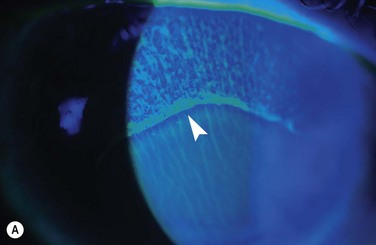
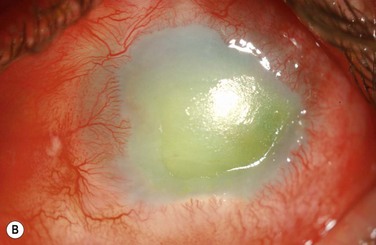
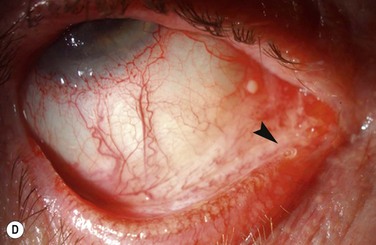
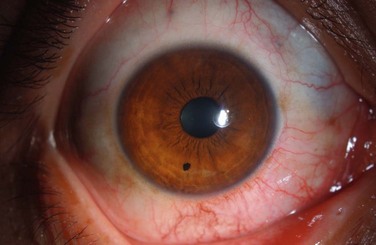
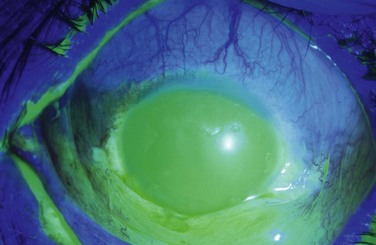
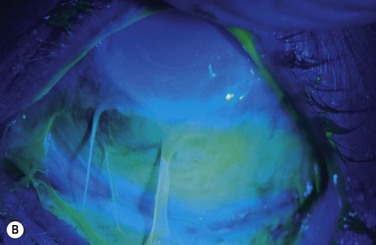
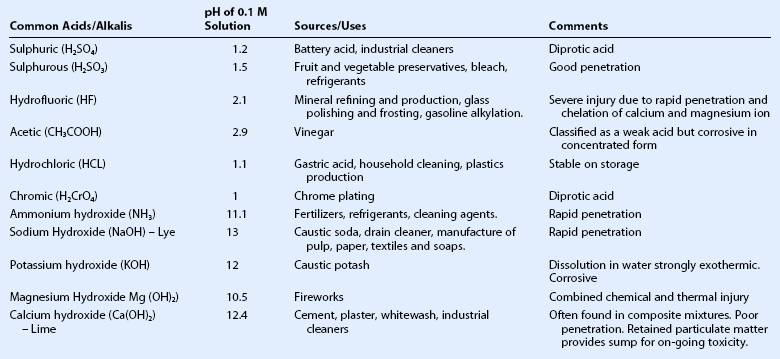
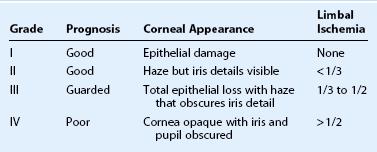
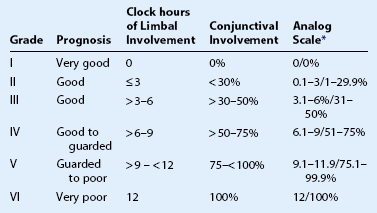
29 Chemical or thermal injury to the eye constitutes an ophthalmic emergency, due to the potential for permanent visual impairment and the threat to the structural integrity of the eye. The prognosis for severe injury is typically poor and may result in widespread damage to the ocular surface epithelium, cornea and anterior segment.2 However, in recent years, the prognosis of severe ocular burns has improved, with advances in the understanding of the physiology of the cornea and the resultant development of enhanced medical and surgical treatments. The final visual prognosis is influenced by the nature of the chemical insult, the extent of ocular damage, and the timing and efficacy of treatment. Chemical or thermal burns represent 7.7% to 18% of cases of ocular trauma.1,3 Responsible chemicals are numerous and include cleaning agents, fertilizers, refrigerants, cement, preservatives and fireworks.2 Alkali injuries occur more frequently than acid injuries, as a result of their more ubiquitous presence in household and industrial products.2 Ocular burns caused by detergents and thermal agents are less common.2,4,5 Fortunately, the majority of chemical injuries are classified as mild2,5,6 and the estimated incidence of severe chemical injuries in the United Kingdom is approximately 0.02 per 100 000. Injured parties are characteristically young and male5–8 and exposure most commonly occurs in a variety of agricultural, industrial and domestic settings, or less commonly in association with a criminal assault.2,5,8 Unfortunately, studies report an increasing number of patients presenting with chemical eye injuries resulting from assault.6 Etiology of Chemical Injury: Causative Agents More than 25,000 chemical products with the potential to cause chemical eye injuries have been identified, many of which may be classified as acids or bases, oxidizing or reducing agents, or corrosives. The most frequently implicated chemical agents are acids and bases. The severity of the injury is related to the nature, concentration, quantity and pH of the chemical involved, and the duration and surface area of exposure.3 In particular, a history of a high-velocity (explosive) chemical or thermal injury should always raise suspicion of an associated intraocular foreign body. Wet and dry cement, ammonia, lye, potassium hydroxide, magnesium hydroxide, and lime, constitute the most common causes of alkali injury to the eye.2,5,8 The severity of an alkali injury is governed by the pH, rather than the properties of the cation.2 Therefore, the most severe injuries are typically caused by ammonia and lye8 which are both capable of rapid penetration into the eye. The damage inflicted by lime injuries is reduced by the formation of calcium soaps that precipitate and hinder further penetration.2 Firework injuries deserve special mention as the presence of magnesium hydroxide results in a combined chemical and thermal injury. The most important agents causing alkali and acid injuries to the eye are summarized in Table 29.1. Table 29.1 Common Causes of Alkali and Acid Injuries2 (Adapted from Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and therapy. Surv Ophthalmol 1997;41:275–313.) The most common causes of acid burns are sulphuric, sulphurous, hydrofluoric, acetic, chromic, and hydrochloric acids.2 The strength of an acid depends on its ability to lose a proton; strong acids ionize completely in an aqueous solution. However, the most severe acid injuries are caused by hydrofluoric acid, as a result of its unique properties. In addition to the action of the dissociated proton, which is the primary mechanism of damage by other acids, hydrofluoric acid has a unique dissolving action which allows it to quickly penetrate into deeper tissues.2 Moreover, hydrofluoric acid chelates all calcium and magnesium from cells, thereby halting cellular biochemical activity. Although alkalis typically cause the most serious chemical injuries, the presence of an acid injury does not preclude an equally devastating ocular injury as very strong acids penetrate just as rapidly as alkalis. Indeed, studies have shown no clinically significant differences in clinical course and prognosis between severe acid and alkali burns.9 Structural and Biochemical Alterations The severity of an ocular chemical injury is influenced by the ability of the chemical to penetrate the eye. Alkalis characteristically penetrate the eye more rapidly than acids.2,3,10 The hydroxyl ion (OH) saponifies plasma membranes, resulting in cell disruption and death, while the cation is responsible for the penetration of the specific alkali.2,3,10 Stronger alkalis are associated with more rapid penetration and the penetration rate increases in ascending order from calcium hydroxide, potassium hydroxide, sodium hydroxide to ammonium hydroxide.10 Changes in aqueous humor pH are observed within a few seconds of contact with ammonium hydroxide, and within 3–5 minutes after sodium hydroxide injury.10,11 Ultimately, irreversible tissue damage occurs when the pH rises above 11.5.2,10 In alkali injuries, cations react with the carboxyl (COOH) groups of stromal collagen and glycosaminoglycans.2,10 Hydration of glycosaminoglycans results in loss of clarity of the stroma, whereas, hydration of collagen fibrils causes distortion of the trabecular meshwork and the release of prostaglandins, these sequelae combine to produce elevations in intraocular pressure.10 In general, as previously noted, acids penetrate the corneal stroma much less readily than alkalis.2,3,10,12 The hydrogen ion mediates damage due to pH alteration, while the anion causes precipitation and denaturation of proteins in the corneal epithelium and anterior stroma.10 Precipitation of the epithelial proteins affords a degree of protection by providing a physical barrier against further ingress.2,3,10,12 However, in the event that an acid succeeds in penetrating the stroma, the damage to ocular structures is similar to that observed in alkali injury.2 Alterations include precipitation of extracellular glycosaminoglycans and corneal opacification, distortion of the trabecular meshwork, changes in anterior chamber pH, damage to anterior chamber structures, and reduced aqueous ascorbate levels.2,10 Vascular damage results in ischemic injury. Both acids and bases may mediate osmolar damage to the delicate physiology of the cornea.2 Chemical insults to the eye may initiate large changes in osmolarity, and the resultant osmolar stress gives rise to cellular dysfunction and destruction. The limited buffering capacity of the cornea affords little protection against a variety of chemical and toxic insults. In the event that the buffering capacity is overwhelmed, there is an immediate cessation of biochemical activity, such as protein synthesis.13 Following corneal epithelial injury, recovery is dependent on the centripetal migration of cells from the most proximal region of viable epithelium.14 The extent of the injury dictates the source of regenerating epithelium; epithelial defects involving a portion, or the entirety of the cornea are replenished by adjacent corneal epithelium and limbus, respectively. However, in the event of complete corneal and limbal epithelial loss, the conjunctiva is the only source of regenerating epithelium. The source of regenerating epithelium influences the rate of re-epithelialisation and the ultimate phenotype of the restored epithelium.2 A variety of factors may retard the rate of re-epithelisation following chemical injury, including a robust and persistent inflammatory response, and structural damage to the epithelial basement membrane.2 Non-healing corneal epithelial wounds pose a significant risk as they expose the cornea to potential microbial infection. Severe chemical injuries deplete stromal keratocyte populations, and initiate collagenolytic processes which degrade collagen fibrils.2 These processes undermine the structural integrity of the corneal stroma, and may culminate in corneal ulceration and perforation. Keratocytes play a critical role in the maintenance and regeneration of the corneal stroma. Following corneal injury, keratocytes migrate into areas of damaged stroma from adjacent tissue. Keratocytes are responsible for collagen synthesis, and collagen production is maximal between days 7 and 56, with a peak at day 21 post injury.2 Collagen synthesis requires ascorbate and thus, may be significantly impaired by the scorbutic state induced in the cornea following severe chemical injury.15,16 Severe chemical injuries are characterized by two waves of inflammation; the first wave occurs in the first 24 hours and the second wave begins at approximately 7 days and peaks 2 to 3 weeks post injury. The intensity of the first wave may be critical for the recruitment of the second wave.2 The second wave of inflammation coincides with the period of maximal corneal degradation and repair, and may facilitate the sterile enzymatic digestion of the corneal stroma. Sterile ulceration is associated with the infiltration of polymorphonuclear leukocytes, and conversely, the exclusion of inflammatory cells from the corneal stroma is associated with cessation of sterile ulceration.2 Emergency management is oriented towards prompt irrigation and the removal of residual chemical debris from the eye. The objectives are to minimize the ingress of the chemical agent into the anterior chamber, and to remove a potential reservoir for ongoing injury. The most important intervention is immediate copious irrigation at the scene of the incident.17,18 Irrigation should be continued until pH neutralization is achieved. Animal models have demonstrated that external irrigation for 90 minutes reduces the pH by 1.5 units.11 In a non-controlled human study involving 66 eyes, immediate copious irrigation resulted in less severe injury, compared with eyes which were not irrigated.17 Although there may be an advantage in the use of amphoteric buffering solutions,10 urgency may necessitate the use of any available neutral irrigation fluid. External irrigation is of limited value in eliminating chemicals once they have reached the intraocular chambers. Animal models of alkali injuries have shown that paracentesis lowers the aqueous humor pH by 1.5 pH units. Subsequent anterior chamber reformation, with buffered phosphate solution, lowers the aqueous humor pH by a further 1.5 pH units.11 However, the value of paracentesis and irrigation of the anterior chamber following a severe chemical injury remains controversial.2 Nonetheless, it may be reasonable to consider aqueous humor replacement in patients with severe injuries presenting within the first 2 hours post exposure. Classification schemes for grading the severity of the initial injury are useful in guiding treatment and provide an estimation of prognosis. The Roper–Hall classification system19 (Table 29.3) was introduced in the mid-1960s and is the most established and commonly applied system. It provides prognostic guidelines based on the degree of corneal haze and the amount of perilimbal ischemia. However, the years following the introduction of the Roper–Hall classifications have seen changes in the understanding and management of ocular surface burns. An enhanced understanding of the role of the limbus in wound healing has been of particular importance. In order to reflect these changes, Dua proposed a new classification scheme in 2001 (Table 29.4) based upon clock hours of limbal involvement (as opposed to ischemia), as well as the percentage of conjunctival involvement. In a recent study, Gupta et al.20 concluded that the Dua classification had superior prognostic value over the Roper–Hall classification scheme in the context of severe ocular burns. Table 29.3 Roper–Hall Classification 196519 (From Roper-Hall MJ. Thermal and chemical burns. Trans Ophthalmol Soc UK 1965;85:631–53.) Table 29.4 *The analog scale records accurately the limbal involvement in clock hours of affected limbus/percentage of conjunctival involvement. While calculating percentage of conjunctival involvement, only involvement of bulbar conjunctiva, up to and including the conjunctival fornices is considered. (From Dua HS, King AJ, Joseph A. A new classification of ocular surface burns. Br J Ophthalmol 2001;85:1379–83.) Examples of mild, moderate and severe chemical burns are highlighted in Figures 29.2, 29.3, and 29.4, respectively.
Chemical and Thermal Injuries to the Ocular Surface
Introduction
Epidemiology
Ocular Chemical Injury
Alkalis
Acids
Pathophysiology
Injury, Repair and Differentiation
Ocular Surface
Stroma
Inflammation
Emergency Treatment
Aqueous Humor Replacement
Classification
Chemical and Thermal Injuries to the Ocular Surface