Cerebellopontine Angle Tumors
Joseph B. Nadol, Jr.
Robert L. Martuza
Because lesions of the cerebellopontine angle most commonly cause hearing loss and vestibular disturbance as their earliest symptoms, the otologist is often consulted for diagnosis and treatment. Although an acoustic neurinoma (vestibular schwannoma, acoustic neuroma, acoustic neurilemoma) is the most common lesion found in the cerebellopontine angle, the otologist should be aware that a variety of primary benign and metastatic malignant lesions may present in the cerebellopontine angle. Management of these lesions has undergone revolutionary change in the last decade. The introduction of diagnostic modalities, such as auditory evoked response audiometry and magnetic resonance imaging, allows demonstration of lesions at much earlier stages. Also, improvements in surgical technique have markedly reduced morbidity and mortality and have made preservation of hearing possible in resection of some of these lesions.
INCIDENCE OF SPECIFIC LESIONS OF THE CEREBELLOPONTINE ANGLE
Although acoustic neurinomas comprise between 75% and 90% of all tumors of the cerebellopontine angle, a variety of other primary and other metastatic lesions may mimic acoustic neurinomas clinically and radiographically. The most common lesions of the cerebellopontine angle and their approximate incidence are shown in Table 42.1. Approximately 98% of all lesions of the cerebellopontine angle are benign and 2% are malignant, either primary or metastatic. The clinical and diagnostic findings that will help differentiate these lesions preoperatively are discussed later (see Differential Diagnosis of Lesions of the Cerebellopontine Angle).
PRESENTING SIGNS AND SYMPTOMS OF CEREBELLOPONTINE ANGLE TUMORS
Unilateral progressive sensorineural loss with retrocochlear signs is the most common first symptom in tumors of the cerebellopontine angle. However, tumors may reach diameters of several centimeters without any substantial hearing loss. Although a down-sloping sensorineural pattern with poor discrimination is the most common audiometric pattern, low-frequency, midfrequency, fluctuating, and sudden sensorineural losses have also been described. Although the presenting symptoms may vary depending upon the origin and type of tumor, the most common presenting symptoms at initial diagnosis of cerebellopontine angle lesions are shown in Table 42.2. Given the fact that between 75% and 90% of all cerebellopontine angle lesions are acoustic neurinomas, the statistics in Table 42.2 are most descriptive of this lesion. More unusual lesions of the cerebellopontine angle may have a higher incidence of nonauditory and vestibular disturbances. For example, facial nerve schwannomas (Chapter 43) may present with slowly progressive facial nerve paresis as the initial neurologic deficit.
DIAGNOSTIC STRATEGY IN THE EVALUATION OF CEREBELLOPONTINE ANGLE LESIONS
The diagnosis of lesions of the cerebellopontine angle is based on neurotologic evaluation; audiometry, including auditory evoked response testing; vestibular testing; and radiographic imaging.
Neurotologic Evaluation
A complete neurotologic evaluation should include a history, particularly seeking the common symptoms presented in Table 42.2, such as auditory, vestibular dysfunction; headache; twitching or weakness of the facial muscles; and numbness of the face. A complete examination should include testing for facial hypesthesia to pin and light touch, evaluation of the corneal reflex using a wisp of cotton on the cornea, clinical evaluation of the facial nerve, cerebellar testing including rapid alternating movements, evaluation of gait disturbances, and testing of the function of the other cranial nerves (14,15).
Audiometry and Auditory Evoked Response Testing
Behavioral audiometry should include bilateral testing of pure-tone thresholds and evaluation of speech discrimination.
The most common audiometric pattern is a high-tone sensorineural loss, although flat loss, midfrequency loss, and low-frequency loss have been described (7). Although in most cases the hearing loss is slowly progressive, sudden or even fluctuant sensorineural loss may be seen. Decrement in speech discrimination tests is common, although there is little relationship between the size of the tumor and either pure-tone or discrimination results. Thus patients with intracanalicular lesions may present with profound sensorineural loss, whereas patients with lesions several centimeters in diameter in the cerebellopontine angle may have nearly normal hearing (Fig. 42.1).
The most common audiometric pattern is a high-tone sensorineural loss, although flat loss, midfrequency loss, and low-frequency loss have been described (7). Although in most cases the hearing loss is slowly progressive, sudden or even fluctuant sensorineural loss may be seen. Decrement in speech discrimination tests is common, although there is little relationship between the size of the tumor and either pure-tone or discrimination results. Thus patients with intracanalicular lesions may present with profound sensorineural loss, whereas patients with lesions several centimeters in diameter in the cerebellopontine angle may have nearly normal hearing (Fig. 42.1).
TABLE 42.1 Lesions of the cerebellopontine angle | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 42.2 Presenting symptoms in cerebellopontine angle lesions | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
The classical tests of retrocochlear involvement, such as tone decay, have been largely replaced by auditory evoked response testing. Brainstem evoked response audiometry is the single most reliable audiometric diagnostic procedure in the diagnosis of cerebellopontine angle lesions. Depending on the parameters used to analyze the evoked response testing, the false-positive and false-negative rates are consistently less than 10% (16).
Vestibular Testing
Approximately 50% of the patients complain of vestibular symptomatology, most commonly mild unsteadiness. However, vestibular hypofunction, as demonstrated by electronystagmography, is seen in most patients with cerebellopontine angle lesions. In a review of 500 patients for unilateral acoustic neurinomas, Brackmann (6) reported that vestibular hypofunction was found in 82%. Similarly, Ojemann et al. (8) reported that 96% of their patients demonstrated vestibular hypofunction by caloric testing. Positional nystagmus was present in approximately 80% of cases, and in more than half of these the positional nystagmus was of the persistent variety (types 1 and 2).
Radiographic Imaging
In no area of diagnostic evaluation has there been more dramatic change in the last decade than in radiographic imaging of the cerebellopontine angle. Laminograms of the internal auditory canal and Pantopaque cisternograms, common 10 years ago, have now been replaced with modern computed tomography (CT) and magnetic resonance imaging (MRI). CT scans with contrast enhancement can reliably image lesions in excess of 1 cm in diameter. MRI, particularly with the introduction of gadolinium contrast enhancement, has provided a reliable method for diagnosing acoustic neurinomas that are purely intracanalicular and provides a technique of low morbidity to evaluate tumor growth or monitor for postoperative recurrence (Fig. 42.2). Gadoliniumenhanced MRI is currently the most sensitive test to evaluate for a suspected cerebellopontine angle tumor and should be
performed in cases of unilateral hearing loss in which the etiology is unclear.
performed in cases of unilateral hearing loss in which the etiology is unclear.
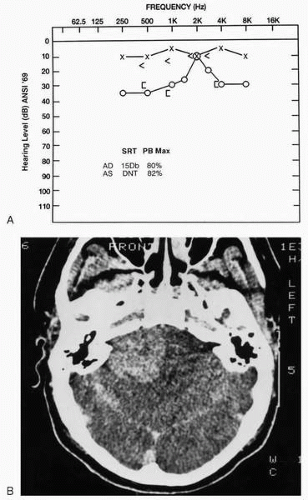 FIG. 42.1 A: Audiogram of a 26-year-old man whose only symptoms were slight hearing loss and tinnitus in the right ear. B: Computed tomographic (CT) scan of the patient demonstrating a 5-cm tumor of the right cerebellopontine angle, histologically demonstrated to be an acoustic neurinoma. |
DIFFERENTIAL DIAGNOSIS OF LESIONS OF THE CEREBELLOPONTINE ANGLE
Although between 75% and 90% of all lesions of the cerebellopontine angle are benign acoustic neurinomas, a variety of other lesions may be found in this location (Table 42.1). The results of the neurotologic and diagnostic evaluations may provide hints as to the presence of a lesion other than an acoustic neurinoma. Differential features of the most common lesions other than acoustic neurinomas are therefore presented.
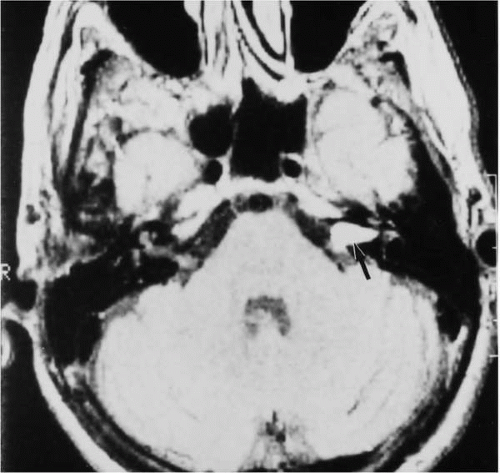 FIG. 42.2 MRI with gadolinium enhancement demonstrating an intracanalicular acoustic neurinoma on the left (arrow). This lesion was not visualized by CT or MRI without contrast enhancement. |
Meningiomas
The presenting symptoms of meningioma differ only slightly from those of acoustic neurinoma. Hearing loss seems to be less common and trigeminal symptomatology more common in meningiomas (17). In addition, dysfunction of the ninth and lower cranial nerves is more common in meningioma than in acoustic neurinoma. Radiologic evaluation with MRI or CT often aids in the differential diagnosis (Fig. 42.3). Meningiomas are less likely to show enlargement of the internal auditory canal. Features on the noncontrast CT scan that suggest meningioma include a lesion that is hyperdense relative to the cerebellum or the presence of calcifications within or at the edge of the tumor. Enhanced MRI or CT may show the presence of a broad attachment to the petrous ridge and may also show involvement of the tentorium or enhancement of the adjacent dura (“dural tail”) (Fig. 42.3C).
Epidermoid Lesions
These lesions, although uncommon and slow growing, tend to envelop rather than displace vascular and neural structures of the cerebellopontine angle. Thus abnormalities of multiple cranial nerves and cerebellar dysfunction are more common in these lesions. The CT scan will show a lesion of lower density than the surrounding brain and with irregular borders. The lesion generally will not enhance with contrast. A combination of CT and MRI greatly facilitates the differential diagnosis (Chapters 4 and 44).
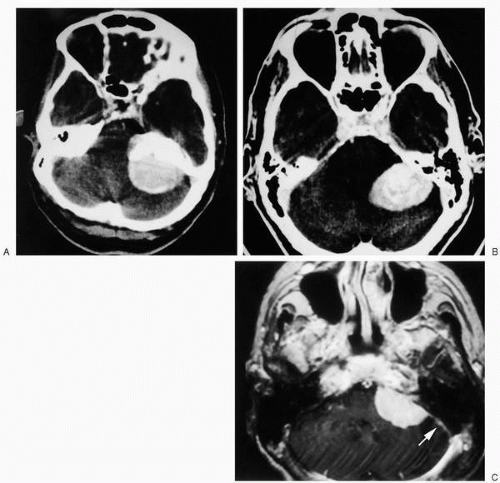 FIG. 42.3 Meningiomas of the petrous apex shown by CT and MRI scan. A: A 56-year-old woman with tinnitus and a normal neurologic and audiometric examination. The lesion was broadly attached to the petrous ridge and demonstrated a rim of calcification. B: Incidental finding on a CT of a 68-year-old man. Characteristic internal calcifications of this petrous ridge meningioma are seen. C: A gadolinium-enhanced MRI of a meningioma of the petrous ridge demonstrates a characteristic “dural tail” (arrow). (A and B from Martuza RL, Parker SW, Nadol JB Jr, et al. Diagnosis of cerebellopontine angle tumors. Clin Neurosurg 1985;32:177-213, with permission.) |
Arachnoid Cyst
The CT scan generally demonstrates a low-density lesion with smooth edges within the internal auditory canal or in the cerebellopontine angle (Figs. 42.4 and 42.5). The density of the lesion is dependent upon the protein content, and enhancement on CT scanning does not occur.
Other Lesions
The differential diagnosis of more unusual lesions of the cerebellopontine angle are well described by Martuza et al. (17). Schwannomas arising from the seventh cranial nerve may present with facial nerve symptoms earlier than in acoustic neurinomas. However, up to 20% of patients with acoustic neurinomas will have facial nerve symptoms and the differential diagnosis may not be made without surgical confirmation of the origin of the lesion. Malignant lesions of the cerebellopontine angle, either primary or metastatic, generally demonstrate rapid progressive symptoms with early cranial nerve involvement and destructive rather than expansile lesions on CT scanning.
BIOLOGY AND NATURAL HISTORY OF ACOUSTIC NEURINOMAS
Pathogenesis
Acoustic neurinomas arise in two clinical settings: the genetic syndrome of neurofibromatosis type 2 and sporadic unilateral acoustic neurinoma. Neurofibromatosis type 2 has now been clearly differentiated from neurofibromatosis type 1 (Von Recklinghausen’s disease) (18).
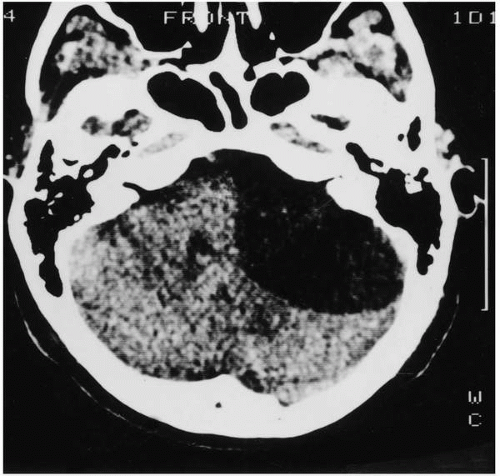 FIG. 42.4 Large arachnoid cyst of the posterior fossa demonstrated by contrast-enhanced CT scan in this 49-year-old woman whose only symptom was tinnitus in the left ear. An audiogram showed slight, low-frequency, conductive loss in the left ear. Auditory evoked response testing was diagnostic of a retrocochlear lesion on the left. (Reprinted with permission from Martuza RL, Parker SW, Nadol JB Jr, et al. Diagnosis of cerebellopontine angle tumors. Clin Neurosurg 1985;32:177-213.) |
Role of the Neurofibromatosis Type 2 Gene in Vestibular Schwannoma Formation
Vestibular schwannomas (acoustic neuromas) occur from mutations in the neurofibromatosis type 2 (NF2) gene (19). The formation of a tumor requires the inactivation of both copies of this gene, either through a chromosomal deletion or through an inactivating mutation. At the molecular level, the genetic abnormalities are at the same locus whether they occur in the unilateral nonhereditary vestibular schwannoma or in the bilateral vestibular schwannoma of the patient with NF2 (20). The difference is at the level of the patient. The patient with NF2 is born with one of the NF2 genes already inactive or missing in every cell of the body. The chance is high—in fact, it is virtually certain—that at some point in his or her lifetime a second inactivating mutation will occur at the same genetic locus; thus bilateral vestibular schwannomas (as well as other tumors, such as meningiomas, schwannomas, and ependymomas) are common and multifocal in NF2 patients (21). Moreover, because one copy of the NF2 gene is abnormal in each germ cell and thus in 50% of each sperm or egg cell, there is a 50% chance of transmitting this disorder to any offspring. In contrast, the patient with a unilateral acoustic neuroma is born with both NF2 genes intact. The odds that both NF2 genes would mutate in the same Schwann cell are so low that the incidence of unilateral acoustic neuroma is low in the general population, and within any individual, he or she is only likely to develop one vestibular schwannoma. Moreover, because the NF2 gene copies are normal in the sperm and egg cells of a patient with a nonhereditary unilateral acoustic neuroma, there is no transmission to offspring.
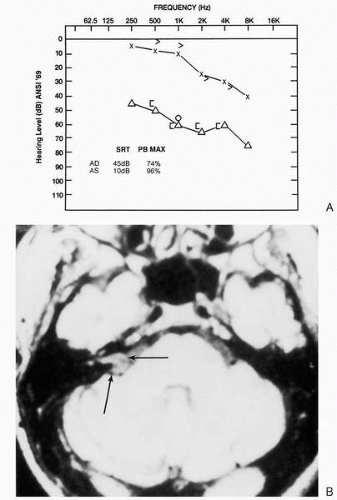 FIG. 42.5 A: Audiogram showing sensorineural loss on the right with reduced speech discrimination. B: MRI scan demonstrating a lesion in the right cerebellopontine angle centered at the internal auditory canal (arrows). This was interpreted radiographically as consistent with acoustic neurinoma but on surgical exploration proved to be an arachnoid cyst. |
Located on the long arm of chromosome 22, the NF2 gene contains 17 exons and produces the protein merlin, a 60- to 70-kDa protein related to the ERM family of proteins, which includes ezrin, radixin, and moesin (22,23). In vitro, the expression of merlin has been shown to be able to inhibit the growth of human meningioma cells (24), to inhibit the growth of NIH-3T3 fibroblasts, (25) and, with overexpression, even to be able to reverse the effects of ras-mediated cell transformation (26). Therefore, functionally, merlin acts like other tumor suppressor genes and its loss would be expected to lead to increased cell growth.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


