Chapter 28 Chernobyl and Radiation-Induced Thyroid Cancer
The Chernobyl (Chornobyl in Ukrainian) nuclear power station sits along the Pripyat River in northern Ukraine, near its mutual border with Belarus and the Russian Federation. In April 1986, an explosion and fire at the plant released a toxic cloud that exposed millions of people in the three countries to enormous quantities of radioactive isotopes, primarily 131I and 137Cs.1,2 The catastrophe generated an estimated 4.6 × 107 Ci of 131I, more than 3 million times greater than that released by the Three Mile Island nuclear accident (Table 28-1). Active emissions continued for almost 10 days, and the radioactive iodine made its way into cow’s milk that was consumed by children and adolescents. Because 131I has a relatively short half-life (8 days), ground activity largely disintegrated within the first few weeks. However, radioactive 137Cs, which can contribute to whole-body irradiation, has a much longer half-life (30 years) and is still measurable in soils and some foods in many parts of Europe (Figure 28-1).
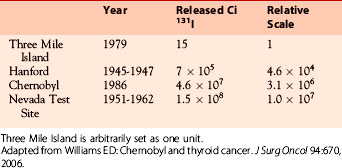
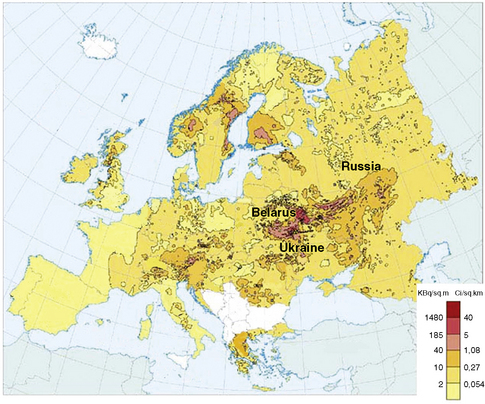
Figure 28-1 Map of ground contamination with 137Cs released by the Chernobyl accident.
(From DeCort M, et al: Atlas of caesium deposition on Europe after the Chernobyl accident, EUR report 16733, Office for Official Publications of the European Communities, Luxembourg, 1998, plate 1.)
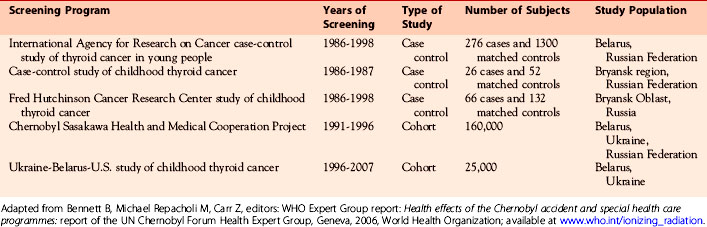
The most important health consequence of this disaster has been a measurable increase in thyroid cancer, almost exclusively of the papillary type, among those who were exposed early in life, a subject that has been extensively studied3–5 (Table 28-2). A central question surrounding this event is the exact extent to which thyroid cancer rates rose from massive radiation exposure. Because radioactive iodine isotopes are widely used in the diagnosis and treatment of thyroid disorders and are important components of fallout from future nuclear accidents or terrorist attacks, answering this question is important to both clinical medicine and public health. Therefore, the Chernobyl catastrophe provides a unique opportunity to calculate the risk of thyroid cancer following exposure to radioactive iodine, understand the mechanisms of radiation-induced thyroid cancer, and make rational recommendations concerning follow-up and treatment of vulnerable populations.
Epidemiology of Radiation-Induced Thyroid Tumors
The thyroid is among the most radiosensitive organs, and external irradiation is recognized to increase the risk of both thyroid cancer and follicular adenoma, particularly if exposure occurs early in life.6,7 At the time of the Chernobyl accident, however, it was not clear that internal irradiation with radioactive iodine posed the same risk as x-rays. Previous experience from the Marshall Islands and Hanford nuclear facility had found that the risk of thyroid cancer was not significantly increased among populations exposed to fallout containing radioactive isotopes of iodine.8,9 Studies of the Nevada Test Site had shown a significant increase in thyroid tumors (both benign and malignant) in exposed children, but for cancers alone the increase was not statistically significant.10–12 In addition, among almost 5000 children under 18 years of age administered 131I for diagnostic purposes at a median dose of 1 Gy (100 rads), there was no increased risk of thyroid cancer.13
Thyroid Cancer
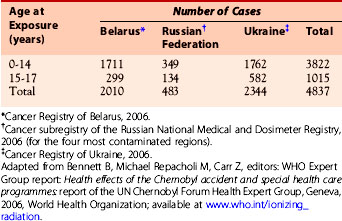
The first accounts of a significant increase in thyroid cancer were published only 6 years after the accident, indicating a very short latency compared to that for external exposure, which is typically a decade or more.14,15 Subsequent reports confirmed the cancer epidemic, and a World Health Organization (WHO) expert group estimated that more than 4000 new cases of thyroid cancer occurred between 1986 and 2002 among those who were children or adolescents at the time of the accident.16 According to the national cancer registry data accumulated during this same time period, nearly 5000 cases of pediatric thyroid cancer were diagnosed and treated in Belarus, Ukraine, and the most contaminated regions of Russia (Table 28-3). The highest frequency was registered in Belarus, where the incidence rate rose from 0.085 cases of thyroid cancer per 100,000 children/year in 1986, which is comparable to that observed in Western countries, to 4 per 100,000/year in 1993, and in the heavily contaminated Gomel region it was 12.6 per 100,000/year by 1996.
Table 28-3 Number of Pediatric Thyroid Cancer Cases Diagnosed between 1986-2002 in Belarus, the Russian Federation, and Ukraine According to Age at Exposure
Although several early analyses suggested an association between radiation dose and thyroid cancer, they were based on estimated doses and were limited by a retrospective design.17–20 Recently, a large, prospective cohort study of Ukraine children less than 18 years of age at exposure found a strong, positive, and approximately linear increased risk of thyroid cancer with doses based on individual measurements obtained within several weeks of the accident.21 In addition, it was observed that the carcinogenic effects of childhood exposure to 131I were not appreciably different than those of therapeutic x-irradiation6,21 (Table 28-4). A follow-up to this study reported that increased cancer risk persisted for two decades after exposure without evidence of decrease during the observation period.123
Table 28-4 Comparison of the Oncogenic Effects of External X-ray Exposure to Those of Internal 131I Exposure during Childhood6,15,51,52

Risk Modification
Several factors have been found to modify the risk of thyroid cancer developing after Chernobyl, most importantly age, gender, and iodine intake. Similar to what has been reported for externally irradiated subjects,6,22 younger age at exposure has been linked to increased risk for Chernobyl cancers,16,23,24 and most, but not all, studies have shown an excess risk for females.13,23–26 However, unlike the effects of age and gender, the modifying effects of iodine nutrition on radiation-induced thyroid cancer are less certain.
Age at Exposure
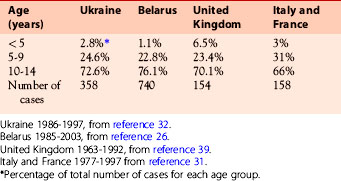
Sporadic pediatric thyroid cancer (that is not associated with radiation exposure) is uncommon (see Chapter 27, Pediatric Thyroid Cancer).27–30 For example, in the United States the rate among prepubertal subjects is less than 1 per million population per year, whereas among adolescents it is only 18 per million.30 By contrast, a remarkable number of the Chernobyl cancers have occurred among younger children.31–33 In Belarus and Ukraine, nearly 1100 children younger than age 14 years were operated on for thyroid cancer from 1985 to 2003 out of a combined population of only 60 million people. In Western countries, many fewer cases have occurred over a much longer period of time and from a much larger population (Table 28-5). In Ukraine, during the 5 years preceding the accident there were only 25 cases of thyroid cancer in subjects up to age 14 years compared to 358 between 1986 and 1997.32 In Belarus, 740 children were operated on from 1985 to 2003, and over three quarters were age 10 to 15 years.33
The risk of thyroid cancer among irradiated adults is uncertain, largely because information is limited. An international study of women treated for cervical cancer found a nonsignificant increased risk of thyroid cancer following an estimated average dose of only 0.11 Gy (11 rads).34 In atomic bomb survivors externally exposed to gamma rays and neutrons at a mean thyroid dose of 0.27 Gy, the cancer risk was increased across all age groups but was significantly lower for adults than for children.35 Although an early Russian report found a positive relationship between dose and thyroid cancer among Chernobyl cleanup workers (“liquidators”), a subsequent analysis found no association between exposure and cancer among subjects who were 15 to 69 years of age at the time of the accident.36,37 Therefore, at the present time it is unclear if adult exposure to radioactive iodine at Chernobyl has increased the risk of thyroid cancer.
Gender
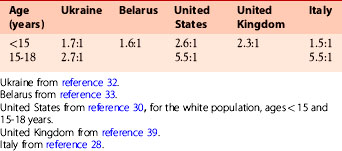
Another potential difference between Chernobyl cancers and those occurring in Western countries is the gender ratio. For sporadic pediatric thyroid cancers, the ratio of girls to boys is lower before puberty than it is during adolescence.38 In a large series of unexposed English children younger than age 15 years of age at operation, the overall female-to-male ratio was 2.3:1; in children under age 10 years it was 1.2:1, and in older children it was 3.6:1, similar to an adult ratio.39 However, the gender ratio does not appear to rise as quickly with age in Chernobyl children (Table 28-6). In Belarus, the gender ratio was 1.6:1 for subjects under 15 years of age, whereas in Ukraine it was similar (1.7:1) for young children and only slightly higher (2.7:1) for those aged 15 to 18 years.32,33 In another large Ukrainian study of subjects aged 14 to 32 years at operation it was 2.1:1, suggesting that radiation exposure may blunt the rise in the gender ratio that normally occurs with older age.23
Iodine Nutrition
Because iodine plays a central role in normal thyroid homeostasis, iodine nutrition could affect oncogenesis both at exposure, by influencing the amount of 131I taken up by the gland, and at a later time, by altering the response to the initial radiation damage. The dose of radioactive iodine received by the thyroid is directly proportional to the quantity of contaminated material ingested and the percentage uptake, and it is inversely proportional to the size of the gland.40 By increasing 131I uptake, chronic iodine deficiency would increase the dose delivered, whereas enlargement of the gland because of endemic goiter would decrease the dose. However, which of these competing influences was the more important is currently unknown.
There is theoretic evidence that iodine deficiency might also increase the sensitivity of thyroid follicular cells to the damaging effects iodizing radiation.41 By decreasing the formation of reactive oxygen species created by hydrogen peroxide, iodine acts as an antioxidant and diminishes the risk of DNA damage from free radicals formed during thyroid hormone synthesis.42 Stimulation of the gland by increased thyrotropin levels caused by iodine deficiency could augment radiation effects through increased generation of these reactive molecules long after initial exposure.
Iodine deficiency is endemic in the Chernobyl regional. Clinical investigations carried out between 1930 and 1950 documented a high prevalence of endemic goiter among residents of northern Ukraine and southern Belarus, especially in the Gomel region43 Although the introduction of iodized salt during the 1950s led to a significant decline in the goiter rate, less importance was being placed on iodine nutrition by the time of the accident.44 Coincident with the rise in the number of thyroid cancers, renewed attention was given to iodine intake during the 1990s. Studies in children suggested mild to moderate deficiency throughout Belarus, although Gomel may have been less severely affected than other areas.45,46 The areas of the northern Ukraine affected by the accident may have had even higher rates of iodine insufficiency.47 Mandatory salt iodization programs in Belarus and Ukraine during 2000-2001 have addressed this problem, and there is reliable evidence that iodine nutrition is now improving.48
Although it has been theorized that iodine insufficiency could influence the incidence of Chernobyl cancers, investigations have produced conflicting results.49 Case-control studies done in Belarus and the Russian Federation reported an inverse relationship between the risk of radiation-induced tumors and iodine intake both at the time of the accident and many years later.19,50 (Table 28-7). However, the UkrAm study found no association of cancer risk with either diffuse goiter, evidence of past iodine deficiency, or urinary iodine concentration, an indicator of iodine intake at the time of screening.21

Follicular Adenoma
Benign follicular adenomas have also increased in frequency following the Chernobyl accident, similar to what was observed in subjects externally irradiated during infancy and early childhood.7,51 A recent report from UkrAm found that although the dose-response relationship for follicular adenoma was linear, the excess relative risk was somewhat lower than for cancer in the same cohort (2.07 versus 5.25 per gray).52 The risk was higher for women than for men, but there was no significant difference according to age at exposure (see Table 28-4). However, it should be kept in mind that the latency for follicular adenomas that developed after external radiation exposure was longer than for cancers, so these findings should be regarded as preliminary and may change with longer periods of observation.
Pathomorphology and Mechanisms of Radiation-Induced Thyroid Cancer
As noted previously, papillary carcinoma is the main type of thyroid cancer in populations exposed to radiation after the Chernobyl accident, similar to what was found in patients exposed to external therapeutic irradiation and in atomic bomb survivors in Japan. Papillary carcinomas constitute approximately 95% of all thyroid cancers diagnosed in children and adolescents from different areas around Chernobyl. In Belarus, the prevalence of this tumor type was 94% to 96% in two large series of patients exposed early in life, whereas follicular carcinoma constituted only 5%.31,53 In the contaminated areas of Ukraine, 93% to 95% of childhood thyroid cancers were papillary carcinomas.32,54 By comparison, among sporadic tumors in children and adolescents in two European counties, papillary carcinoma comprised 82% of thyroid cancer cases, whereas follicular carcinoma was found in 15% of cases.31 This correlates with the general prevalence of papillary carcinomas in other countries such as the United States, where papillary carcinomas account for approximately 80% of all thyroid tumors.30,55,56
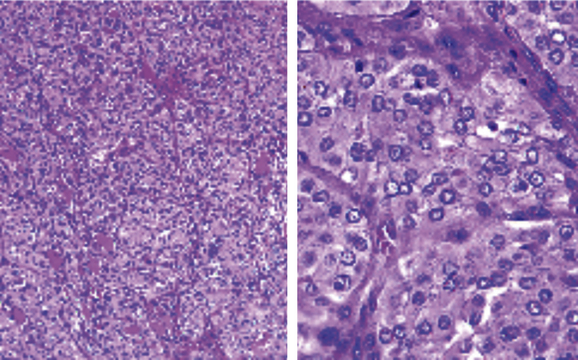
Many post-Chernobyl papillary carcinomas had an unusual microscopic appearance. Although the tumor cells demonstrated all diagnostic nuclear features of papillary carcinoma (such as enlarged, oval nuclei with irregular nuclear contours; nuclear grooves and pseudo-inclusions; and chromatin clearing), they did not form classic papillary structures and instead grew in solid sheets admixed with a variable component of neoplastic follicles (Figure 28-2).57,58 Because of the predominance of the solid growth pattern and the absence of well-formed papillae, these tumors were classified as the solid or solid-follicular variant of papillary carcinoma. Following Chernobyl, the solid variant was observed in approximately 30% of papillary cancers, and another one third showed predominantly a follicular growth pattern with a minor but substantial component of solid growth32,57,59 The solid-follicular morphology was particularly common in those exposed at a very young age (0 to 2 years).60 In contrast, the solid variant is rare in a general population, comprising only 1% to 2% of papillary carcinomas in both children and adults.61,62 As discussed later in this chapter, among the Chernobyl cancers the solid variant had a strong correlation with a specific type of genetic alteration (i.e., RET/PTC3 chromosomal rearrangement).
Many papillary thyroid carcinomas that developed after Chernobyl had a number of histopathologic features that are typically associated with more aggressive biologic behavior. When compared to cancers in children with no radiation history from two European countries, the post-Chernobyl tumors had a significantly higher frequency of extrathyroidal extension (49% versus 25%) and of lymph node metastases (65% versus 54%),31 but they had a similar rate of distant lung metastases. Other studies have reported an even higher frequency of extrathyroidal tumor spread,57,59 particularly in association with a younger age at the time of exposure and a short latency period (time from exposure to operation).53,60 The common finding of wide tumor invasion with spread to the regional lymph nodes, together with a higher frequency of the solid growth pattern that was interpreted by some pathologists as evidence for tumor dedifferentiation, raised the possibility that these radiation-associated tumors might be prone to aggressive clinical behavior. However, to date this has not been confirmed. Out of more than 4000 patients with thyroid cancer who were exposed to radiation during childhood and diagnosed with cancer by 2002, only 15 deaths resulting from progression of the disease have been documented so far.16,63,64 This correlates with the results of other studies that reveal an overall favorable prognosis and low mortality rate of thyroid cancer in children, despite a high frequency of extrathyroidal extension and lymph node metastases observed in this age group (see Chapter 27, Pediatric Thyroid Cancer).65–67 There are also reports that Chernobyl cancers with longer latency are better differentiated and show less aggressive features at presentation.60



