it relates to the lips, nose,
labiomental groove, and soft tissues of the neck. If the physical evaluation and clinical photographs show a minor deformity requiring augmentation with an alloplast, radiographs of the chin are usually not necessary. However, if the deformity is more complex (e.g., vertical chin excess with horizontal deficiency or transverse bony asymmetry), radiographic analysis is essential.
labiomental groove, and soft tissues of the neck. If the physical evaluation and clinical photographs show a minor deformity requiring augmentation with an alloplast, radiographs of the chin are usually not necessary. However, if the deformity is more complex (e.g., vertical chin excess with horizontal deficiency or transverse bony asymmetry), radiographic analysis is essential.
 Figure 192.1 Left: Lateral photograph of a 23-year-old patient who underwent orthodontic therapy as an adolescent. The patient’s occlusion was class I, but the skeletal chin deficiency remained. Right: Postoperative image of the patient after chin augmentation with alloplast. |
Radiographic evaluation of the chin routinely includes a panoramic radiograph (Panorex) (Fig. 192.3) and cephalometric radiographs in the AP and lateral views (Fig. 192.4A and B). The panoramic radiograph shows the cortical outline of the mandible and the vertical mandibular height. The Panorex also delineates the position of the tooth roots and of the inferior alveolar canals and mental foramina. It is important to know the exact position of the mental foramen and canal preoperatively so intraoperative damage to the mental nerve can be prevented (9). The inferior alveolar nerve, a branch of the third division of the fifth (trigeminal) cranial nerve, travels through the mandibular canal and exits the mental foramen as the mental nerve (10). The mental nerve supplies sensation to the skin and mucous membranes of the lower lip and chin. The mandibular canal is often located 2 to 3 mm below the level of the mental foramen. Bony osteotomies should therefore be performed at least 5 mm below the mental foramen to avoid injury to the neurovascular bundle.
 Figure 192.2 Upper left: A preoperative frontal photograph of a woman with mentalis muscle strain secondary to microgenia. Lower left: A lateral preoperative view is shown. Upper right: A frontal postoperative view is shown. The patient has undergone a chin augmentation with an alloplast with resolution of the mentalis strain. Lower right: A lateral view of the postoperative result is shown. |
If orthognathic surgery is considered with bony genioplasty, AP and lateral cephalometric radiographs should be performed. These radiographs allow analysis of skeletal and soft tissue key points, which can be used to predict bony movements after skeletal surgery. The AP cephalometric radiograph allows identification of transverse asymmetries of the chin. Transverse asymmetry of the chin may be associated with more global facial asymmetry (hemifacial microsomia) or with a syndrome such as oculoauricular vertebral (OAV) spectrum, or may be isolated (Fig. 192.5). It is very important to identify chin asymmetries and discuss them with the patient preoperatively. If chin augmentation is performed with an alloplast implant and the asymmetry is not considered, the asymmetry may be magnified.
Lateral cephalometric radiographs provide a soft tissue and skeletal profile upon which key landmarks can be recognized. The radiograph is with the patient’s head being stabilized with a headholder in a fixed position at a fixed distance from the radiograph machine (Fig. 192.6).
The head is stabilized with the Frankfort horizontal (from the porion [the superior aspect of the external auditory canal] to the infraorbitale [the inferior orbital rim]) being parallel to the ground. The standardized radiograph produced allows identification of a series of bony and soft tissue landmarks from which various facial analyses can be performed.
The head is stabilized with the Frankfort horizontal (from the porion [the superior aspect of the external auditory canal] to the infraorbitale [the inferior orbital rim]) being parallel to the ground. The standardized radiograph produced allows identification of a series of bony and soft tissue landmarks from which various facial analyses can be performed.
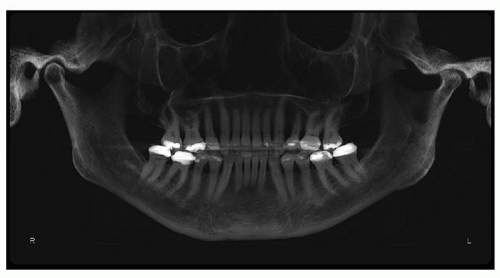 Figure 192.3 A panoramic radiograph is shown. |
The facial analyses created from the lateral cephalometric radiograph produce a two-dimensional prediction of the new postoperative chin position. Various analyses have been described including Ricketts, Burstone, Gonzalez-Ulloa and Stevens, and others. Each of these evaluation methods has positive and negative aspects. The Ricketts analysis, for instance, uses a tangent connecting the soft tissue pogonion (most projecting point) of the chin with the most projecting point of the nasal tip (Fig. 192.7). In this system, the upper lip should lie about 4 mm behind the line, whereas the lower lip is ideally located 2 mm behind the line. While the Ricketts analysis correctly evaluates the lower face in profile, it places great importance on the projection of the nasal tip. The Steiner analysis uses the columellar inflection point (“S”) to identify the correct position for the chin point (8). This method places importance on the lip position. The Holdaway “H” angle relates the position of the soft tissue pogonion with important skeletal points on the mid and lower face. No single analysis is ideal, but each method attempts to determine the “ideal” positions for the soft tissues and skeleton of the chin because these structures relate to the remainder of the face.
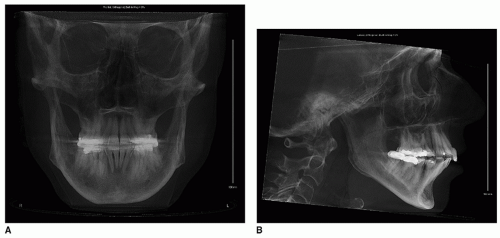 Figure 192.4 A: A frontal cephalometric radiograph is shown. B: A lateral cephalometric radiograph is shown. |
The aesthetic unit of the chin and upper and lower lips should occupy one-third of the vertical facial height (Fig. 192.8). The lower facial third height can be obtained by measuring the distance between the soft tissue subnasale and the soft tissue gnathion. If this distance is greater than one-third of the overall facial height, vertical macrogenia exists. If the distance is less than one-third of the facial height, vertical microgenia can be diagnosed. The lower facial third can be further subdivided into subunits that will indicate specifically from where the increase or decrease in vertical height originates. Two methods exist for subdivision of lower facial heights (Fig. 192.9). The first includes a vertical third from subnasale to upper lip stomion and two thirds from upper lip stomion to the menton. The second method divides the lower third into two equal parts, from the subnasale to the vermilion border of the lower lip and from the lower lip vermilion border to the gnathion. All of these analyses relate the height of the chin and lower face to the total facial height. In complex chin deformities, a vertical discrepancy as well as a horizontal deficiency or excess may often be present (Fig. 192.10).
 Figure 192.5 Photograph of a 25-year-old female with hemifacial microsomia. A vertical line has been drawn through the center of cupid’s bow of the upper lip, demonstrating how the chin deviates to the affected smaller facial side. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


