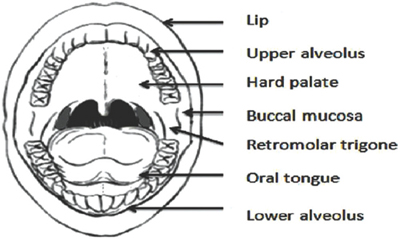
10 Core Messages • Cancers of the lip and oral cavity are unique and occur with the highest frequency in Southeast Asia due to the unique habit of tobacco chewing. • Numerous subsites within the oral cavity have distinct biological features. Proper assessment of the epicenter of the lesions is hence imperative. • There are well-defined premalignant lesions of the lip and oral cavity. • Early stage tumors are usually treated with single modality, with surgery being indicated in the majority. • Locally advanced tumors are treated with combined modality, the treatment being surgery followed by adjuvant radiotherapy/chemoradiation. • The majority of the cancer patients present late and hence emphasis for treatment should be on early detection. • Similarly, treatment outcomes should be improved by providing the modality giving the best possible health-related quality of life. Cancers of the lip and oral cavity rank tenth in the list of cancers prevalent in the world population. Globally, oral cancers account for approximately 405,000 new cases diagnosed each year with two-thirds of them occurring in developing countries (Sri Lanka, India, Pakistan, and Bangladesh).1 In these countries, lip and oral cavity cancer is most commonly seen in men and accounts for 30% of all new cancer cases diagnosed annually. In India, the incidence rate seen in men is 4.5 to 6.1/100,000 but may be as high as 13.9/100,000 in certain regions such as Bhopal.2,3 Oral cancers in the Indian population usually occur a decade earlier compared to the western population, with 60 to 80% of them presenting in an advanced stage (III/IV).4 Cosmesis and important functions such as speech and swallowing are therefore affected both by the disease itself and treatment. Emphasis therefore should be on prevention and early detection to avoid significant impact on health-related quality of life. The oral cavity extends anterior from the skin–vermilion junction of the lips to the junction of the hard and soft palate and the line of circumvallate papillae. It is further subdivided into various subsites, each with a distinct International Classification of Diseases code (Fig. 10.1). Epidemiologically too, oral cavity cancers differ in their prevalence according to the geographical areas with varying patterns of tobacco use. It is imperative for a clinician to identify the epicenter of origin of the cancer as each subsite has a distinct biological behavior and impact for treatment. Extent: The lip begins at the junction of the vermilion border with the skin and includes only the vermilion surface or that portion of the lip that comes into contact with the opposing lip. It is well defined into an upper and lower lip joined at the commissures of the mouth. Lymphatic drainage: Upper lip—Buccal, parotid→prevascular facial nodes→submandibular nodes→upper deep cervical nodes. Lower lip—Submandibular nodes→upper deep cervical nodes. Distinctive features: Cancers of the lip are commonly seen in pipe and cigar smokers. Also, people chronically exposed to harmful ultraviolet rays such as farmers can develop these cancers. These tumors are predominantly treated by surgical excision and require complex reconstruction to provide adequate cosmesis. Extent: Buccal mucosa includes all the membrane lining of the inner surface of the cheeks and lips from the line of contact of the opposing lips to the line of attachment of the mucosa to the alveolar ridge (upper and lower) and pterygomandibular raphe. The membranous lining overlying the ascending ramus of the mandible behind the third molar to the maxillary tuberosity at the apex is known as the “retromolar trigone” and is important oncologically as the tumors involving this region have a propensity for early spread to the infratemporal fossa rendering them unamenable for surgery. Lymphatic drainage: Parotid, submental, submandibular→ upper deep cervical nodes. Distinctive features: In India, buccal mucosa cancers outnumber cancers at all other sites. Gingivobuccal cancers are also known as Indian oral cancer, and constitute 60% of all oral cancers in the country. The site of this cancer is distinctive in view of the placement of the betel quid. Figure 10.1 Anatomic subsites of the oral cavity. Extent: Lower alveolar ridge refers to the mucosa overlying the alveolar process of the mandible which extends from the line of attachment of mucosa in the buccal gutter to the line of free mucosa of the floor of the mouth. It extends to the ascending ramus of the mandible posteriorly. In view of their proximity to the bone, these tumors exhibit early bone erosion and have a higher propensity for early nodal metastasis. Lymphatic drainage: Submental (Ia) and submandibular (Ib). Distinctive features: Gingivobuccal cancers behave differently compared with other subsites of the oral cavity with respect to stage at presentation, propensity for neck metastasis, and recurrence patterns (Table 10.1). Extent: Upper alveolar ridge refers to the mucosa overlying the alveolar process of the maxilla which extends from the line of attachment of the mucosa in the upper gingival buccal gutter to the junction of the hard palate. Its posterior margin is the upper end of the pterygopalatine arch. Lymphatic drainage: Submental (Ia), submandibular (Ib), and retropharyngeal nodes. Table 10.1 Biological Disparity in Oral Cavity Cancers
Cancers of the Lip and Oral Cavity
Relevant Anatomy and Distinctive Features
Lip (C00.0 to C00.9)
Buccal Mucosa (C06.0 to C06.2, C06.7, and C06.8)
Lower Alveolar Ridge (C03.1)
Upper Alveolar Ridge (C03.0)
Parameters | Gingivobuccal Cancers | Tongue/Floor of Mouth Cancers |
Stage at presentation | I and II (13%) III (15%) IV (72%) | I and II (40%) III (33%) IV (27%) |
Propensity for neck metastasis | Low | High |
Metastatic rates | N0: 55–60% N+: 40–45% | N0: 25–30% N+: 70–75% |
First echelon node | Level Ib (submandibular) | Level II (upper jugular) and III (mid jugular) |
Patterns of failure | Predominantly local | Predominantly regional |
Reconstruction | Difficult Composite (mucosa + skin + bone) | Easier Bone and skin rarely involved |
Adapted from reference 5.
Retromolar Gingiva (Retromolar Trigone, C06.2)
Extent: Retromolar gingiva is the attached mucosa overlying the ascending ramus of the mandible from the level of the posterior surface of the last molar teeth to the apex superiorly, adjacent to the tuberosity of the maxilla.
Lymphatic drainage: Submental (Ia) and submandibular (Ib).
Distinctive features: The tumors of this region have a high propensity for nodal metastasis as well as early spread to infratemporal fossa.
Floor of the Mouth (C04.0, C04.1, C04.8, and C04.9)
Extent: This is a semilunar space over the mylohyoid and hyoglossus muscles, extending from the inner surface of the lower alveolar ridge to the undersurface of the tongue. Its posterior boundary is the base of the anterior pillar of the tonsil. It is divided into two sides by the frenulum of the tongue and contains the ostia of the submaxillary and sublingual salivary glands. The mylohyoid muscles attached to the mylohyoid line on the inner surface of the mandible act as a diaphragm between the oral cavity and neck, and serve as an important landmark in therapeutic decision making.
Lymphatic drainage: Submental (Ia) and submandibular nodes (Ib).
Distinctive feature: Floor of the mouth cancers have high propensity for early nodal metastasis (unilateral and contralateral).
Hard Palate (C05.0)
Extent: Hard palate is the semilunar area between the upper alveolar ridge and the mucous membrane covering the palatine process of the maxillary palatine bones. It extends from the inner surface of the superior alveolar ridge to the posterior edge of the palatine bone.
Lymphatic drainage: Retropharyngeal nodes→deep cervical nodes.
Distinctive features: The mucosa overlying the hard palate closely adheres to the underlying periosteum by regularly arranged Sharpey fibers. This mucosa also contains numerous minor salivary glands which may give rise to minor salivary gland tumors. The hard palate is the most common site for the occurrence of adenoid cystic carcinomas.
Anterior Two-Thirds of the Tongue (Oral Tongue, C02.0 to C02.3, C02.8, and C02.9)
Extent: The anterior two-thirds of the tongue is the freely mobile portion of the tongue that extends anteriorly from the line of the circumvallate papillae to its undersurface at the junction of the floor of the mouth. It is composed of four areas: the tip, the lateral borders, the dorsum, and the undersurface (nonvillous ventral surface of the tongue). The undersurface of the tongue is considered a separate category by the World Health Organization (WHO).
Lymphatic drainage: Tip—submental nodes (Ia), rest of the tongue: submandibular nodes (Ib).
Distinctive features: Anterior two-thirds of the tongue plays an important part in the functions of speech and swallowing (Phases I and II). Hence, any surgery involving excision of the tongue musculature has a direct bearing on the functional outcomes for the patient. Tongue cancers have a higher propensity for nodal metastasis (ipsilateral and contralateral) in view of the abundant vascularity of the organ. The surgery of these tumors usually encompasses a bilateral neck dissection to improve locoregional control. Also, a higher incidence of occult metastasis is seen in tongue cancers ranging from 20 to 40%.4
Epidemiology
Globally, oral cancers account for approximately 405,000 new cases diagnosed each year with two-thirds of them occurring in developing countries (Sri Lanka, India, Pakistan, and Bangladesh).5 In these countries oral cancer is the most common cancer in men and accounts for 30% of all new cancer cases annually (Fig. 10.2).
Etiological Factors
The oral cavity by virtue of its function is exposed to a variety of carcinogenic or potentially carcinogenic substances. The most common etiological agents are depicted in Fig. 10.3 and briefly described below.
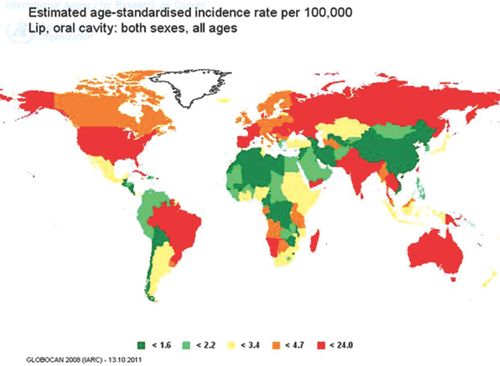
Figure 10.2 World age-standardized incidence rates of men for lip and oral cavity cancers (2008 estimates).
Source: http://globocan.iarc.fr/map.
Tobacco and Tobacco Products
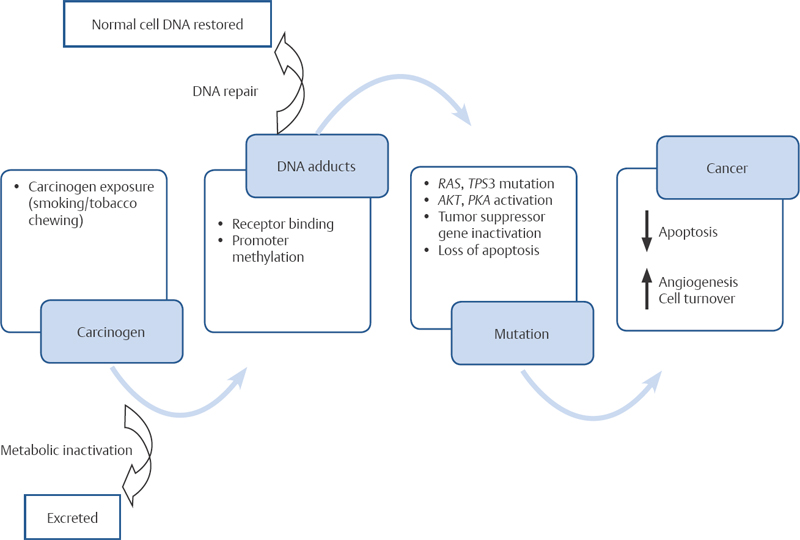
Tobacco is the single most important factor implicated in the etiology of oral cancers. Globally, tobacco is responsible for the death of 1 in 10 adults (5 million deaths per year) with 2.41 (1.80 to 3.15) million deaths in the developing countries and 2.43 (2.13 to 2.78) million deaths in the developed countries. Evidence from the population-based registry in India has shown that tobacco is responsible for 50% of the cancers seen in the Indian population. Tobacco is a mixture of carcinogenic compounds such as polycyclic aromatic hydrocarbons and nitrosamines. Tobacco is consumed in different forms, viz., tobacco smoking and smokeless forms (Fig. 10.4 and Table 10.2). The oral use of smokeless tobacco is widely prevalent in India; its different methods of consumption include chewing, sucking, and applying tobacco preparations to the teeth and gums. Smokeless tobacco products are often made at home but are also manufactured. Tobacco carcinogenesis is a multistep process6 and is depicted in Fig. 10.5.
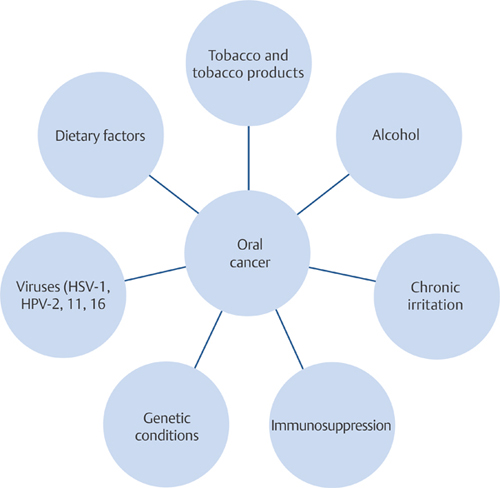
Figure 10.3 Common etiological agents for oral cavity cancer. HPV, human papillomavirus; HSV, herpes simplex virus.

Alcohol
In the work of McCoy and Wynder, strong evidence exists to support the concept of synergistic activity of alcohol with tobacco.7 The proposed mechanisms for alcohol cocarcinogenesis are shown in Fig. 10.5 and Table 10.3.
Dietary Factors
Although there has been no conclusive study to correlate dietary deficiency with carcinogenicity, a few studies have shown a protective function of vitamin A in preventing cancer.8
Chronic Irritation
Various studies have analyzed the role of chronic irritation in carcinogenesis. Factors which have been implicated to date include poor oral and dental hygiene, sharp tooth, ill-fitting dentures, syphilis, chronic mouthwash usage, and marijuana consumption.9–11
Viruses
Viruses such as herpes simplex virus and human papillomavirus (HPV)-2, 11, and 16 have been suspected to cause oral cancers; but to date no definite proof has been found.12,13
Immunosuppression
HIV-infected patients are more prone to develop Kaposi sarcoma and non-Hodgkin lymphoma (NHL) in the oral cavity. Kaposi sarcoma is associated with human herpesvirus 8 while NHL is with Epstein-Barr virus.14 Similarly, immunosuppression associated with kidney transplantation and bone marrow transplant has been implicated in the development of oral cancer.15
Table 10.2 Different Forms of Tobacco Consumption
Smokeless | Tobacco Smoking |
Paan (betel quid) with tobacco | Beedis |
Paan masala | Cigarette |
Mainpuri tobacco | Cigar |
Mawa | Cheroot |
Tobacco and slaked lime (khaini) | Chuttas (reverse smoking) |
Chewing tobacco | Dhumtis |
Pipe | |
Hookah | |
Hooklis | |
Chillum |
Genetic Factors
Patients having genetic mutations which affect the process of deoxyribonucleic acid repair, viz, xeroderma pigmentosum, Fanconi anemia, and ataxia telangiectasia are more prone to develop oral cancers.16
Pathology
The oral cavity is involved with a variety of pathologies, both benign and malignant. Among the malignant lesions described by the WHO, 95% are squamous cell carcinomas (SCCs) (Table 10.4).
Potentially Malignant Lesions of the Lip and Oral Cavity
The WHO in 2005 modified the terminology, definitions, and classification of oral lesions with a predisposition to malignant transformation and proposed the term “potentially malignant” for “premalignant” or “precancerous” lesions.17 Also, it recommended abandoning the traditional distinction between potentially malignant lesions and potentially malignant conditions and using the term “potentially malignant disorders” instead.17 The potentially malignant lesions of the oral cavity include leukoplakia, erythroleukoplakia, and submucous fibrosis (SMF).
Table 10.3 Proposed Mechanism of Alcohol Co-Carcinogenesis
Local Effects | Systemic Effects |
Solvent for potential carcinogens | Alcohol metabolism—acetaldehyde |
Mucosa injury-aids carcinogen uptake | Production of other free radicals |
Acetaldehyde production by oral bacteria | Chronic alcoholics • CYP2E1 enzyme induction • Nutritional deficiencies |
Carcinogenic impurities | Altered retinoid metabolism |
Chronic alcoholics • Poor salivary flow • Gastroesophageal reflux | • Reduced immune surveillance |
Table 10.4 World Health Organization Classification for Oral Cavity Lesions
A. Epithelial Tumors | |
Malignant epithelial tumors | |
a. Squamous cell carcinoma | |
• Verrucous carcinoma | |
• Basaloid squamous cell carcinoma | |
• Papillary squamous cell carcinoma | |
• Spindle cell carcinoma | |
• Acantholytic squamous cell carcinoma | |
• Adenosquamous carcinoma | |
• Carcinoma cuniculatum | |
Epithelial precursor lesions | |
Benign epithelial tumors | |
a. Papillomas | |
• Squamous cell papilloma and verruca vulgaris | |
• Condyloma acuminatum | |
• Focal epithelial hyperplasia | |
b. Granular cell tumor | |
c. Keratoacanthoma | |
B. Salivary Gland Tumors | |
a. Salivary gland carcinomas | 8050/0 |
• Acinic cell carcinoma | 8550/3 |
• Mucoepidermoid carcinoma | 8430/3 |
• Adenoid cystic carcinoma | 8200/3 |
• Polymorphous low-grade adenocarcinoma | 8525/3 |
• Basal cell adenocarcinoma | 8147/3 |
• Epithelial–myoepithelial carcinoma | 8562/3 |
• Clear cell carcinoma, not otherwise specified | 8310/3 |
• Cystadenocarcinoma | 8450/3 |
• Mucinous adenocarcinoma | 8480/3 |
• Oncocytic carcinoma | 8290/3 |
• Salivary duct carcinoma | 8500/3 |
• Myoepithelial carcinoma | 8982/3 |
• Carcinoma ex pleomorphic adenoma | 8941/3 |
b. Salivary gland adenomas | 8050/0 |
• Pleomorphic adenoma | 8940/0 |
• Myoepithelioma | 8982/0 |
• Basal cell adenoma | 8147/0 |
• Canalicular adenoma | 8149/0 |
• Duct papilloma | 8503/0 |
• Cystadenoma | |
C. Soft Tissue Tumors | |
Kaposi sarcoma | 9140/3 |
Lymphangioma | 9170/0 |
Ectomesenchymal chondromyxoid tumor | |
Focal oral mucinosis | |
Congenital granular cell epulis | |
D. Hematolymphoid Tumors | |
DLBCL | 9680/3m |
Mantle-cell lymphoma | 9673/3 |
Follicular lymphoma | 9690/3 |
Extranodal marginal zone B-cell lymphoma of MALT type | 9699/3 |
Burkitt lymphoma | 9687/3 |
T-cell lymphoma (including anaplastic large cell lymphoma) | 9714/3 |
Extramedullary plasmacytoma | 9734/3 |
Langerhans cell histiocytosis | 9751/1 |
Extramedullary myeloid sarcoma | 9930/3 |
Follicular dendritic-cell sarcoma/tumor | 9758/3 |
E. Mucosal Malignant Melanoma | |
F. Tumors of Bone | |
Odontogenic carcinomas | |
• Metastasizing (malignant) ameloblastoma | 9310/3 |
• Ameloblastic carcinoma–primary type | 9270/3 |
• Ameloblastic carcinoma–secondary type (dedifferentiated), | 9270/3 |
• Intraosseous | |
• Ameloblastic carcinoma–secondary type (dedifferentiated), | 9270/3 |
• Peripheral | |
• Primary intraosseous squamous cell carcinoma – solid | 9270/3 |
• Type | |
• Primary intraosseous squamous cell carcinoma derived from keratocystic odontogenic tumor | 9270/3 |
• Primary intraosseous squamous cell carcinoma derived from odontogenic cysts | 9270/3 |
• Clear cell odontogenic carcinoma | 9341/3 |
• Ghost cell odontogenic carcinoma | 9302/3 |
• Odontogenic sarcomas | |
• Ameloblastoma fibrosarcoma | 9330/3 |
• Ameloblastic fibrodentino and fibro-odontosarcoma | 9290/3 |
G. Secondary Tumors | |
DLBCL, diffuse large B-cell lymphoma; MALT, mucosa-associated lymphoid tissue.
Leukoplakia
Leukoplakia is defined as “a white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer” (Fig. 10.6).17 Globally, the estimated reported prevalence of oral leukoplakia is approximately 2%.18 Whereas, the annual malignant transformation rate is 1%, resulting in development of oral cancer in 20 per 100,000 people per year. Leukoplakia is six times more common among smokers compared with nonsmokers.19 Alcohol is an independent risk factor, regardless of beverage type or drinking pattern.20 The role of HPV is still being explored.20–22

Figure 10.6 Leukoplakia seen on the (A) buccal mucosa and (B) tongue.
Clinically, leukoplakia is divided into two types.
1. Homogeneous type (flat, thin, uniform white in color)
2. Nonhomogeneous type
The nonhomogeneous type has been defined as a white and red lesion (“erythroleukoplakia”), that may be either irregularly flat (speckled) or nodular. Verrucous leukoplakia is yet another type of nonhomogeneous leukoplakia. Although verrucous leukoplakia usually has a uniform white appearance, its verrucous texture distinguishes it from homogeneous (flat) leukoplakia. Verrucous leukoplakia is clinically difficult to distinguish from verrucous carcinoma. Proliferative verrucous leukoplakia (PVL) is another subtype of verrucous leukoplakia, characterized by multifocal presentation, resistance to treatment and a high rate of malignant transformation.17,18,20 PVL is more prevalent in elderly women and there may be no history of tobacco use. The risk factors associated with an increased rate of malignant transformation are represented in Table 10.5. Clinical and histological classification is shown in Tables 10.6 and 10.7.23
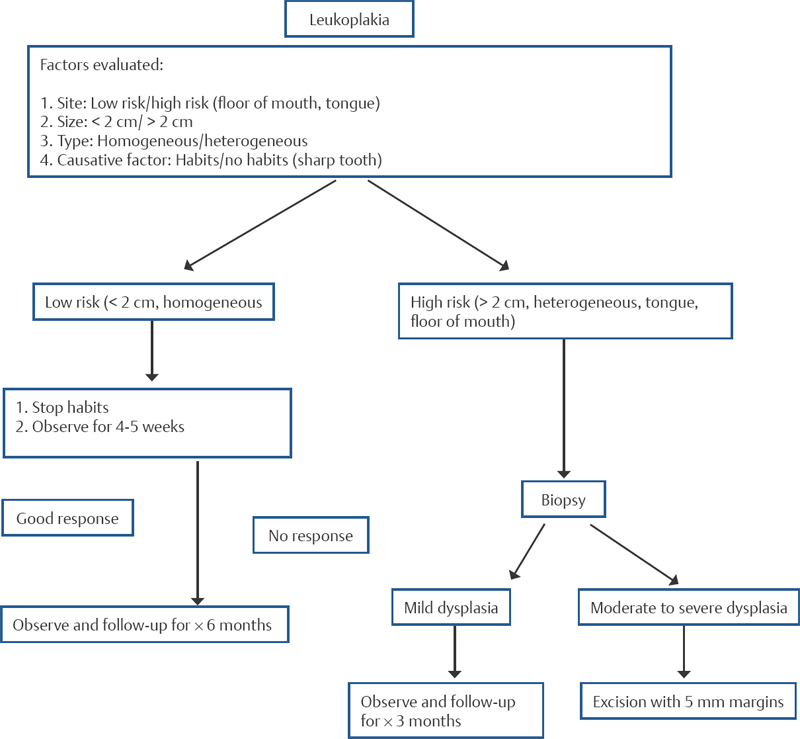
Biopsy or excision is preferable for the diagnosis and prevention of malignant transformation. The management algorithm for leukoplakia is shown in Fig. 10.7.24
Erythroplakia
Erythroplakia is defined as a “bright red velvety patch that cannot be characterized clinically or pathologically as being caused by any other condition.” Histologically, erythroplakia exhibits some degree of dysplasia and may even have foci of carcinoma in situ. Higher rates (68%) of aneuploidy are seen in erythroplakic lesions and serve as a surrogate marker for malignant transformation. Surgical excision is the treatment of choice for this pathology.
Table 10.5 High Risk Factors for Malignant Transformation
Females |
Long duration of leukoplakia |
Location on the tongue or floor of mouth17 |
Leukoplakia in nonsmokers |
Nonhomogeneous (speckled/nodular) type |
Presence of dysplastic changes |
Presence of Candida albicans |
Molecular markers (loss of heterozygosity at loci 3p14 and 9p21, expression of a novel molecule podoplanin, suprabasal expression of p53, presence of high-risk HPV 16, immunohistochemistry pattern of cyclin D1, p27 and p63, and the expression of cytokeratin 8.66–70 |
HPV, human papillomavirus.
Table 10.6 World Health Organization Histological Classification that Histologically Categorizes Precursor and Related Lesions
WHO Classification | SIN | Ljubljana Classification of SIN |
Squamous cell hyperplasia | Squamous cell (simple) hyperplasia | |
Mild dysplasia | SIN 1 | Basal/parabasal cell hyperplasia |
Moderate dysplasia | SIN 2 | Atypical hyperplasia |
Severe dysplasia | SIN 3c | Atypical hyperplasia |
Carcinoma in situ | SIN 3c | Carcinoma in situ |
Adapted from reference 23.
WHO, World Health Organization; SIN, squamous intraepithelial neoplasia.
Table 10.7 Classification and Staging System for Oral Leukoplakias (OL-System)
L (size of leukoplakia) |
• Lx: Size not specified |
• L1: Single/multiple (< 2 cm) |
• L2: Single/multiple (2–4 cm) |
• L3: Single/multiple (> 4 cm) |
P (pathologic features) |
• Px: Absence/presence of epithelial dysplasia not reported |
• P0: No epithelial dysplasia |
• P1: Mild/moderate dysplasia |
• P2: Severe dysplasia |
OL-staging system |
• Stage I: L1P0 |
• Stage II: L2P0 |
• Stage III: L3P0 or L1/2P1 |
• Stage IV: L3P1 or any L P2 |
Lichen Planus
Lichen planus clinically presents as lacy white lines on a violaceous background on the buccal mucosa, often accompanied by symptoms of pain and burning sensations (Fig. 10.8). Histologically, it is characterized by band-like subepithelial mononuclear infiltrate of T cells and histiocytes and degenerating basal keratinocytes that form colloid bodies. This pathology has an annual malignant transformation rate of 1%.25
Oral Submucous Fibrosis
Oral submucous fibrosis (OSMF) is caused by chronic exposure to betel nut and tobacco. This pathology is characterized by a generalized dense scarring of the oral soft tissue resulting in trismus. Histological findings vary according to the stage of the disease and include subepithelial fibrosis, chronic inflammation, hyalinization, and loss of vascularity. The annual malignant transformation rate is approximately 0.5%.26
Natural History of Oral Squamous Cell Carcinoma (Genetic Progression Model)
Oral carcinogenesis is a multistep process that involves biomolecular changes brought by carcinogens leading to premalignant changes which in turn lead to malignancy. It was Slaughter who first described the concept of “field cancerization” wherein multiple carcinogenic insults to the mucosa of the upper aerodigestive tract lead to alteration in the molecular milieu of the lining cells.27,28 These mutations result in development of a progeny that has the ability of uncontrolled cell division, eventually developing into malignancy. This theory also provides insight into the development of second primaries in this region. Development of a second primary is the main cause of mortality in early-stage oral cancers. The genetic model of carcinogenesis is depicted in Fig. 10.9.
Site Distribution
The site distribution of oral cavity cancer is in direct correlation with the regions that are maximally exposed to carcinogens, for example, gingivobuccal sulcus.4 It is these areas where salivary stagnation occurs exposing the mucosa to tremendous carcinogenic insults.29 Great disparity exists in the distribution of oral cancer sites among developing and developed countries, and the answer lies in the difference in habits peculiar to the population, i.e. chewing vs. smoking tobacco, (Fig. 10.10).
Regional Metastasis
Cervical lymph node metastasis is considered the single most important prognostic factor in oral cavity SCC. The 5-year survival reduces to approximately 50% after development of nodal metastasis.30 The site of nodal metastasis depends on the primary subsite, T stage, and histopathological features. Lymphatic spread from a tumor follows a step-wise orderly pattern. The nodal metastasis seen at different sites is depicted in Table 10.8 and Figs. 10.11.1 to 10.11.4.
Diagnosis
Clinical Evaluation
A detailed clinical history should be obtained from the patient presenting with an oral cavity lesion. The patient should be inquired regarding his addictions (tobacco, alcohol, etc.) with the aim of identifying the possible risk factors. Similarly, a detailed family history should be elicited to rule out any genetic susceptibility conditions. Patients having comorbid (such as conditions (diabetes, cardiac problems, or asthma) should be evaluated with regard to the current disease status and a physician referral should be obtained in case of derangements. The clinical examination should also include, apart from the oral cavity, 90 degree Hopkins telescopy to rule out a second primary and document vocal cord status along with a detailed evaluation of the neck to detect neck metastasis. Patients presenting with trismus and advanced disease who are not amenable for routine clinical evaluation should be examined under anesthesia to map the tumor extent and plan the required therapeutic approach. The symptomatology of each subsite of the oral cavity is unique and is briefly described in Table 10.9.
< div class='tao-gold-member'>