Purpose
We sought to analyze surgically induced refractive change (SIRC) and change in high-order aberration after Raindrop corneal inlay insertion (ReVision Optics, Lake Forest, CA), and assess the extent to which Raindrop corneal inlay insertion could correct presbyopia.
Design
Interventional case series.
Methods
Seventeen patients were included if they had a corneal thickness ≥500 μm and a stable manifest spherical equivalent refraction between 0.50 and +1.00 diopters (D). The Raindrop corneal inlay was implanted on the stromal bed of a femtosecond laser-assisted generated flap of nondominant eyes. Manifest refraction, corneal powers, and corneal high-order aberrations were measured preoperatively and at 3 and 12 months postoperatively.
Results
The SIRC by manifest refraction was 0.99 ± 0.26 D. The changes derived from simulated keratometry (K), true net power, and equivalent K reading (EKR) at 1.0–4.0 mm were greater than the SIRC (all P < .01) while the change in EKR at 6.0 mm was less than the SIRC ( P < .01). The changes in EKR 5.0 mm, automated K, and EKR 4.5 mm did not differ significantly from the SIRC ( P = .81, .29, and .09, respectively), and the difference was the least for EKR 5.0 mm. In analysis of high-order aberrations, only spherical aberration showed statistically significant difference between preoperative and postoperative on both anterior cornea and total cornea (all P < .01).
Conclusion
Raindrop corneal inlay corrects presbyopia via increasing negative spherical aberration. The equivalent K reading at 5.0 mm accurately reflected the SIRC, and would be applicable for intraocular power prediction before cataract surgery.
Presbyopia is an age-related process involving loss of accommodation, such that the eye is no longer capable of comfortably sustaining the accommodation necessary for clear near vision. The nearest point that can be focused on gradually recedes, leading to a need for spectacles for near work, such as reading, and even for focusing at intermediate distances.
The dioptric elements of the eye are the cornea and the crystalline lens. In contrast with the latter, the cornea is a stable optical structure, and it can therefore be used to therapeutically induce precise and useful amounts of pseudoaccommodation via the creation of a multifocal optical profile.
The treatment of presbyopia in emmetropic patients is currently one of the biggest challenges in refractive surgery, and several different approaches have been used, including conductive keratoplasty, laser-assisted in situ keratomileusis (LASIK) monovision, corneal multifocal ablation, intrastromal femtosecond concentric rings, and corneal inlays.
Corneal inlays were originally developed by Barraquer in the 1940s as a treatment for ametropia, and were continuously improved over subsequent years. Currently, corneal inlays are a potentially successful treatment option for presbyopia rather than ametropia. They are usually implanted on the corneal stroma, under a corneal flap, or within a corneal pocket in the nondominant eye. They are small, 2–4 mm in diameter, and 5–40 μm thick. They involve implanting a higher refractive index material deep in the cornea or limiting the pupil entrance diameter via a pinhole design. They can also be used in conjunction with myopic or hyperopic LASIK surgery.
In recent studies, Raindrop corneal inlay (ReVision Optics, Lake Forest, CA) improved uncorrected near and intermediate visual acuity, with high patient satisfaction. The aim of this current study was to analyze surgically induced refractive change (SIRC) and change in high-order aberration (HOA) after Raindrop corneal inlay insertion, and assess the extent to which Raindrop corneal inlay insertion could correct presbyopia.
Methods
Informed consent was obtained from all patients before the study, and the methods used adhered to the tenets of the Declaration of Helsinki for the use of human participants in biomedical research. This study was approved by the institutional review board of Seoul St. Mary’s Hospital.
Patients were included if they needed a near add between +1.50 and +2.50 D and had a stable manifest spherical equivalent refraction between −0.50 and +1.00 D with no more than 1.00 D of refractive cylinder, and had best-corrected distance and near visual acuities of 0.1 logMAR (20/25 Snellen) or better. A monovision trial was performed, and patients were implanted after expressing satisfaction with their vision and confidence that they could conduct their lives normally after wearing a contact lens to correct the near vision of the nondominant eye for at least 5 days. The Early Treatment Diabetic Retinopathy Study near (40 cm), intermediate (80 cm), and distance (6 m) visual acuities were assessed using the Optec 6500 Vision Tester (Stereo Optical Co., Inc., Chicago, IL) set to photopic luminance. Uncorrected near visual acuity, uncorrected intermediate visual acuity, and uncorrected distance visual acuity were measured preoperatively and at 3 and 12 months postoperatively. The treated eye had a corneal thickness ≥500 μm. Exclusion criteria included previous ocular surgery; ocular or eyelid pathology, infection, or inflammation; irregularity in corneal topography; systemic disease or therapies that could affect wound healing or visual outcomes; and any condition that could lead to refractive changes.
Refractive outcomes were measured at 3 and 12 months postoperatively by manifest refraction, and keratometric measurements were obtained 3 and 12 months after the operation using a Canon RK-5 automated keratometer and a Pentacam rotating Scheimpflug camera. A Pentacam HR (Oculus, Wetzler, Germany) was used to analyze the cornea via 25-picture scanning, and only scans that had an examination quality specification graded by the instrument as “OK” were included in this study. Preoperatively and postoperatively, the following corneal measurements were analyzed using a Pentacam Scheimpflug rotating camera.
Average keratometry (K) reading. This value is the arithmetic mean of the pair of meridians 90° apart with the greatest difference in axial power within the central 3.0 mm. It is equivalent to the simulated K of traditional corneal topography, and is calculated by entering a corneal curvature radius into a thin-lens formula for paraxial imagery, which considers the cornea as a single refractive sphere.
True net power . This is the result of a modified Gaussian optics formula for thick lenses.
Equivalent K reading . This value is calculated via the formula previously described by Holladay et al., and takes into account the effect of the posterior corneal surface.
Corneal HOAs . The elevation data from Scheimpflug images are combined to form a 3-dimensional reconstruction of the corneal structure. Internal software automatically converts the corneal elevation profile into corneal wavefront data using Zernicke polynomials. HOAs were measured on anterior cornea, posterior cornea, and total cornea in the 6.0 mm zone.
Corneal Inlays
Raindrop corneal inlays are made of a clear, permeable hydrogel material with approximately the same refractive index as the cornea (1.376). They have a positive meniscus shape, with a diameter of 2 mm and a central thickness of 32–36 μm. The index of refraction is the same as that of the surrounding corneal tissue; it alters the eye’s refractive power only by increasing the central radius of curvature of the cornea overlying the implant. Because the inlay is thinner at the edge than in the center, the increase in anterior corneal height transitions from the region to the inlay diameter, through an intermediate region, and back to the unaltered cornea. The final anterior corneal shape is influenced by the biomechanical remodeling of the overlying anterior flap, and remodeling of epithelium.
Surgical Procedure
The nondominant eye was prepared for creating a flap with a diameter >8 mm, and a depth of one-third of the central corneal thickness (IntraLase; Abbott Medical Optics, Inc., Santa Ana, CA). The Raindrop corneal inlay was delivered from the preloaded inserter to the stromal bed. The inlay was positioned over the center of the pupil and the flap was replaced on the corneal bed.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 21.0; SPSS, Inc., Chicago, IL). The Wilcoxon signed-rank test was used to assess the significance of the differences between the preoperative and postoperative data. The Friedman test (nonparametric repeated measures analysis of variance) was also performed with the Dunn posttest in analysis of corneal power changes, and P < .01 was determined to indicate statistical significance.
Results
Table 1 shows the patient characteristics and preoperative data. There were 7 right eyes and 10 left eyes in this study, and the preoperative subjective spherical equivalent was 0.45 ± 0.71 D. For accurate analysis of HOA, some Zernike coefficients for those HOA modes with odd symmetry—specifically Z(3,3) (trefoil-x), Z(3,1) (coma-x), Z(4,−2) (secondary astigmatism), and Z(4,−4) (Q) of the 7 right eyes—were converted to have opposite sign as recommended by the Optical Society of America notation for Zernike polynomials. Figure 1 shows the mean monocular visual acuities for a period of time in eyes with a corneal inlay. Both at 3 and 12 months postoperatively, uncorrected near visual acuity was improved compared with preoperative examination (0.60 ± 0.17 vs 0.10 ± 0.14 and 0.11 ± 0.11, all P values < .01). Eyes with corneal inlay showed a significantly improved uncorrected intermediate visual acuity at 3 and 12 months postoperatively (0.31 ± 0.12 vs 0.06 ± 0.10 and 0.06 ± 0.09, all P values < .01). On the other hand, there was no statistically significant difference in uncorrected distance visual acuity (0.04 ± 0.06 vs 0.09 ± 0.07 and 0.08 ± 0.06, P values .19 and .26, respectively).
| Variable | Value |
|---|---|
| Age (y) | |
| Mean ± SD (range) | 54.64 ± 3.98 (48–60) |
| Sex | |
| Male:female | 9:8 |
| Number of eyes | 17 |
| Right:left | 7:10 |
| Preoperative data | |
| Manifest sphere (D) | 0.58 ± 0.62 |
| Manifest cylinder (D) | −0.28 ± 0.32 |
| Manifest SE (D) | 0.45 ± 0.71 |
| Uncorrected visual acuity | |
| Near | 0.60 ± 0.17 |
| Intermediate | 0.31 ± 0.12 |
| Distance | 0.04 ± 0.06 |
| Corrected visual acuity | |
| Near | 0.01 ± 0.10 |
| Intermediate | 0.01 ± 0.08 |
| Distance | 0.02 ± 0.07 |
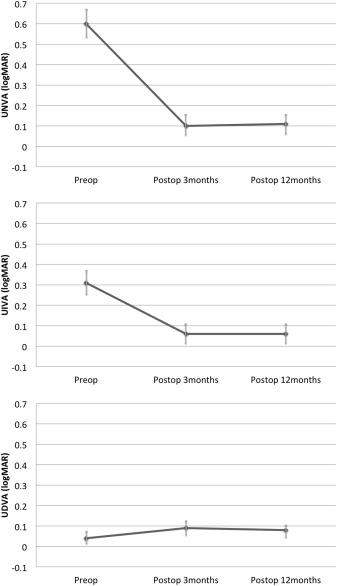
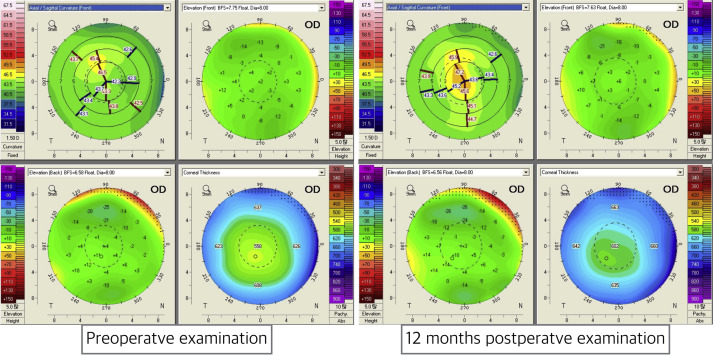
Figure 2 shows an example of one patient’s preoperative and 12-month postoperative data using a Scheimpflug rotating camera. The sagittal map shows the steepening of central cornea. In anterior surface best fit sphere map and posterior surface best fit sphere map, relatively greater change of best fit sphere was identified (0.12 vs 0.02).
The changes in subjective refraction and keratometric values are shown in Table 2 . The mean manifest refractive changes in the spherical equivalent at the corneal plane were 1.03 ± 0.27 D and 0.99 ± 0.26 D at 3 and 12 months postoperatively. The changes derived from simulated K, true net power, and equivalent K readings at 1.0–4.0 mm were greater than the SIRC (all P < .01). The difference was greatest equivalent K reading at 1.0 mm, followed by equivalent K reading at 2.0 mm, equivalent K reading at 3.0 mm, true net power, equivalent K reading at 4.0 mm, and simulated K. The change in equivalent K reading at 6.0 mm was less than the SIRC ( P < .01). The changes in equivalent K reading at 5.0 mm, automated K, and equivalent K reading at 4.5 mm did not differ significantly from the SIRC ( P = .74, .24, and .07 at 3 months postoperatively and P = .81, .29, and .09 at 12 months postoperatively), and the difference was the least for equivalent K reading at 5.0 mm.
| Parameter | 3 Months Postoperatively – Preoperatively | 12 Months Postoperatively – Preoperatively | ||
|---|---|---|---|---|
| P Value With SIRC a | P Value With SIRC a | |||
| Subjective refraction | 1.03 ± 0.27 | 0.99 ± 0.26 | ||
| Automated keratometer | 1.14 ± 0.32 | .24 | 1.13 ± 0.31 | .29 |
| Simulated K | 1.32 ± 0.30 | <.01 | 1.72 ± 0.28 | <.01 |
| True net power | 1.61 ± 0.35 | <.01 | 1.57 ± 0.35 | <.01 |
| Equivalent K reading at 1.0 mm | 3.40 ± 0.65 | <.01 | 3.31 ± 0.60 | <.01 |
| Equivalent K reading at 2.0 mm | 2.87 ± 0.49 | <.01 | 2.83 ± 0.47 | <.01 |
| Equivalent K reading at 3.0 mm | 2.18 ± 0.37 | <.01 | 2.14 ± 0.38 | <.01 |
| Equivalent K reading at 4.0 mm | 1.52 ± 0.28 | <.01 | 1.52 ± 0.27 | <.01 |
| Equivalent K reading at 4.5 mm | 1.22 ± 0.27 | .07 | 1.20 ± 0.23 | .09 |
| Equivalent K reading at 5.0 mm | 1.01 ± 0.24 | .74 | 0.99 ± 0.23 | .81 |
| Equivalent K reading at 6.0 mm | 0.74 ± 0.26 | <.01 | 0.74 ± 0.25 | <.01 |
a The Friedman test (nonparametric repeated measures analysis of variance) was performed with the Dunn posttest.
Table 3 shows the HOAs of the anterior cornea. Only spherical aberration showed a statistically significant difference between preoperative and postoperative anterior cornea values ( P < .01). The mean changes in spherical aberration were −0.43 ± 0.19 μm at 3 months postoperatively and −0.41 ± 0.17 at 12 months postoperatively. Specifically, negative spherical aberrations increased after Raindrop corneal inlay implantation. Table 4 shows the HOAs of the posterior cornea, none of which changed significantly ( P = .09–.86). Table 5 shows the HOAs of the total cornea, of which only spherical aberration exhibited a statistically significant difference between preoperative and postoperative anterior cornea ( P < .01). The mean change in spherical aberration was −0.43 ± 0.13 μm at 3 months postoperatively and −0.40 ± 0.13 μm at 12 months postoperatively, and negative spherical aberrations increased. Figure 3 shows the changes in HOAs for 3 months after corneal inlay implantation.
| Zernike Coefficient | Preoperatively | 3 Months Postoperatively | P Value a | 12 Months Postoperatively | P Value b |
|---|---|---|---|---|---|
| Z(3,3) (trefoil-x) | −0.01 ± 0.12 | −0.08 ± 0.13 | .16 | −0.05 ± 0.13 | .45 |
| Z(3,1) (coma-x) | 0.16 ± 0.10 | 0.17 ± 0.10 | .91 | 0.17 ± 0.10 | .90 |
| Z(3,−1) (coma-y) | 0.12 ± 0.27 | 0.18 ± 0.34 | .42 | 0.16 ± 0.30 | .67 |
| Z(3,−3) (trefoil-y) | −0.06 ± 0.18 | −0.06 ± 0.21 | .92 | −0.06 ± 0.20 | .90 |
| Z(4,4) (Q) | −0.05 ± 0.08 | −0.01 ± 0.13 | .31 | −0.01 ± 0.11 | .33 |
| Z(4,2) (2nd astigmatism) | 0.06 ± 0.05 | 0.05 ± 0.10 | .86 | 0.05 ± 0.08 | .87 |
| Z(4,0) (SA) | 0.29 ± 0.11 | −0.14 ± 0.18 | <.01 | −0.13 ± 0.17 | <.01 |
| Z(4,−2) (2nd astigmatism) | 0.01 ± 0.04 | 0.01 ± 0.08 | .91 | 0.01 ± 0.05 | .92 |
| Z(4,−4) (Q) | −0.02 ± 0.09 | −0.06 ± 0.15 | .36 | −0.05 ± 0.11 | .44 |
| Total HOAs | 0.54 ± 0.11 | 0.63 ± 0.12 | .05 | 0.61 ± 0.11 | .11 |
a Wilcoxon signed-rank test for comparison of preoperative and postoperative data at 3 months.
b Wilcoxon signed-rank test for comparison of preoperative and postoperative data at 12 months.
| Zernike Coefficient | Preoperatively | 3 Months Postoperatively | P Value a | 12 Months Postoperatively | P Value b |
|---|---|---|---|---|---|
| Z(3,3) (trefoil-x) | −0.01 ± 0.02 | −0.01 ± 0.05 | .82 | −0.01 ± 0.04 | .86 |
| Z(3,1) (coma-x) | −0.02 ± 0.02 | −0.03 ± 0.02 | .73 | −0.01 ± 0.02 | .80 |
| Z(3,−1) (coma-y) | 0.00 ± 0.05 | 0.02 ± 0.05 | .02 | 0.01 ± 0.05 | .10 |
| Z(3,−3) (trefoil-y) | 0.00 ± 0.06 | −0.02 ± 0.04 | .13 | −0.01 ± 0.04 | .17 |
| Z(4,4) (Q) | −0.04 ± 0.02 | −0.03 ± 0.02 | .09 | −0.03 ± 0.02 | .10 |
| Z(4,2) (2nd astigmatism) | −0.03 ± 0.02 | −0.03 ± 0.02 | .69 | −0.03 ± 0.02 | .68 |
| Z(4,0) (SA) | −0.14 ± 0.03 | −0.15 ± 0.03 | .19 | −0.14 ± 0.03 | .17 |
| Z(4,−2) (2nd astigmatism) | 0.00 ± 0.01 | −0.01 ± 0.02 | .57 | 0.00 ± 0.02 | .57 |
| Z(4,−4) (Q) | 0.00 ± 0.01 | 0.02 ± 0.02 | .20 | 0.01 ± 0.02 | .27 |
| Total HOAs | 0.18 ± 0.03 | 0.20 ± 0.03 | .12 | 0.19 ± 0.03 | .18 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


