Vestibular schwannomas (VS) are among the most common benign tumors of the central nervous system. Bilateral VS are the hallmark of neurofibromatosis type II, commonly leading to complete deafness and cranial nerve deficits as a result of tumor progression or treatment with surgery or radiation. Effective medical therapies are needed to address tumor progression and treatment-related morbidity. This article reviews the standard therapies for VS, summarizes the molecular biology of these tumors, and describes potential targets for chemotherapeutic agents. The article also defines and recommends the use of specific clinical end points in future drug trials, describes previous and current experience with anti-VEGF and anti-EGFR agents, and delineates areas of future research.
| ADC | Apparent diffusion coefficient |
| CML | Chronic myelogenous leukemia |
| CNS | Central nervous system |
| HER | Human epidermal growth factor receptor |
| FSRT | Fractionated stereotactic radiotherapy |
| NF2 | Neurofibromatosis type 2 |
| PDGFR | Platelet derived growth factor receptors |
| VEGF | Vascular endothelial growth factor |
| VS | Vestibular schwannoma |
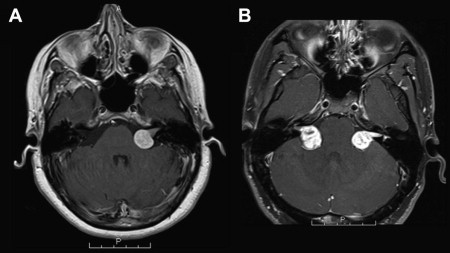
Bilateral VS are the hallmark of neurofibromatosis type 2 (NF2), an autosomal-dominant tumor suppressor syndrome characterized by multiple schwannomas, meningiomas, and ependymomas (see Fig. 1 B). The incidence of NF2 is approximately 1 per 25,000 live births and accounts for 2% to 7% of patients with VS, depending on methodology. Because of their location, bilaterality, and inexorable growth, NF2-related VS eventually lead to clinically meaningful hearing loss, cranial nerve deficits, and brainstem compression. Moreover, these patients often experience hearing loss as a result of surgery or radiation treatment. Overall life expectancy in NF2 is greatly diminished, with older literature suggesting that 60% of patients die before age 44. Indeed, disease-specific mortality in NF2 is greater than 90%, with nearly all deaths occurring as a direct result of tumor growth (causing brainstem compression and eventual hydrocephalus) or complications of treatment.
In addition to the increased mortality of NF2, the bilateral nature of VS in this disorder leads to significant long-term morbidity and decreased quality of life caused by lower cranial nerve problems, including deafness, swallowing problems, facial diplegia, dysarthria, and aspiration pneumonia. Treatment-related morbidity is also higher in NF2-related VS, because of the bilateral nature of the problem and because nerve fibers are considered more likely to run through NF2-associated schwannomas, rather than lying on the surface as in sporadic VS.
Given the morbidity and mortality of NF2-associated VS and the high risks of surgical treatment or radiation therapy, medical therapies that can slow or arrest tumor growth are urgently needed. Recently, a consensus conference recognized that rationally designed phase II clinical trials were a realistic short-term goal in treating NF2-related VS. This article reviews the current standard therapies for VS, describes previous experience with chemotherapy, and delineates areas of current and future research.
Standard treatments for VS
Observation for VS
Progressive growth of tumors in the cerebellopontine angle carries a high rate of morbidity, with cranial nerve problems (including hearing loss), brainstem or cerebellar compression, and eventually hydrocephalus from compression of the fourth ventricle. However, the natural history of VS is unpredictable, especially for sporadic VS. Tumors may grow at a steady rate, plateau at a certain size, or rarely even shrink. Additionally, tumors may recur after treatment. Given the increasing availability of cranial imaging and the high resolution now available in routine brain MRIs, diagnosis of small VS has now become commonplace.
Several studies have attempted to elucidate the natural history of VS. The largest to date is a prospective evaluation of tumor growth data from more than 500 patients in the Danish national registry, followed for a median of 3.6 years. During the follow-up period, 17% of tumors confined to the internal acoustic meatus grew, compared with 29% of extrameatal tumors. No relationship between tumor growth and patient gender or age could be determined. The same registry was used to assess changes in hearing over time in patients allocated to expectant management strategies. Patients received annual audiologic and MRI examinations. At the outset of the study, 53% of patients had speech discrimination of greater than 70%; at the end of the 10-year observation period, this rate had fallen to 31%. Patients with hearing that was initially good maintained their hearing at higher rates than patients with impaired hearing at baseline.
These results seem to confirm that primary observation is justified for smaller, asymptomatic tumors. Indeed, a “watchful waiting” approach is common in clinical practice, particularly given the relatively slow growth of most VS and high risk of treatment-related morbidity including complete hearing loss. Larger, symptomatic tumors, or those with substantial cystic components, are often removed because they are more likely to cause morbidity related to progressive growth, and surgery becomes more challenging and risky with larger tumors. Thus, the chosen therapeutic approach may depend on the clinician’s interpretation of the evidence for ongoing tumor growth. Consensus recommendations vary, but commonly use a tumor size threshold of 20 mm and a growth rate of greater than 2 mm per year (based on increase in the largest dimension) for recommendation of treatment. At this size, further growth may compromise cranial nerve function, and may also make future surgery more difficult. Additionally, an actively growing tumor is more likely to result in progressive hearing decline over time, especially if the tumor is already large at diagnosis.
Surgery for VS
The decision to manage VS surgically is often straightforward for large, symptomatic tumors and those causing brainstem compression or hydrocephalus. However, surgery is frequently performed for smaller, asymptomatic tumors. The most compelling argument for surgery is the theoretical risk of progressive hearing deterioration over time. Larger tumors are particularly problematic to manage conservatively. Based on what is known about the natural history of VS, progressive hearing loss is more likely with rapidly growing tumors, especially those that are large at baseline. The morbidity of surgery increases with tumor size, because of the difficulties of exposure including cerebellar retraction and facial nerve damage. These issues arise frequently in surgical treatment of NF2-related VS, because they have a markedly faster growth rate than seen in sporadic VS and may present at a larger size. Additionally, NF2 patients with bilateral VS may already have impaired hearing in one or both ears, raising the stakes for a high-risk surgery. Although hearing may stabilize with either surgery or radiation therapy, it usually does not improve.
As is the case for many complex, high-risk surgical procedures, outcomes for surgical treatment of VS are superior at larger institutions with more experienced, specialized surgeons. A retrospective cohort study of 2643 operations selected from a large national administrative database demonstrated a significant volume-outcome relationship for VS resection when adjusting for potential confounders such as age, gender, race, payor (type of insurance), geographic region, procedure timing, admission type and source, medical comorbidities, and NF status. Postoperative complications including neurologic deficits, prolonged mechanical ventilation, facial nerve injury, and need for blood transfusion were less frequent at higher-volume hospitals or with higher-volume surgeons. Furthermore, length of stay was shorter, hospital charges were less, and perioperative mortality was reduced. The potentially high risks of short- and long-term morbidity from VS surgery and the relatively small number of tertiary care centers that have the requisite caseload and surgical experience to manage these risks further complicate the delivery of care for patients with VS, not all of whom have access to these settings.
Radiation Therapy for VS
Radiation is often used as adjuvant therapy for treatment of sporadic brain tumors. As the other mainstay of treatment for VS, radiation therapy can help avoid some of the morbidities associated with surgery. Although many larger VS are believed to be poor candidates for radiotherapy because of the concomitant risks of swelling near the brainstem, recent technical advances including fractionated radiation and radiosurgery have been used with some success to treat smaller tumors. However, outcomes for NF2-related VS are generally worse than those for sporadic VS.
In particular, fractionated stereotactic radiotherapy (FSRT) has been advocated to minimize the risk of hearing loss. A recent series of 106 patients treated with FSRT demonstrated excellent local tumor control (94% at 3 years and 93% at 5 years). Notably, the “useful” hearing preservation rate was 98% at 5 years in patients without NF2 but only 64% in patients with NF2. The median irradiated tumor volume was small (3.9 cm 3 ), although the maximum tumor volume was greater than 30 cm 3 . FSRT was generally well tolerated, with a low incidence of cranial neuropathies including radiation-induced toxicity to the trigeminal and facial nerve (<5%).
Another series of 190 previously untreated patients with unilateral VS examined the efficacy and complication rate of gamma knife radiosurgery. The 5-year tumor control rate, as defined by no requirement for surgical intervention, was 97%. Patients had low rates of radiation-induced cranial neuropathies, although increasing marginal radiation dose did lead to higher rates of facial nerve weakness and decreased preservation of speech discrimination. Hearing-level preservation was 71% and preservation of speech discrimination was 91%, although the authors do not stratify by NF2 status; most patients in the sample had unilateral VS, which were more likely to be sporadic. As with surgery, hearing improvement was rare (7%), although many patients preserved their pretreatment hearing status.
In patients with smaller tumors, or in older patients with medical comorbidities, radiosurgery or FSRT may be an attractive alternative to neurosurgery, with lower rates of treatment-associated cranial neuropathies. Additionally, radiosurgery avoids problematic perioperative complications such as infection and cerebrospinal fluid leak. Patients successfully treated with radiotherapy may be able to avoid surgery in the future. However, for larger tumors, radiotherapy is often impractical or unsafe. In the NF2 population, the risk of secondary malignancy after radiation is a particular concern. These patients are usually younger than sporadic patients at the time of treatment (with more time to develop a malignancy) and have a genetic predisposition to tumor formation.
Molecular biology in VS
Given the high treatment-related morbidity of VS especially in NF2 patients, developing innovative and effective medical therapies is a high priority. For more than 10 years, development of promising chemotherapeutic agents has mainly focused on finding appropriate molecular targets based on the tumor’s underlying biology. Drugs developed in this way have become the mainstay in treating breast cancer, chronic myelogenous leukemia, and other malignancies, with a resulting dramatic improvement in outcomes for some conditions. This section reviews the molecular biology of VS and describes its relevance to treatment; in addition, past and current uses of chemotherapeutic agents against VS are discussed and possible areas of future innovation are described.
NF2-related and sporadic VS demonstrate loss of the NF2 gene product Merlin, a tumor-suppressor protein. Merlin interacts with various receptor tyrosine kinases, including the human epidermal growth factor (HER) family, platelet-derived growth factor receptors (PDGFR), and c-KIT, thereby inhibiting their signaling. In human and Drosophila models, Merlin has been shown to control the surface availability of the HER-1/EGFR, HER-2, HER-3, and PDGF receptors. Amplification of HER-1/EGFR, HER2, or PDGFR, an established mechanism of tumorigenesis in sporadic cancer, is not present in human VS specimens. Cultured NF2 -deficient cells lack contact inhibition, an effect likely mediated by HER-1/EGFR signaling. Overall, the loss of functional Merlin leads to dysregulation of a pathway associated with contact-dependent inhibition in normal Schwann cells, ultimately leading to tumorigenesis and continued growth of VS.
HER-2 signaling seems to be necessary for Schwann cell differentiation and proliferation, and activated HER-2 and HER-3 are abundantly expressed in sporadic and NF2-related VS. In an immunohistochemical analysis of 38 VS specimens, HER-2 was upregulated in 76% of sporadic and 94% of NF2-related VS. Importantly, EGF ligand was upregulated in 100% of NF2-related VS, but not in sporadic VS. HER-1/EGFR expression levels correlated directly with VS tumor size and inversely with patient age. Similarly, PDGFRB is overexpressed in Schwannoma cells and, when stimulated by the ligand PDGF, has a mitogenic effect on tumor cells.
Vascular endothelial growth factor (VEGF) is a mediator of angiogenesis and vascular permeability. Its activity is mediated by the receptor tyrosine kinases VEGFR1 and VEGFR2 and by the neuropilins NRP1 and NRP2. In the peripheral nervous system, semaphorins serve as negative regulators of the VEGF pathway and act through the neuropilin receptors. VEGF and the receptor VEGFR1 have been detected in sporadic and NF2-associated schwannomas, with increased levels correlating with increased rates of tumor growth. In a separate study, the expression pattern of VEGF and its receptors VEGFR2, NRP1, and NRP2 was determined in tissue samples from sporadic and NF-associated VS. VEGF was expressed in all VS and VEGFR2 in almost a third of tumor vessels. Evidence from a transgenic mouse model shows that anti-VEGF agents bevacizumab and vandetanib can increase apoptosis, reduce tumor growth rate, and increase survival in rodents with intracranial schwannomas. By using microscopy and whole-body imaging techniques, Wong and colleagues demonstrated that these anti-VEGF agents decreased vessel permeability, thereby normalizing the vasculature of schwannoma xenografts in nude mice. The authors hypothesize that this occurs because the natural balance between VEGF and semaphorin 3 signaling is re-established. This antivascular effect may be the mechanism by which anti-VEGF therapies cause death of tumor cells and thereby delay progression.
These findings have spurred great interest in the development of targeted molecular therapies for the treatment of VS. According to a recent consensus conference, the HER family of receptors in particular is thought to furnish the most compelling target for rationally designed drug therapy. HER-1/EGFR inhibitors, such as erlotinib, and the anti-VEGF agent bevacizumab have also been recently studied. Specific findings and current research are discussed later.
Molecular biology in VS
Given the high treatment-related morbidity of VS especially in NF2 patients, developing innovative and effective medical therapies is a high priority. For more than 10 years, development of promising chemotherapeutic agents has mainly focused on finding appropriate molecular targets based on the tumor’s underlying biology. Drugs developed in this way have become the mainstay in treating breast cancer, chronic myelogenous leukemia, and other malignancies, with a resulting dramatic improvement in outcomes for some conditions. This section reviews the molecular biology of VS and describes its relevance to treatment; in addition, past and current uses of chemotherapeutic agents against VS are discussed and possible areas of future innovation are described.
NF2-related and sporadic VS demonstrate loss of the NF2 gene product Merlin, a tumor-suppressor protein. Merlin interacts with various receptor tyrosine kinases, including the human epidermal growth factor (HER) family, platelet-derived growth factor receptors (PDGFR), and c-KIT, thereby inhibiting their signaling. In human and Drosophila models, Merlin has been shown to control the surface availability of the HER-1/EGFR, HER-2, HER-3, and PDGF receptors. Amplification of HER-1/EGFR, HER2, or PDGFR, an established mechanism of tumorigenesis in sporadic cancer, is not present in human VS specimens. Cultured NF2 -deficient cells lack contact inhibition, an effect likely mediated by HER-1/EGFR signaling. Overall, the loss of functional Merlin leads to dysregulation of a pathway associated with contact-dependent inhibition in normal Schwann cells, ultimately leading to tumorigenesis and continued growth of VS.
HER-2 signaling seems to be necessary for Schwann cell differentiation and proliferation, and activated HER-2 and HER-3 are abundantly expressed in sporadic and NF2-related VS. In an immunohistochemical analysis of 38 VS specimens, HER-2 was upregulated in 76% of sporadic and 94% of NF2-related VS. Importantly, EGF ligand was upregulated in 100% of NF2-related VS, but not in sporadic VS. HER-1/EGFR expression levels correlated directly with VS tumor size and inversely with patient age. Similarly, PDGFRB is overexpressed in Schwannoma cells and, when stimulated by the ligand PDGF, has a mitogenic effect on tumor cells.
Vascular endothelial growth factor (VEGF) is a mediator of angiogenesis and vascular permeability. Its activity is mediated by the receptor tyrosine kinases VEGFR1 and VEGFR2 and by the neuropilins NRP1 and NRP2. In the peripheral nervous system, semaphorins serve as negative regulators of the VEGF pathway and act through the neuropilin receptors. VEGF and the receptor VEGFR1 have been detected in sporadic and NF2-associated schwannomas, with increased levels correlating with increased rates of tumor growth. In a separate study, the expression pattern of VEGF and its receptors VEGFR2, NRP1, and NRP2 was determined in tissue samples from sporadic and NF-associated VS. VEGF was expressed in all VS and VEGFR2 in almost a third of tumor vessels. Evidence from a transgenic mouse model shows that anti-VEGF agents bevacizumab and vandetanib can increase apoptosis, reduce tumor growth rate, and increase survival in rodents with intracranial schwannomas. By using microscopy and whole-body imaging techniques, Wong and colleagues demonstrated that these anti-VEGF agents decreased vessel permeability, thereby normalizing the vasculature of schwannoma xenografts in nude mice. The authors hypothesize that this occurs because the natural balance between VEGF and semaphorin 3 signaling is re-established. This antivascular effect may be the mechanism by which anti-VEGF therapies cause death of tumor cells and thereby delay progression.
These findings have spurred great interest in the development of targeted molecular therapies for the treatment of VS. According to a recent consensus conference, the HER family of receptors in particular is thought to furnish the most compelling target for rationally designed drug therapy. HER-1/EGFR inhibitors, such as erlotinib, and the anti-VEGF agent bevacizumab have also been recently studied. Specific findings and current research are discussed later.
End points for clinical trials
After a promising agent for a molecular target is identified, it must be tested in a well-designed clinical trial. One of the primary challenges in designing and conducting clinical trials is the choice of end points that are clinically appropriate, objectively measurable, and reproducible by other researchers. In the past, there has been a lack of consensus on end point standardization in the treatment of VS. In 2009, the authors’ group at Massachusetts General Hospital (MGH) proposed a set of suggested response criteria to define end points for future phase II studies of anticancer drugs in VS. By using objective and predefined criteria, important primary and secondary outcomes can be described (eg, time to tumor progression, hearing loss, or subjective symptoms) and related to patient prognostic factors, such as age, baseline tumor size, and tumor growth rate.
Hearing End Points
Hearing preservation is of crucial importance to patients, particularly those with NF2 who have bilateral tumors and frequently experience the loss of all usable hearing within their lifetimes as a result of tumor growth or treatment. Because most NF2 patients are diagnosed well after their acquisition of language, this hearing loss has a profound effect on their quality of life, social skills, and ability to function at home and in the workplace. Subjective measures of hearing, although they may be highly relevant to the patient’s perceived symptoms and quality of life, are problematic for use as a primary outcome in a clinical trial.
Several methods have been suggested for the objective measure of changes in hearing, although no single method has been adopted for routine use in drug trials. The standard audiogram commonly incorporates the ability to detect sound (pure tone threshold) and speech discrimination (word recognition score based on standardized lists of words). For example, the American Academy of Otolaryngology recommends testing pure tone thresholds at levels of 0.5, 1, 2, and 3 kHz, and testing speech discrimination scores at up to 40 dB above the speech discrimination threshold using a 50-word recorded list in the subject’s native language. A composite hearing scale, the Gardner-Robertson classification, is sometimes used to report changes in hearing after treatment with open surgery or radiosurgery, combining pure tone threshold and word recognition into a four-level scale. However, this scale lacks sensitivity because of “floor effects” for those in lower categories (classes III, IV, and V), in which NF2 patients are more likely to fall. Time to hearing loss or failure has been proposed as an end point for clinical trials, but given the difficulty of assessing subjects with severely impaired hearing at baseline and the long follow-up times required, it may be impractical to use as a primary outcome.
The authors suggest that maximum word recognition scores be used as the primary hearing end point in phase II clinical trials for anti-VS drugs. Word recognition affects basic communication more profoundly than does pure tone threshold. VS have a propensity to cause auditory nerve dysfunction because of direct pressure and secondary degeneration of the cochlea. Indeed, hearing aids, although they decrease the pure tone threshold, are often of little benefit for patients with NF2 and bilateral VS, because sound amplification alone does not address the underlying auditory nerve dysfunction.
Finally, recent evidence on drug therapies for VS suggests that patients treated with targeted agents can experience measurable and clinically meaningful improvement in their hearing even in the absence of a radiographic response or with progressive disease as measured by MRI scan (discussed next). This may be caused by the amelioration of the auditory nerve dysfunction caused by tumor growth and tumor-associated edema. Intuitively, a clinically meaningful improvement in hearing is the most important outcome from the perspective of a patient agreeing to participate in a clinical trial, and probably the most objective and reliable way to achieve this is by measuring the word recognition score.
Radiographic End Points
Traditionally, changes in contrast enhancement on MRI or CT have been used to define objective radiographic tumor response to treatment. The neuro-oncology literature includes several novel modalities to measure radiographic response of malignant CNS tumors, including diffusion or perfusion changes in MRI imaging. However, as with most benign CNS tumors, these methods have not been validated in either sporadic or NF2-related VS.
Historic methods of measuring tumor size and response, such as the 1981 World Health Organization criteria, revised in 2000 as the RECIST criteria, and the Macdonald criteria for malignant glioma, have all been used in the VS literature. Linear growth (based on largest tumor dimension) is often used as a treatment recommendation threshold, most commonly 2 mm per year. However, NF2-related VS in particular are often larger and have a more irregular shape than sporadic VS, so linear dimension, whether unidimensional or bidimensional, is less likely to be an adequate surrogate for volume. More recently, and with the advent of higher-resolution MRI imaging, volumetric measurement has become the accepted method of defining radiographic response. Using 3-mm axial slices through the internal auditory canal produces the greatest accuracy, with an intrarater coefficient of variation of less than 5% for tumors larger than 1 cm 3 . In a recent paper on suggested response criteria, the authors suggest volumetric methods, with an objective radiographic response defined as a 20% or greater reduction in VS volume based on postcontrast T1-weighted MRI images collected with 3-mm or finer cuts through the internal auditory canal.
Radiographic tumor response has been successfully used in phase II chemotherapy trials of various cancers. The underlying assumptions are that most chemotherapeutic drugs work by a cytotoxic mechanism, resulting in radiographic shrinkage, and that objective decrease in tumor size is related to other end points, such as overall survival or progression-free survival, that are clinically relevant to patients. However, some agents are postulated to have cytostatic, rather than cytotoxic, effects, and may result in radiographic stabilization (or decrease in growth rate) rather than overt shrinkage. For sporadic VS, spontaneous involution occurs in approximately 8% of tumors, usually during a long period of observation given their slow growth rate. However, this rarely occurs in NF2-related tumors; in a recent analysis, only 3 (3.6%) of 84 tumors regressed by 2 mm or more during 9 months to 2 years of follow-up, suggesting that any objective radiographic shrinkage of NF2-related schwannomas would be caused by drug activity and not by spontaneous involution.
It is well known that contrast enhancement may be misleading, reflecting radiation necrosis or “treatment effect” rather than tumor growth. In such cases, time to disease progression, rather than objective radiographic response, may be a more reliable indicator of the drug’s clinical efficacy. Indeed, progression-free survival at 6 months is now a frequently used primary end point in drug trials for recurrent malignant glioma. Although histologically benign, given their problematic location and rapid growth, it is appropriate to consider NF2-related VS in a similar clinical category as malignant CNS tumors. In this setting, determination of progression-free survival at 12, 24, and 60 months would provide meaningful clinical information about drug activity for VS.
A final consideration relevant to NF2-related VS is the presence of multiple lesions. In principle, one target lesion (usually the largest or most symptomatic lesion) should be selected as the lesion of interest for assessing the primary end point of radiographic response. In NF2-related VS, this can be difficult because of the irregularity of the tumors, changes in previously treated tumors, and the presence of multiple or confluent tumors.
Tinnitus and Other End Points
In addition to the possible primary end points described previously, the design of future clinical trials should take into consideration subjective improvement in patient symptoms. Among the most bothersome of these symptoms is tinnitus. As with many subjective symptoms, there is no diagnostic test for tinnitus. Measurement of tinnitus is complicated by the fact that it is an extremely common symptom, with up to a third of the adult population reporting it at some point, although few individuals experience symptoms significant enough to affect their quality of life. An individual’s subjective emotional and psychologic responses to tinnitus can also affect its perceived severity, making an objective measurement more difficult.
Tinnitus can be a sensitive indicator of cochlear dysfunction. It can encompass the clinical spectrum from barely noticeable “white noise” to troublesome or even distressing whistling and ringing that can be heard despite loud background noise. In VS, as in Meniere’s disease, it may correlate with hearing loss, although it may fluctuate less as hearing loss progresses. A clinical grading system for tinnitus has been proposed, assigning a value of 0 to 3, which incorporates degree of severity and continuity versus fluctuation. More recently, a five-point severity grading scale (slight, mild, moderate, severe, and catastrophic) has been proposed, but no one system has been accepted for general use in clinical trials. In their studies, the authors have used a grading scale along with the Tinnitus Reaction Questionnaire, which assesses the psychologic distress associated with tinnitus.
Vertigo and balance problems are common in NF2 patients with bilateral VS, but are notoriously difficult to measure objectively. Although there is a well-validated objective scale for facial nerve palsy, the House-Brackmann scale, facial nerve dysfunction is often a consequence of surgical treatment rather than of the natural history of the disease. The same is true of trigeminal nerve dysfunction. Therefore, these entities are unlikely to be used as primary clinical end points, although they certainly have a profound influence on the patient’s overall quality of life.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


