Fig. 1
Eight-year-old male h/o pyriform aperture stenosis with an associated solitary central median maxillary incisor
Mild cases of PAS may be treated conservatively with humidification and topical nasal decongestants. Severe cases require surgical management, which is most frequently approached via a sublabial incision in infants. The aperture is widened using drills, shavers, and/or bony curettes. Occasionally, a portion of the anterior head of the inferior turbinate is removed to improve the airway. Stenting may be recommended for a period of 1–4 weeks.
Nasolacrimal Duct Cyst
Obstruction of the nasolacrimal duct is common, occurring in approximately 30 % of infants. Although most cases are asymptomatic, severe obstruction can occur resulting from the formation of cysts, which can herniate into the nasal cavity causing obstruction. Bilateral cysts form in 14 % of cases causing symptoms of respiratory distress prompting airway evaluation. Diagnosis is made with nasal endoscopy showing cystic masses in the inferior meati. CT can be used to aid in the diagnosis and may reveal dilation of the lacrimal duct and sac. Treatment of intranasal cysts involves an above-and-below approach with ophthalmologic probing of the duct and endonasal marsupialization of the cyst [6, 7].
Septal Deviation/Midnasal Stenosis
Septal deviation or dislocation of the cartilaginous septum can occur during traumatic delivery predisposing infants to severe nasal airway obstruction with nasal rhinitis. Diagnosis is made with anterior rhinoscopy revealing displacement of the septal cartilage into the obstructed side of the nose. Conservative treatment involves humidification, nasal steroids, and suctioning. If conservative treatment fails, manual reduction of the cartilaginous septum back into the septal groove of the maxillary crest can improve the nasal airway [8].
Choanal Atresia
The choanae connect the nasal cavity to the nasopharynx. When this connection fails to develop, choanal atresia (CA) results. CA is unilateral in 65–75 % of cases, typically causing only mild respiratory symptoms and chronic unilateral rhinorrhea. In bilateral CA, the nasal cavity is completely separated from the nasopharynx, resulting in more significant symptoms of cyanosis during feeding, respiratory distress, and failure to thrive. Bilateral CA is also associated with other congenital abnormalities, most notably CHARGE association, in approximately 50 % of patients. Nasal endoscopy shows a blind pouch with lack of connection between the nasal cavity and pharynx (Fig. 2). Axial CT confirms the diagnosis showing thickening of the posterior bony septum and medialization of the lateral nasal walls (Fig. 3) [9].
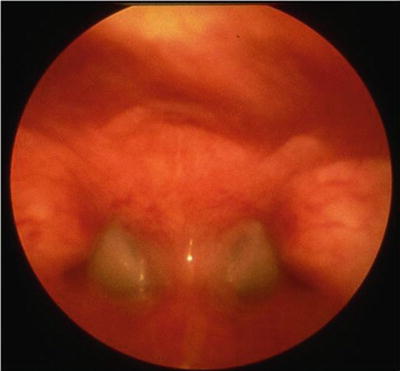
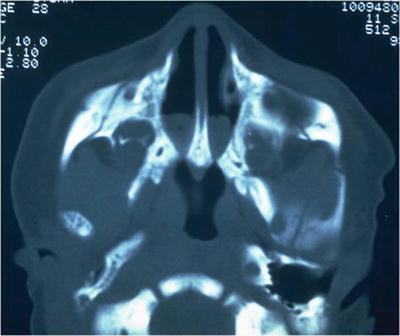
Fig. 2
Bilateral choanal atresia viewed from the oropharynx with a 120° scope
Fig. 3
Axial CT showing bilateral choanal atresia
Surgery is the primary treatment for CA. Timing varies dependent upon unilateral versus bilateral atresia with bilateral atresia needing attention in a more urgent fashion due to symptoms of respiratory distress. Multiple surgical options exist including transnasal puncture and/or dilation, transnasal approach with removal of bony stenosis with/without stenting, and transpalatal approach with/without stenting.
Oropharyngeal Obstruction
Newborns may present with obstruction at the level of the oral cavity and oropharynx. Obstruction at this level may cause respiratory distress immediately at birth, necessitating early airway intervention, including laryngoscopy to establish endotracheal intubation or tracheotomy.
Micrognathia/Base of Tongue Obstruction
Hypoplasia of the mandible, or micrognathia, with posterior displacement of the tongue base can cause significant obstruction of the oropharyngeal airway. Micrognathia can occur in isolation or in combination with several congenital craniofacial syndromes, most notably Pierre-Robin sequence (PRS) (Fig. 4). Characteristics of PRS include micrognathia, glossoptosis, or posterior displacement of the base of tongue, and cleft palate. Clinically, infants present with upper airway obstruction and feeding difficulties. Lack of weight gain despite adequate nutritional intake is an indicator of persistent airway obstruction. Severe airway obstruction is manifested by suprasternal and subcostal retractions, cyanosis, and carbon dioxide retention. Physical exam along with sleep endoscopy can confirm the diagnosis.

Fig. 4
Micrognathia in a child with Pierre-Robin sequence
Macroglossia
Tongue function is important for deglutition, phonation, and respiration. Macroglossia is defined as a resting tongue that protrudes beyond the teeth or alveolar ridge. Congenital macroglossia is seen in pediatric overgrowth disorders, most commonly Beckwith–Wiedemann syndrome. Low- and high-flow vascular anomalies with tongue involvement can also cause tongue enlargement. Clinically, severe macroglossia in the newborn can obstruct the oropharyngeal airway with symptoms of obstructive sleep apnea with CO2 retention, retractions, and respiratory distress. Surgical treatment options include tongue reduction surgery and/or tracheostomy [12, 13].
Congenital Pharyngeal Mass
Tumors obstructing the nasal/nasopharyngeal airway are exceedingly rare. Differential includes teratoma, epidermoid cyst, rhabdomyosarcoma, Rathke pouch cyst, lingual thyroid, vallecular cysts, and other rare neoplasms. Presenting signs include stridor with recurrent respiratory distress. CT and/or MRI are recommended to evaluate the extent of the lesion. Treatment involves securing the airway, occasionally with endoscopic assistance, and is subsequently dependent upon the primary etiology.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


