Otitis media is now the most common disease diagnosed by clinicians in the United States. Even though these infections primarily affect infants and young children and to a lesser extent, older children and teenagers, the disease is also common in adults. Over the past two decades, there has been a significant increase in the incidence of otitis media in children, especially in the infant age group, which has been attributed to the dramatic rise in attendance in child day care centers.1
Currently, there are at least four major controversies related to the management of this highly prevalent disease: (1) to treat or not to treat acute otitis media with antibiotics; (2) to treat or not to treat middle ear effusion that persists after an episode of acute otitis media with antibiotics; (3) to treat or not to treat otitis media with effusion with antibiotics; and (4) which management options are most safe and effective for prevention of recurrent acute otitis media. These controversial issues are primarily due to the ever-increasing rates of antibiotic-resistant bacterial pathogens that cause otitis media, which has been attributed to overuse of antimicrobial agents.
Diagnosis of Otitis Media Related to Treatment
Important in the decision to treat or not treat otitis media, the clinician must appreciate the diagnostic differences between acute otitis media and otitis media with effusion, as the latter condition is usually not treated unless it becomes chronic (Table 78—1).
Acute otitis media is characterized by the rapid, brief onset of signs and symptoms of infection in the middle ear. One or more of the following are present: otalgia (or pulling of the ear in the infant), fever, or irritability of recent onset. The tympanic membrane is full or bulging, opaque, and has limited or no mobility to pneumatic otoscopy. After an episode of acute otitis media, the middle ear may have fluid that remains for weeks to months, which has been termed persistent middle ear effusion.
* Maria B. Bluestone provided editorial assistance in the preparation of this manuscript.
Otitis media with effusion is a relatively asymptomatic middle ear effusion. Pneumatic otoscopy frequently shows either a retracted or concave tympanic membrane, the mobility of which is limited or absent. However, fullness, or even bulging, may be visualized. In addition, an air-fluid level or bubbles, or both, may be observed through a translucent tympanic membrane.
Microbiologic Etiology Related to Treatment
Related to an accurate diagnosis, there is a difference in the prevalence of bacterial pathogens that are isolated from ears of patients with acute otitis media compared to aspirates of otitis media with effusion. This, in turn, has an impact on the decision to recommend or not recommend antimicrobial therapy.
Pathogenic bacteria are present in approximately 70% of the middle ears of patients who have acute otitis media, and are similar in type in both children and adults.2, 3 Streptococcus pneumoniae (40%), Haemophilus influenzae (25%), and Moraxella catarrhalis (12%) are the most common pathogens isolated. Group A β-hemolytic streptococcus and Staphylococcus aureus also cause this infection in both children and adults, but not as frequently as pneumococcus and H. influenzae. Respiratory viruses have been cultured from as many as 20% of acute effusions.
The percentage of H. influenzae that is β-lactamase-producing varies according to the community in the United States, but the rate is now about 25%. Currently, most, if not all strains of M. catarrhalis produce β-lactamase. The rate of isolation of multidrug-resistant S. pneumoniae is increasing in this country. At the Children’s Hospital of Pittsburgh—a tertiary referral center—the rate increased from approximately 10% in 1988 to more than 40% in 1997, and more than one-half of these strains were highly resistant; most likely the rate is lower in community practices (Fig. 78—1).
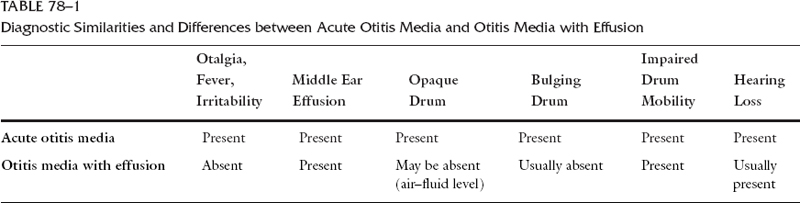
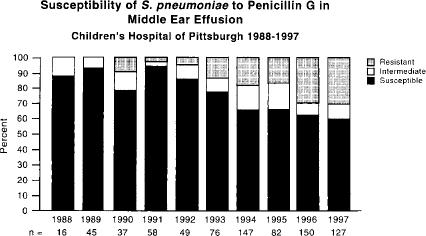
Figure 78—1 Prevalence of penicillin-resistant Pneumococcus isolated from the middle ears of infants and children at the Children—s Hospital of Pittsburgh from 1988 to 1997.
In contrast to acute otitis media, bacteria considered to be potentially pathogenic can be isolated from only one-third of middle-ear aspirates from patients who have otitis media with effusion. Similar to isolates from acute otitis media, the most common are S. pneumoniae, H. influenzae, and M. catarrhalis , but the latter two organisms are more commonly isolated than pneumococcus.4 Resistance rates of these organisms are similar to rates found when these bacteria cause acute otitis media. Recently, these three bacteria have been detected by polymerase chain reaction (PCR) in approximately 70% of chronic middle ear effusions at the time of myringotomy and tympanostomy tube insertion; only about one-third of the organisms were identified using traditional culture methods.5, 6
Management
ACUTE OTITIS MEDIA
Antibiotic therapy has been the standard treatment for acute otitis media for over half a century, but this widespread practice has now been questioned.
To Treat or Not to Treat Acute Otitis Media with Antibiotics?
With the possibility of increasing the problem of resistant bacterial pathogens, some clinicians, especially in some European countries, question the need for antimicrobial therapy in all patients for treatment of acute otitis media. But most experts in the United States today agree that acute otitis media should be actively treated with an antimicrobial agent. Table 78—2 summarizes four outcomes that provide convincing evidence to support this recommendation and are described in detail below.
| Compared with placebo (or no drug), antimicrobials: |
| 1. Sterilize the middle ear effusion7 2. Result in earlier resolution of symptoms of acute infection8 3. Shorten time with middle ear effusion (hearing loss)9 4. Dramatically decrease suppurative complications10, 11 |
Microbiologic Outcome Howie et al.7 evaluated the microbiologic efficacy with various therapeutic regimens, including a placebo. Although these studies suggest that many cases of infection of the middle ear resolve spontaneously or with the assistance of spontaneous drainage, the data indicate that the most important bacterial pathogens responsible for otitis media will not resolve clinically or microbiologically without medical intervention. A proportion of middle ear effusions that have a positive culture clear the organism without drug intervention (spontaneous clearance). However, in about 20% of infections due to S. pneumoniae , and in 50% of infections due to H. influenzae , administration of an antimicrobial agent to which these organisms are susceptible results in sterilization of the effusion in almost all the ears.
Symptomatic Outcome Rosenfeld et al.8 conducted a meta-analysis of 5400 children from 33 randomized trials that addressed the question of efficacy of antimicrobial therapy. These investigators found the spontaneous (without antibiotics or tympanocentesis) rate of primary control to be 81%. However, the rate was 95% when antimicrobial agents were administered. They concluded that “antibiotics have a modest but significant impact on the primary control of acute otitis media.”
Middle Ear Effusion Outcome Kaleida and colleagues9 evaluated amoxicillin or placebo for management of nonsevere acute otitis media. (The distinction between severe and nonsevere disease was based on an otalgia scoring system and the child’s temperature; subjects in the severe category were not randomized to receive only placebo.) At the completion of the 2-week amoxicillin treatment, there were statistically fewer children with middle ear effusion (47%) when compared to those who received placebo (63%). Since presence of middle ear effusion is associated with a conductive hearing loss, the administration of an antimicrobial agent reduces the time with hearing loss, which may have implications for child development.
Suppurative Complications Outcome Two important, large clinical trials conducted in Scandinavia during the 1950s, in which patients either were treated with an antibiotic or the agents were withheld, demonstrated that the suppurative complications of otitis media, such as mastoiditis and meningitis, almost exclusively occurred in those children who did not receive antimicrobial agents.10, 11 The rate of suppurative complications of acute otitis media has dramatically fallen with the advent of the widespread use of antimicrobial agents for this infection. Withholding antimicrobial therapy today will most likely result in an increase in complications.
Indeed, the Centers for Disease Control and Prevention and the American Academy of Pediatrics have recently reaf-firmed the recommendation to treat all documented cases of acute otitis media with an antimicrobial agent, but stressed the need to make a distinction between acute otitis media and otitis media with effusion, as the latter disease does necessarily require medical treatment.12
Selection of an Antimicrobial Agent
Of the 15 antimicrobial agents currently approved for treatment of acute otitis media, amoxicillin is still recommended for initial empiric therapy, as it is relatively safe, effective for most strains of S. pneumoniae and H. influenzae, and available in a variety of formulations (Table 78—3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


